Biplanar Distal Chevron Osteotomy: A Masterclass in Hallux Valgus Correction

Key Takeaway
This masterclass details the biplanar distal chevron osteotomy for hallux valgus correction. Fellows will learn comprehensive anatomy, meticulous preoperative planning, and granular, real-time intraoperative execution. We cover precise osteotomy techniques, critical neurovascular protection, hardware application, and strategies for managing potential complications. Postoperative rehabilitation protocols are also thoroughly discussed, ensuring a complete understanding from incision to recovery.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues, to the operating theater and to this advanced discourse on forefoot reconstruction. Today, we are undertaking a comprehensive analysis of a ubiquitous yet biomechanically complex deformity: hallux valgus (HV). Specifically, we will dissect the nuances of the biplanar distal chevron osteotomy, a procedure that, when meticulously executed, provides exceptional correction for moderate deformities, particularly those complicated by an increased distal metatarsal articular angle (DMAA). This chapter is designed to transition the orthopedic surgeon from a basic understanding of bunionectomies to a master-level comprehension of triplanar and biplanar corrective principles.
Hallux valgus is not merely a cosmetic bump; it is a progressive, multidimensional derangement of the first ray. It is characterized by the lateral deviation of the hallux proximal phalanx, the reciprocal medial deviation of the first metatarsal (metatarsus primus varus), and the insidious pronation of the great toe. Epidemiologically, it is a pervasive condition, disproportionately affecting females, with a strong familial predisposition suggesting a polygenic inheritance pattern affecting ligamentous laxity and articular geometry. The condition precipitates a cascade of biomechanical failures, typically presenting with debilitating pain over the medial eminence, difficulty accommodating standard footwear, and progressive functional limitations during the propulsive phase of gait.
The pathogenesis of hallux valgus is rooted in a fundamental imbalance of the dynamic and static stabilizers of the first metatarsophalangeal (MTP) joint. The literature increasingly points to the lateral deviation of the great toe as the inciting event, often exacerbated by restrictive, narrow-toe-box footwear. This lateralizing force exerts a varus-producing moment on the first metatarsal head. As the hallux valgus angle (HVA) deteriorates, the intermetatarsal angle (IMA) inevitably widens. Crucially, the sesamoid complex, tethered to the proximal phalanx via the plantar plate and the transverse metatarsal ligament, remains relatively anatomic in its spatial orientation while the first metatarsal head subluxates medially off this fulcrum.
This progressive displacement leads not only to functional deficits but also to profound alterations in forefoot weight-bearing mechanics. The medial column loses its ability to effectively bear weight, leading to load transfer laterally. Patients frequently develop painful transfer metatarsalgia beneath the lesser metatarsal heads, accompanied by intractable plantar keratoses. Understanding this patho-epidemiological cascade is the absolute prerequisite for surgical intervention; we are not merely shaving bone, we are restoring the functional tripod of the foot.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel is ever passed, the surgeon must possess a crystal-clear, three-dimensional understanding of the first ray's surgical anatomy. The first MTP joint is an exquisitely complex articulation, its structural intricacies directly dictating its physiological function and its patterns of pathological failure.
Osteology and Articular Geometry
The osteology of the first ray is uniquely adapted for immense load-bearing and propulsion. The first metatarsal head is broadly convex, featuring a distinct, cartilage-covered sagittal groove on its plantar aspect, which serves as the articulation pathway for the sesamoids. Medially, the metatarsal head presents the medial eminence, a non-articular prominence that becomes hypertrophied and symptomatic in hallux valgus due to chronic bursal inflammation and osteophytic proliferation. Dorsally, repetitive microtrauma can lead to the formation of a "dorsal bunion" or degenerative osteophytes.

The proximal phalanx of the great toe features a shallow, concave articular base designed to glide congruently over the metatarsal head. However, it is the sesamoid complex that represents the mechanical linchpin of the joint. Comprising the tibial (medial) and fibular (lateral) sesamoids embedded within the bifurcated tendons of the flexor hallucis brevis (FHB), this complex acts as a critical fulcrum. It enhances the mechanical advantage of the intrinsic flexors, absorbs weight-bearing forces, and protects the plantar aspect of the metatarsal head. The spatial relationship of the sesamoids relative to the metatarsal head is arguably the most critical diagnostic indicator of deformity severity and rotational malalignment.

Soft Tissue Envelopes and Musculotendinous Dynamics
The ligamentous and capsular structures surrounding the MTP joint undergo profound morphological changes in the presence of hallux valgus. The articular capsule becomes highly asymmetric; the medial capsule and the medial collateral ligament become severely attenuated, redundant, and mechanically incompetent. Conversely, the lateral capsule, the lateral collateral ligament, and the adductor hallucis insertion become rigidly contracted, creating a formidable deforming tether that must be addressed surgically.

The plantar plate is a robust, fibrocartilaginous structure that reinforces the plantar aspect of the joint and houses the sesamoids. A positive MTP joint drawer sign on clinical examination indicates profound instability, typically secondary to attenuation or outright rupture of the plantar capsule or collateral ligaments. The deep transverse metatarsal ligament connects the first metatarsal head to the lesser metatarsals, providing essential stability to the transverse forefoot arch.
Muscularly, the intrinsic and extrinsic tendons act as dynamic deforming forces once alignment is lost. The abductor hallucis, normally a medial stabilizer, loses its mechanical advantage as the metatarsal drifts medially, its vector shifting plantarly to induce hallux pronation. The adductor hallucis becomes an unopposed lateralizing force. Furthermore, the powerful extrinsic tendons—the extensor hallucis longus (EHL) and flexor hallucis longus (FHL)—"bowstring" laterally across the apex of the deformity, exponentially accelerating the valgus drift of the digit.
Neurovascular Topography
Meticulous respect for the neurovascular topography is what separates a competent surgeon from a master. The dorsal medial cutaneous nerve, a terminal branch of the superficial peroneal nerve, courses subcutaneously along the dorsomedial aspect of the first metatarsal. It is exquisitely vulnerable during the initial skin incision and subcutaneous dissection. Iatrogenic injury to this nerve guarantees a highly symptomatic neuroma, often causing more morbidity than the original bunion.

The vascular supply to the first metatarsal head is the most critical anatomical consideration during any distal osteotomy. The primary arterial inflow is derived from the lateral metatarsal artery, a branch of the first dorsal metatarsal artery, which penetrates the lateral capsule and enters the metatarsal head laterally. There is secondary, albeit highly variable, collateral flow from the medial and plantar arterial networks. Excessive periosteal stripping, aggressive lateral capsular release combined with a medial osteotomy, or inadvertent violation of the lateral cortical hinge can obliterate this vascular network. The resulting avascular necrosis (AVN) of the metatarsal head is a catastrophic complication that inevitably leads to joint collapse and requires salvage arthrodesis.
Exhaustive Indications and Contraindications
The biplanar distal chevron osteotomy is a highly versatile tool, but it is not a panacea. Proper patient selection is the cornerstone of surgical success. This procedure is specifically tailored for mild to moderate hallux valgus deformities where the primary pathology involves an abnormal angulation of the distal articular surface—the Distal Metatarsal Articular Angle (DMAA).
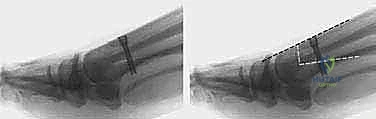
A standard uniplana chevron osteotomy translates the metatarsal head laterally to reduce the IMA, but it does not alter the orientation of the articular cartilage. If a patient presents with an increased DMAA (typically >8-10 degrees), a standard chevron will result in a congruent joint that is still pointing laterally, inevitably leading to clinical recurrence. The biplanar modification involves resecting a medially based wedge of bone from the osteotomy limbs, allowing the surgeon to simultaneously translate the head laterally and tilt the articular surface medially, restoring true joint congruency and alignment.
Contraindications must be strictly observed. Severe deformities (IMA > 15-20 degrees) exceed the translational capacity of a distal osteotomy; attempting a chevron in these cases will result in inadequate correction or perilous lateral overhang of the capital fragment, threatening stability and vascularity. Proximal osteotomies or Lapidus arthrodesis are indicated for severe deformities. Furthermore, hypermobility of the first tarsometatarsal (TMT) joint is a relative contraindication, as a distal procedure will not address the proximal instability, leading to a high rate of recurrence.
| Parameter | Indications for Biplanar Chevron | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Deformity Severity | Mild to Moderate (IMA < 15°, HVA < 30°) | Severe Deformity (IMA > 20°, HVA > 40°) | Moderate-Severe (IMA 15-20°) |
| Articular Geometry | Increased DMAA (> 8-10°) | Severe MTP Joint Osteoarthritis (Hallux Rigidus) | Mild osteophytic changes |
| Joint Status | Congruent or mildly subluxated MTP joint | Active Infection or Charcot Arthropathy | Rheumatoid Arthritis (severe) |
| Proximal Stability | Stable 1st TMT Joint | Profound 1st TMT Hypermobility | Neuromuscular spasticity |
| Patient Factors | Symptomatic despite conservative care | Severe Peripheral Vascular Disease | Uncontrolled Diabetes / Smoking |
Pre-Operative Planning, Templating, and Patient Positioning
Surgical execution is merely the culmination of exhaustive preoperative planning. Our assessment begins with a fastidious history and a dynamic physical examination. We must evaluate the foot with the patient standing, as non-weight-bearing exams drastically underestimate the magnitude of the deformity and the degree of hallux pronation.
Clinical and Radiographic Assessment
The clinical exam must differentiate between flexible and rigid deformities, assess the presence of transfer metatarsalgia, and rigorously test for first ray hypermobility. We perform a drawer test for MTP joint instability and meticulously document the baseline neurovascular status, specifically mapping the sensory distribution of the dorsal medial cutaneous nerve.

Weight-bearing radiographs are non-negotiable. We demand high-quality anteroposterior (AP), lateral, and sesamoid axial views. On the AP view, we measure the HVA (normal <15 degrees) and the IMA (normal <9 degrees). We critically evaluate the sesamoid position relative to the first metatarsal diaphyseal axis, grading it from 0 (normal) to 3 (completely displaced).

The DMAA is the most critical measurement for this specific procedure. It is the angle subtended by a line connecting the medial and lateral articular margins of the metatarsal head and a line perpendicular to the diaphyseal axis. An increased DMAA dictates the need for the biplanar wedge resection. We also assess the relative length of the first and second metatarsals; a chevron osteotomy inherently shortens the first ray slightly, and excessive shortening (>5mm) will virtually guarantee postoperative transfer metatarsalgia.
Templating and Algorithmic Decision Making
Modern digital templating software is invaluable. We template the anticipated osteotomy to calculate the exact millimeter of lateral translation required to normalize the IMA, and we measure the precise angle of the wedge resection needed to normalize the DMAA. This mathematical approach removes intraoperative guesswork.

Patient positioning is critical for optimal ergonomics and exposure. The patient is positioned supine with a bump under the ipsilateral hip to internally rotate the leg, bringing the medial aspect of the foot into a direct vertical alignment facing the surgeon. A well-padded thigh or calf tourniquet is applied. Intravenous antibiotics are administered prior to inflation. The foot is prepped and draped in a standard sterile fashion, ensuring the toes are exposed for intraoperative alignment assessment.
Step-by-Step Surgical Approach and Fixation Technique
The biplanar distal chevron osteotomy demands absolute precision. The margin between a beautifully corrected, stable joint and a catastrophic avascular necrosis or malunion is measured in millimeters.
Incision and Deep Dissection
We begin with a medial longitudinal incision, approximately 5 to 6 centimeters in length, centered over the first MTP joint. The incision is placed slightly dorsal to the midline of the medial eminence to avoid painful plantar scarring. Careful subcutaneous dissection is paramount; we utilize blunt dissection techniques to identify and meticulously retract the dorsal medial cutaneous nerve dorsally, and the plantar medial cutaneous nerve plantarly.

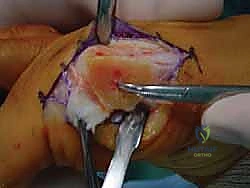
An L-shaped or inverted L-shaped capsulotomy is then performed. The vertical limb is placed just proximal to the base of the proximal phalanx, and the horizontal limb runs along the dorsal or plantar margin of the medial eminence. The capsule is sharply elevated off the medial eminence, creating a robust, full-thickness flap that will be crucial for the final medial capsulorrhaphy. We expose the medial eminence but strictly avoid stripping the capsule laterally or dorsolaterally to preserve the fragile lateral metatarsal artery.

The Biplanar Chevron Osteotomy Execution
The first osseous step is the exostectomy. Using an oscillating saw, the medial eminence is resected in a line parallel to the medial border of the foot, taking care to preserve the sagittal groove plantarly to avoid destabilizing the tibial sesamoid.

We then identify the apex of our osteotomy. A guide pin is placed centrally in the metatarsal head, approximately 1 to 1.5 centimeters proximal to the articular cartilage. This ensures the osteotomy is performed in cancellous bone, optimizing healing potential. The standard chevron is a V-shaped cut with an apex angle of approximately 60 degrees.

To execute the biplanar modification for DMAA correction, we must remove a medially based wedge of bone. This is most commonly performed on the dorsal limb of the osteotomy. The saw blade is directed from medial to lateral, but instead of a single cut, two convergent cuts are made, meeting at the lateral cortex, which acts as a vital hinge. The angle of this wedge corresponds directly to the preoperative templating of the DMAA. The plantar limb is then cut in a standard fashion, ensuring the blade exits proximal to the sesamoid complex to avoid intra-articular damage.

Deformity Correction and Rigid Fixation
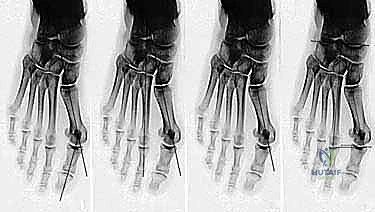
Once the osteotomy is complete, the capital fragment is mobilized. We apply a lateral translating force to the metatarsal head, shifting it laterally by up to 50% of the shaft width to correct the IMA. Simultaneously, the medially based wedge on the dorsal limb is closed, which tilts the articular surface medially, effectively correcting the DMAA and restoring joint congruency.

The capital fragment is then gently impacted onto the metatarsal shaft to ensure bone-to-bone contact and compression. Temporary fixation is achieved with a smooth Kirschner wire driven from dorsal-proximal to plantar-distal. We then evaluate the alignment clinically and fluoroscopically, verifying the HVA, IMA, DMAA, and sesamoid reduction.

Permanent rigid fixation is typically achieved using one or two headless compression screws or specialized osteotomy staples. The hardware must be countersunk to prevent soft tissue irritation. Following fixation, the medial overhanging edge of the proximal metatarsal shaft is resected flush with the translated metatarsal head.

The final, critical step is the medial capsulorrhaphy. The redundant medial capsule is advanced and imbricated to pull the sesamoid complex back under the metatarsal head and to provide a strong medial soft-tissue tether against recurrent valgus drift.

Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, complications can occur. The surgeon must be intimately familiar with the etiology, prevention, and salvage of these adverse events. The biplanar nature of this osteotomy introduces specific risks regarding stability and vascularity that exceed those of a simple uniplana cut.
Avascular necrosis (AVN) of the metatarsal head is the most feared complication. While modern techniques have reduced its incidence to less than 1-2%, it remains catastrophic. AVN is driven by excessive lateral soft tissue stripping combined with violation of the lateral cortical hinge during the osteotomy. Prevention is entirely technique-dependent. Salvage for symptomatic, collapsed AVN is invariably a first MTP joint arthrodesis.

Recurrence of the deformity (incidence 5-10%) is typically the result of under-correction of the DMAA, failure to recognize proximal hypermobility, or inadequate medial capsular plication. Conversely, hallux varus (over-correction) is a highly distressing complication caused by aggressive lateral capsular release, excessive lateral translation of the capital fragment, or over-resection of the medial eminence. Salvage for flexible varus may involve soft tissue reconstruction (e.g., EHB transfer), while rigid varus requires arthrodesis.
Transfer metatarsalgia is a common functional complication resulting from excessive shortening or dorsal elevation of the first metatarsal head during fixation. The first ray loses its weight-bearing capacity, transferring loads to the lesser metatarsals. Prevention requires meticulous attention to the plantar limb cut angle to maintain length and plantarflexion.
| Complication | Estimated Incidence | Primary Prevention Strategy | Salvage/Management Protocol |
|---|---|---|---|
| Avascular Necrosis (AVN) | < 1 - 2% | Preserve lateral capsule/blood supply; avoid excessive stripping. | Non-weight bearing if early; MTP Arthrodesis if collapsed. |
| Recurrence of Deformity | 5 - 10% | Accurate DMAA correction; address hypermobility; robust capsulorrhaphy. | Revision osteotomy (proximal) or Lapidus arthrodesis. |
| Hallux Varus (Overcorrection) | 2 - 5% | Avoid over-resection of medial eminence; conservative lateral release. | Soft tissue release/transfer; MTP Arthrodesis for rigid deformities. |
| Transfer Metatarsalgia | 5 - 15% | Prevent excessive shortening (>5mm) or dorsal elevation of MT head. | Orthotics; Lesser metatarsal Weil osteotomies if severe. |
| Nonunion / Delayed Union | < 1% | Ensure cancellous bone contact; rigid internal compression fixation. | Bone grafting and revision internal fixation. |
| Nerve Injury (Neuroma) | 3 - 5% | Meticulous blunt dissection; identify and retract dorsal medial cutaneous nerve. | Gabapentinoids, targeted injections, surgical excision of neuroma. |
Phased Post-Operative Rehabilitation Protocols
Rehabilitation following a biplanar distal chevron osteotomy is a delicate balance between protecting the osseous integration and preventing debilitating MTP joint stiffness. We employ a strict, phased protocol.

Phase 1 (Weeks 0-2): Tissue Healing and Protection. The patient is placed in a rigid, flat-bottomed postoperative shoe. Weight-bearing is restricted to the heel and lateral border of the foot. The primary goal is wound healing and edema control. Elevation is critical. Dressings remain intact until the first postoperative visit at two weeks, at which point sutures are removed.

Phase 2 (Weeks 2-6): Osseous Consolidation and Early Motion. Radiographs are obtained to verify hardware position and early callus formation. The patient remains in the rigid shoe but can transition to flat-foot weight-bearing as tolerated. Crucially, active and passive range of motion (ROM) exercises of the MTP joint are initiated. The surgeon or physical therapist must instruct the patient to mobilize the joint to prevent capsular adhesions, which are notoriously difficult to resolve later.

Phase 3 (Weeks 6-12): Maturation and Functional Return. At six weeks, assuming radiographic evidence of bridging trabeculae, the patient is transitioned into a wide-toe-box, supportive athletic shoe. Physical therapy intensifies, focusing on intrinsic foot muscle strengthening, gait retraining, and restoration of full MTP joint dorsiflexion required for the propulsive phase of gait. High-impact activities and narrow footwear are strictly prohibited until at least 12 to 16 weeks postoperatively.

Summary of Landmark Literature and Clinical Guidelines
The evolution of the distal chevron osteotomy is a testament to iterative surgical refinement. The original uniplana procedure, popularized by Austin and Leventen in 1981, revolutionized the treatment of mild bunions by providing a stable, intrinsically sound osteotomy that allowed for early weight-bearing. However, long-term follow-up revealed unacceptable recurrence rates in patients with an unaddressed, increased DMAA.

The biplanar modification emerged as a necessary evolution. Landmark biomechanical and clinical studies by authors such as Nery, Sammarco, and Coughlin demonstrated that a congruent joint is the absolute prerequisite for long-term survivorship of the correction. Their work proved that resecting a medially based wedge from the osteotomy limbs effectively reorients the articular cartilage, normalizing the DMAA without compromising the intrinsic stability of the V-cut.

Current clinical guidelines from the American Orthopaedic Foot & Ankle Society (AOFAS) strongly support the use of biplanar distal osteotomies for mild to moderate hallux valgus with an incongruent joint or increased DMAA. The literature confirms that when rigid internal fixation (such as headless compression screws) is utilized, the rates of nonunion and displacement are statistically negligible.

Furthermore, recent systematic reviews have definitively debunked the historical fear of a high AVN rate associated with distal osteotomies, provided that the lateral capsular blood supply is respected and the lateral cortical hinge is not recklessly violated.

As orthopedic surgeons, we must rely on this evidence-based foundation. The biplanar distal chevron osteotomy is not merely a technical exercise; it is a profound biomechanical realignment that demands respect for anatomy, precision in execution, and rigorous adherence to postoperative protocols.





