Bridge Plating for High-Energy Distal Radius Fractures: An Intraoperative Masterclass

Key Takeaway
This masterclass guides fellows through bridge plating high-energy distal radius fractures. We cover detailed surgical anatomy, meticulous preoperative planning, and a step-by-step intraoperative execution, emphasizing indirect reduction and plate insertion techniques. Crucial pearls on avoiding neurovascular injury, managing intra-articular fragments, and assessing DRUJ stability are discussed. Postoperative care and complication management ensure comprehensive understanding for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
The management of high-energy distal radius fractures represents a formidable challenge even for the most seasoned orthopedic trauma surgeon. Unlike the classic low-energy Colles fracture typically seen in the osteoporotic elderly population, high-energy variants are characterized by massive axial loading, violent sheer forces, and severe torsional stress. These mechanisms result in profound metaphyseal comminution, diaphyseal extension, and catastrophic disruption of the articular surface. The energy imparted to the bone frequently shatters the scaphoid and lunate facets, creating independent, rotated, and impacted osteochondral fragments that defy traditional methods of direct reduction. In these scenarios, the soft tissue envelope is equally traumatized, precluding extensive open surgical approaches that would further devitalize the precarious blood supply to the metaphyseal fragments.
Historically, external fixation was the gold standard for managing these highly comminuted, unstable fracture patterns. The principle relied on ligamentotaxis—utilizing the intact volar radiocarpal ligaments to pull the articular fragments back into alignment through longitudinal distraction. However, external fixation is fraught with complications, including pin tract infections, loss of reduction due to pin loosening, radial sensory nerve irritation, and significant patient dissatisfaction due to the cumbersome nature of the frame. While standard volar locking plates (VLP) revolutionized the treatment of extra-articular and simple intra-articular fractures, they frequently fail in the setting of severe metaphyseal-diaphyseal comminution. The screws lack adequate bone purchase in the "void" of the shattered metaphysis, leading to secondary subsidence, loss of volar tilt, and eventual hardware failure.
Enter the concept of dorsal bridge plating, essentially an "internal external fixator." This technique, refined over the past two decades, offers a robust, elegant solution by providing strong, spanning fixation from the intact radial diaphysis to the second or third metacarpal. By bypassing the zone of injury entirely, the bridge plate allows for indirect reduction via ligamentotaxis while eliminating the morbidities associated with external pins. It acts as a load-bearing device, neutralizing axial, bending, and torsional forces across the radiocarpal joint. This is a game-changer for maintaining reduction and restoring critical wrist anatomy, especially in polytraumatized patients who require immediate weight-bearing through the upper extremity to facilitate mobilization with crutches or transfers.
Anatomical restoration of the distal radius is paramount for superior functional outcomes; anything less inevitably leads to altered wrist kinematics, persistent pain, weakness, and rapid-onset post-traumatic radiocarpal and midcarpal arthrosis. The bridge plating technique allows the surgeon to harness the power of distraction without the biological insult of a massive open reduction. By preserving the fracture hematoma and the periosteal blood supply, we optimize the biological environment for secondary bone healing (callus formation) in the comminuted metaphysis. Today, we will deconstruct this procedure step-by-step, providing an intraoperative masterclass on how to execute this technique with precision, safety, and biomechanical sound reasoning.

Detailed Surgical Anatomy and Biomechanics
Before a single incision is made, a profound understanding of the complex osteology, ligamentous anatomy, and neurovascular topography of the wrist is non-negotiable. The distal radius is a marvel of biomechanical engineering, often conceptualized as a three-column structure (radial, intermediate, and ulnar columns) as described by Rikli and Regazzoni. The articular surface is typically tilted 21 degrees in the anteroposterior plane (volar tilt) and 11 degrees in the lateral plane (radial inclination), with an average radial height of 11-12 mm relative to the distal ulna. This precise geometry is essential for normal load transmission across the wrist, where approximately 80% of the axial load passes through the radiocarpal joint and 20% through the ulnocarpal axis. High-energy fractures frequently obliterate this geometry, creating sagittal or coronal splits that uncouple the scaphoid and lunate facets.
The principle of ligamentotaxis, which bridge plating heavily relies upon, is entirely dependent on the integrity of the volar extrinsic radiocarpal ligaments. The radioscaphocapitate (RSC) ligament, the long radiolunate (LRL) ligament, and the short radiolunate (SRL) ligament are robust structures that originate from the volar margin of the distal radius and insert onto the carpus. When longitudinal traction is applied to the hand, these ligaments become taut, acting as a tension band that pulls the displaced articular fragments of the radius distally and palmarly, indirectly restoring the volar tilt and radial height. It is critical to understand that ligamentotaxis cannot reduce central "die-punch" fragments, as these lack soft tissue attachments; such fragments may require supplementary percutaneous manipulation or limited open reduction.
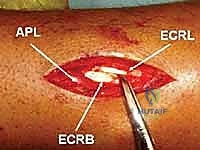
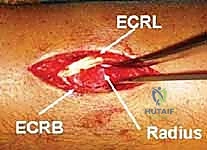
Navigating the dorsal aspect of the wrist requires meticulous attention to the extensor compartments. The extensor retinaculum is divided into six distinct compartments. Our surgical approach leverages the natural interval between the second and third compartments. The second dorsal compartment houses the extensor carpi radialis longus (ECRL) and extensor carpi radialis brevis (ECRB), which insert onto the bases of the second and third metacarpals, respectively. The third compartment contains the extensor pollicis longus (EPL), which hooks around the tubercle of Lister—a crucial bony landmark on the dorsal radius. Proximally, the first compartment contains the abductor pollicis longus (APL) and extensor pollicis brevis (EPB), collectively known as the "outcroppers," which cross obliquely over the ECRL and ECRB. Our bridge plate must be passed extraperiosteally, gliding beneath the outcroppers and between the ECRL and ECRB to prevent tendon attrition.
Equally critical is the preservation of the neurovascular structures, most notably the Superficial Radial Nerve (SRN). The SRN emerges from beneath the brachioradialis tendon approximately 9 cm proximal to the radial styloid, piercing the deep fascia to become subcutaneous. It branches extensively over the dorsal-radial aspect of the wrist and hand. Iatrogenic injury to the SRN during the proximal incision or during subcutaneous tunneling can result in debilitating neuromas and Complex Regional Pain Syndrome (CRPS). The radial artery, while located more volarly, can be at risk during aggressive radial-sided dissection or errant drilling. Maintaining a strict extraperiosteal plane during plate insertion is the ultimate safeguard against these catastrophic neurovascular and tendinous complications.
Exhaustive Indications and Contraindications
The decision to utilize a dorsal spanning bridge plate must be carefully weighed against alternative fixation strategies. The primary indication for bridge plating is a highly comminuted, high-energy distal radius fracture where the metaphyseal bone stock is insufficient to support standard volar or dorsal locked plating. This includes fractures with extensive diaphyseal extension, severe osteopenia where screw pull-out is a certainty, and massive articular comminution where direct open reduction would necessitate unacceptable soft tissue stripping. In these scenarios, the bridge plate acts as a load-sharing device, maintaining length, alignment, and rotation while the metaphyseal void heals via secondary intention.
Polytrauma patients represent a highly specific and critical indication for bridge plating. Patients with concomitant lower extremity injuries, pelvic ring disruptions, or spinal trauma often require the immediate use of their upper extremities for crutch weight-bearing, wheelchair transfers, or bed mobility. A standard volar plate or a cast cannot withstand the immense axial loads generated during these activities, leading to catastrophic hardware failure or loss of reduction. A robust 2.4mm or 2.7mm dorsal spanning plate anchored securely in the radial diaphysis and the second or third metacarpal provides the biomechanical stability necessary to permit immediate, full weight-bearing through the injured limb, thereby expediting the patient's overall rehabilitation and preventing the systemic complications of prolonged bed rest.
Radiocarpal fracture-dislocations and severe carpal instability patterns associated with distal radius fractures also serve as excellent indications. In cases where the radiocarpal ligaments are severely compromised or avulsed with small bony fragments, the spanning plate acts as an internal splint, neutralizing the deforming forces of the extrinsic flexors and extensors. By holding the carpus in strict anatomical alignment relative to the radius for 12 to 16 weeks, the plate allows the capsuloligamentous structures to heal in an isometric position, preventing chronic radiocarpal subluxation or late carpal collapse.
Conversely, absolute contraindications are relatively few but critical to observe. Active infection at the surgical site or severe soft tissue compromise (such as a massive degloving injury or severe burns over the dorsal wrist) precludes the use of internal hardware. Relative contraindications include fractures that can be adequately and stably fixed with a standard volar locking plate, as bridge plating necessitates a mandatory secondary surgery for hardware removal and temporarily sacrifices wrist motion. Additionally, pre-existing stiff wrist conditions or severe baseline radiocarpal arthritis may make the subsequent rehabilitation following prolonged immobilization exceedingly difficult, requiring careful preoperative counseling.
| Parameter | Indications for Dorsal Bridge Plating | Contraindications |
|---|---|---|
| Fracture Pattern | Severe metaphyseal/diaphyseal comminution; bone loss; radiocarpal fracture-dislocations. | Simple extra-articular fractures; reducible intra-articular fractures amenable to VLP. |
| Patient Profile | Polytrauma requiring upper extremity weight-bearing; severe osteoporosis. | Low-demand patients adequately managed with casting (relative). |
| Soft Tissue Status | Intact dorsal soft tissue envelope; severe volar soft tissue injury precluding VLP. | Active dorsal infection; massive dorsal soft tissue degloving/burns. |
| Logistical Factors | Patient agreeable to mandatory secondary surgery for plate removal. | Patient medically unfit for a secondary elective surgery. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the bedrock of a successful bridge plating procedure. The process begins with a rigorous review of high-quality imaging. Standard posteroanterior (PA), lateral, and oblique radiographs provide a baseline understanding of the fracture pattern, radial shortening, and loss of volar tilt. However, for high-energy injuries, a non-contrast Computed Tomography (CT) scan with 3D reconstructions is absolutely indispensable. The CT scan serves as a surgical roadmap, revealing the hidden complexities of the injury: the exact number and orientation of intra-articular fragments, the presence of impacted central die-punch fragments, the integrity of the distal radioulnar joint (DRUJ), and the extent of diaphyseal propagation. This advanced imaging allows the surgeon to mentally rehearse the reduction maneuvers and anticipate the need for supplementary percutaneous wire fixation or bone grafting.
Templating the hardware is the next critical step. The surgeon must determine the appropriate plate length and trajectory before entering the operating room. We typically utilize a 22-hole or 24-hole 2.4mm titanium mandibular reconstruction plate or a dedicated 2.4mm/2.7mm distal radius bridge (DRB) plate. The plate must be long enough to span from the healthy radial diaphysis (requiring at least 6 to 8 cortices of secure fixation proximal to the fracture) to the distal metadiaphysis of the second or third metacarpal (requiring 6 cortices of fixation). Dedicated DRB plates often feature tapered ends, which significantly facilitate the blind extraperiosteal passage beneath the outcropper muscles and extensor retinaculum, minimizing soft tissue trauma.
Patient positioning and operating room setup must be optimized to allow for seamless fluoroscopic imaging and unobstructed access to the limb. The patient is placed in the supine position under general anesthesia or a high-quality regional brachial plexus block. The involved extremity is prepped and draped free, then positioned on a radiolucent hand table. A sterile tourniquet is applied to the proximal arm but is typically not inflated until the initial closed reduction maneuvers are completed, allowing for better assessment of the limb's vascular status during traction. The C-arm fluoroscopy unit is positioned either parallel or perpendicular to the hand table, ensuring it can easily arc to obtain true AP, lateral, and oblique views without contaminating the sterile field or requiring awkward manipulation of the fractured limb.
The application of longitudinal traction is the final preparatory step and is often therapeutic in itself. We utilize sterile finger traps applied to the index and middle fingers. Adequate padding must be placed around the digits to prevent skin necrosis or nerve compression. The finger traps are connected to a rope and pulley system at the end of the hand table, and approximately 10 to 15 pounds (4.5 to 6.8 kg) of longitudinal traction is applied. A counter-traction strap is placed across the distal humerus. This initial traction is crucial; it overcomes the deforming forces of the forearm musculature, restores radial length, and allows the surgeon to assess the efficacy of ligamentotaxis in real-time via fluoroscopy, setting the stage for the formal reduction maneuvers.


Step-by-Step Surgical Approach and Fixation Technique
With the patient prepped, traction applied, and the surgical team ready, we commence the intraoperative execution. The first objective is to achieve the best possible closed reduction under traction, utilizing the Agee maneuver. This technique is a calculated combination of forces designed to restore length, sagittal tilt, and correct rotational deformities without opening the fracture site. As the initial 4.5 to 6.8 kg of traction is applied, we observe the wrist under fluoroscopy. The longitudinal pull utilizes the intact volar ligaments to drag the distal articular fragments out of their impacted, shortened position.


Once length is restored, the surgeon performs palmar translation of the carpus relative to the forearm. By pushing the carpus volarly, the tension on the dorsal radiocarpal ligaments increases, which helps to indirectly hinge the dorsal articular fragments back into place, thereby restoring the crucial volar tilt. Finally, the hand is gently pronated relative to the forearm to correct the supination deformity that frequently accompanies high-energy distal radius fractures. These maneuvers are confirmed with AP and lateral fluoroscopy. It is imperative not to force the reduction; excessive manipulation can further comminute fragments. The goal is an acceptable alignment that the bridge plate will subsequently lock into place.


Following the Agee maneuver, we plan our incisions and plate trajectory. The chosen DRB plate is superimposed on the skin over the dorsal radial aspect of the forearm and hand. The plate should extend from the mid-radial diaphysis to the base of the second metacarpal. Fluoroscopy is used to confirm that the plate length is adequate to provide at least three bicortical screws (six cortices) in healthy bone both proximally and distally. We mark a 3-4 cm longitudinal incision distally over the index metacarpal and a second 4-5 cm longitudinal incision proximally over the radial diaphysis, ensuring the proximal incision is safely away from the fracture hematoma.


The distal incision is made first, carefully dissecting down to the dorsal surface of the second metacarpal. The extensor hood is identified, and the interval between the ECRL and the extensor digitorum communis (EDC) to the index finger is developed. The periosteum of the metacarpal is incised and minimally elevated. Next, the proximal incision is made. Extreme caution must be exercised here to identify and protect the Superficial Radial Nerve (SRN) and the cephalic vein. The interval between the brachioradialis and the ECRL is developed to expose the radial diaphysis.

Now comes the most critical step: tunneling the plate. Using a blunt elevator or a dedicated tunneling instrument, an extraperiosteal path is created from proximal to distal. The instrument must pass beneath the muscle bellies of the outcroppers (APL and EPB) and beneath the extensor retinaculum, staying deep to the ECRL and ECRB tendons. Blind passage without maintaining contact with the bone can lead to devastating tendon interposition or neurovascular injury. Once the tunnel is established, the tapered bridge plate is slid from proximal to distal.

Fixation begins distally. The plate is centered over the second metacarpal, and three non-locking or locking 2.4mm screws are inserted bicortically. With the distal end secured, attention turns to the proximal fixation. While maintaining the traction and the Agee reduction maneuver, the plate is secured to the radial diaphysis. The first proximal screw is often placed in compression mode to tension the construct and maximize ligamentotaxis. Subsequently, two to three additional locking screws are placed proximally. Final fluoroscopic images are obtained in multiple planes to confirm the restoration of radial height, volar tilt, articular congruity, and the extra-articular trajectory of all screws.




Complications, Incidence Rates, and Salvage Management
While bridge plating is a highly effective technique, it is not without significant risks. The most frequent complication is iatrogenic injury to the Superficial Radial Nerve (SRN). The SRN's highly variable branching pattern makes it exquisitely vulnerable during the proximal incision and the subsequent subcutaneous dissection. Injury can range from a transient neuropraxia due to traction, to a complete transection resulting in a painful neuroma. Meticulous surgical technique, utilizing blunt dissection and loupe magnification, is the only way to mitigate this risk. If an SRN neuroma develops, salvage management may require surgical excision of the neuroma and burying the nerve stump into the brachioradialis muscle belly.
Tendon complications represent another major category of morbidity. Extensor tendon tenosynovitis or frank rupture can occur if the plate is not placed strictly extraperiosteally. If the plate is inadvertently passed over the outcroppers (APL/EPB) or if it rubs against the EPL or EDC tendons, the mechanical attrition will inevitably lead to tendon failure. The incidence of tendon rupture is significantly reduced by using modern, low-profile plates and ensuring meticulous tunneling deep to the muscle bellies. Should a rupture occur, salvage typically requires tendon transfer procedures, such as transferring the extensor indicis proprius (EIP) to the EPL.
Bone healing complications, while less common than with external fixation, still occur. Malunion can result if the initial indirect reduction was inadequate or if the plate was tensioned improperly, failing to restore volar tilt or radial height. Nonunion is rare due to the preservation of the fracture hematoma, but it can occur in cases of massive bone loss or severe thermal injury to the periosteum. Management of a symptomatic malunion or nonunion necessitates a complex secondary reconstruction, often involving a corrective osteotomy, structural bone grafting (e.g., iliac crest), and revision internal fixation, which carries a high morbidity profile.
Complex Regional Pain Syndrome (CRPS) and profound wrist stiffness are the functional enemies of this procedure. Because the radiocarpal joint is immobilized for 12 to 16 weeks, capsular contracture is guaranteed. While most patients regain functional motion with aggressive post-operative therapy, a subset will develop debilitating stiffness. CRPS, characterized by disproportionate pain, autonomic dysfunction, and trophic changes, requires aggressive multimodal management, including sympathetic nerve blocks, gabapentinoids, and intensive desensitization therapy. If severe stiffness persists despite therapy, a salvage arthroscopic or open capsular release may be considered, though results are often unpredictable.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| SRN Neuritis/Neuroma | 5% - 10% | Iatrogenic traction or transection during proximal exposure. | Observation, gabapentinoids; surgical excision and muscle burying for recalcitrant neuromas. |
| Extensor Tendon Rupture | 2% - 5% | Plate placed superficial to outcroppers; mechanical attrition. | Tendon transfer (e.g., EIP to EPL) or tendon grafting. |
| Malunion / Loss of Reduction | 5% - 8% | Inadequate initial reduction; failure to achieve ligamentotaxis. | Corrective osteotomy with structural bone grafting and revision fixation. |
| Severe Wrist Stiffness / CRPS | 10% - 15% | Prolonged immobilization; exaggerated inflammatory response. | Aggressive hand therapy, sympathetic blocks, late surgical capsulolysis. |
Phased Post-Operative Rehabilitation Protocols
The rehabilitation following dorsal bridge plating is distinctly different from that of standard volar plating, primarily because the radiocarpal joint is intentionally immobilized for an extended period. The protocol is divided into three distinct phases. Phase 1 begins immediately post-operatively and lasts for the first two weeks. The primary goals during this acute phase are aggressive edema control, pain management, and the prevention of digital stiffness. The patient is placed in a bulky soft dressing or a removable volar splint. Immediate, active, full range of motion of all digits (fingers and thumb) is absolutely mandatory. Patients must be instructed to perform tendon gliding exercises to prevent adhesions of
