Butler Procedure for Overlapping Fifth Toe: An Intraoperative Masterclass
Key Takeaway
Join us in the OR for a detailed masterclass on the Butler procedure for overlapping fifth toe. We'll meticulously cover patient positioning, the precise racquet incision, neurovascular preservation, extensor tenotomy, and comprehensive capsular release. Learn critical intraoperative pearls to ensure successful correction and long-term stability, guiding you through every micro-step from initial incision to final closure.
Comprehensive Introduction and Patho-Epidemiology
Clinical Presentation and Demographic Profile
The overlapping fifth toe represents a ubiquitous yet biomechanically complex congenital forefoot deformity that orthopedic surgeons frequently encounter in both pediatric and adult populations. Clinically, the condition is characterized by a pathognomonic triplanar deformity: the fifth toe is rigidly dorsiflexed at the metatarsophalangeal (MTP) joint, adducted toward the midline of the foot, and externally (laterally) rotated such that it overrides the adjacent fourth toe. The deformity is frequently bilateral, presenting in approximately twenty to thirty percent of cases, and demonstrates an equal distribution across male and female demographics. While a definitive genetic locus has not been universally isolated, a strong familial predisposition is routinely observed, suggesting an autosomal dominant pattern of inheritance with variable penetrance.
In the neonate and infant, the overlapping fifth toe is almost universally asymptomatic, prompting consultation primarily due to parental cosmetic concern or anxiety regarding future ambulation. However, as the child transitions into adolescence and adulthood, the natural history dictates a progressive rigidification of the deformity. The dorsally displaced proximal phalanx and the overriding toe create a prominent dorsal profile that is subjected to repetitive microtrauma and shear forces within standard footwear. This mechanical friction inevitably leads to the formation of painful dorsal helomata (corns), adventitial bursitis, and hyperkeratotic lesions over the proximal interphalangeal (PIP) joint or the lateral aspect of the fifth metatarsal head. Consequently, what begins as a benign structural anomaly evolves into a source of significant functional impairment, limiting shoe wear options and causing pronounced ambulatory discomfort.
Nonoperative management modalities, including passive stretching, dynamic splinting, syndactyly taping (buddy taping), and customized orthoses, have historically been employed as first-line therapies. However, the orthopedic literature and extensive clinical experience demonstrate that these conservative measures are almost universally ineffective in achieving permanent structural correction. The soft tissue contractures are too robust, and the deforming forces too chronic, to yield to non-surgical tethering. Therefore, surgical intervention remains the definitive gold standard for symptomatic patients, those with recalcitrant skin ulcerations, or those experiencing severe psychological distress secondary to the cosmetic appearance of the foot.
Pathogenesis and Etiological Theories
The precise embryological etiology of the overlapping fifth toe remains somewhat elusive, though it is widely accepted to be a consequence of a localized soft-tissue dysplasia rather than an intrinsic primary osseous malformation. The prevailing pathogenic theory implicates a congenital, primary contracture of the extensor digitorum longus (EDL) tendon specific to the fifth ray. This shortened, hypertonic musculotendinous unit acts as a relentless deforming force, pulling the proximal phalanx into sustained dorsiflexion and adduction. Over time, this dynamic imbalance induces secondary adaptive changes within the static stabilizers of the MTP joint.
As the proximal phalanx is drawn dorsally, the dorsal and medial aspects of the MTP joint capsule undergo profound fibrotic contracture. This capsular tightening effectively locks the toe in its malaligned position, transforming a dynamic deformity into a rigid structural one. Furthermore, the plantar plate—a critical fibrocartilaginous structure that normally resists MTP joint hyperextension—can become attenuated or adaptively shortened in its proximal-distal dimension, exacerbating the dorsal subluxation of the joint. The collateral ligaments, particularly the medial collateral ligament, also contract, tethering the toe in adduction and preventing passive reduction.
The rotational component of the deformity (lateral or external rotation) is multifactorial. It is partially driven by the eccentric pull of the contracted EDL tendon, but may also be exacerbated by asymmetrical tension from the extensor digitorum brevis (EDB) tendon or imbalances within the intrinsic musculature, such as the plantar interossei and the lumbrical to the fifth toe. Ultimately, the pathogenesis is a cascading sequence of events: a primary tendinous contracture leads to secondary capsuloligamentous fibrosis, culminating in a complex, triplanar subluxation or frank dislocation of the fifth MTP joint that demands meticulous, multi-tiered surgical release.
Detailed Surgical Anatomy and Biomechanics
Osteology and Metatarsophalangeal Joint Mechanics
A profound mastery of the osteology and articular mechanics of the fifth ray is non-negotiable for the operating surgeon. The fifth metatarsal head serves as the convex proximal articular surface of the MTP joint. In the setting of an overlapping fifth toe, the metatarsal head itself is typically morphologically normal, lacking the structural abnormalities seen in conditions like a tailor's bunion (though the two can occasionally coexist). However, the base of the proximal phalanx, which forms the concave distal articular surface, is chronically displaced dorsally and medially.
This sustained dorsal subluxation alters the normal instantaneous center of rotation of the MTP joint. The articular cartilage of the dorsal metatarsal head may exhibit localized wear or fibrillation due to the abnormal contact pressures exerted by the overriding proximal phalanx. During the Butler procedure, the surgeon must recognize that the osseous structures themselves do not require osteotomy or resection; rather, the goal is to liberate the constrained proximal phalanx and restore its congruent articulation with the metatarsal head. The MTP joint capsule, a robust fibrous sleeve, is the primary static restraint that must be systematically dismantled. The dorsal and medial capsular tissues are typically thickened and fibrotic, requiring sharp surgical release to permit plantarward and lateral translation of the toe.
Tendinous Architecture and Deforming Forces
The tendinous anatomy of the fifth toe dictates the surgical approach to soft-tissue balancing. The extensor digitorum longus (EDL) tendon is the primary antagonist in this pathology. Originating from the anterior compartment of the leg, it traverses the ankle and foot to insert onto the dorsal base of the middle and distal phalanges of the fifth toe. Its congenital shortening is the primary driver of the dorsiflexion and adduction deformity. During the Butler procedure, a complete transverse tenotomy of the EDL is an absolute prerequisite for correction.
The extensor digitorum brevis (EDB) tendon to the fifth toe, when present (it is occasionally absent in normal anatomy), joins the EDL tendon and can contribute to the lateral rotational vector of the deformity. Deep to the extensors lie the flexor tendons: the flexor digitorum longus (FDL) and flexor digitorum brevis (FDB). These structures run plantar to the MTP joint and are generally not the primary contracted tissues in this specific deformity. However, their relative length and tension become critically important once the extensor forces are negated. If the flexors are overly tight, they may induce a secondary hammer toe deformity post-correction. Therefore, intraoperative assessment of flexor tension is necessary, though routine flexor tenotomy is rarely indicated in a classic Butler procedure unless a concomitant sagittal plane deformity of the interphalangeal joints exists.
Neurovascular Topography of the Fifth Ray
The neurovascular anatomy of the fifth digit represents the "danger zone" of the Butler procedure. Iatrogenic injury to these structures is the most devastating complication, potentially leading to digital ischemia, necrosis, or chronic neuropathic pain. The blood supply to the fifth toe is derived from the dorsal and plantar digital arteries. The dorsal digital arteries, branches of the dorsal metatarsal arteries, supply the dorsal skin and superficial structures. They are relatively small and delicate, running superficially within the subcutaneous tissue.
The plantar digital arteries, branches of the plantar metatarsal arteries, are significantly more robust and provide the dominant arterial supply to the digit. They course along the medial and lateral plantar aspects of the toe, intimately associated with the plantar digital nerves. The plantar digital nerves, terminal branches of the superficial fibular and lateral plantar nerves, provide profound sensory innervation to the toe. During the execution of the double-racquet incision and subsequent skin flap elevation, the surgeon must maintain a precise dissection plane. The neurovascular bundles lie perilously close to the flexor tendon sheath and the MTP joint capsule. Aggressive retraction, careless use of electrocautery, or dissecting too superficially can easily compromise these bundles, making meticulous, blunt dissection and absolute hemostasis paramount.
Exhaustive Indications and Contraindications
Patient Selection Criteria
The decision to proceed with a Butler procedure must be grounded in stringent patient selection criteria. The ideal candidate is a pediatric patient (typically between the ages of 1 and 12 years) or an adolescent presenting with a rigid, symptomatic overlapping fifth toe. Symptoms warranting intervention include persistent pain exacerbated by footwear, recurrent dorsal ulcerations or intractable keratoses, and significant difficulty in obtaining proper shoe fit. Furthermore, severe cosmetic deformity causing psychological distress in the adolescent patient is a valid indication, provided the patient and family have realistic expectations regarding scarring and postoperative toe morphology.
The Butler procedure is uniquely designed to address the specific pathoanatomy of the overlapping fifth toe—namely, the dorsal skin contracture, the EDL shortening, and the dorsomedial capsular fibrosis. It relies on the ingenious double-racquet incision to physically transpose the toe into a plantar and lateral position while simultaneously excising redundant dorsal skin and providing a V-Y advancement effect plantarly. Therefore, it is the procedure of choice when the deformity is primarily driven by soft-tissue contracture at the MTP joint without significant underlying osseous angular deformity (such as a severe metatarsus adductus or a structural clinodactyly of the phalanges).
Contraindications to the Butler Procedure
Contraindications to the Butler procedure can be categorized into absolute and relative parameters. Absolute contraindications include the presence of active local or systemic infection, severe peripheral vascular disease (which would preclude adequate healing of the complex skin flaps), and profound peripheral neuropathy (where the patient lacks protective sensation and cannot participate in postoperative rehabilitation). Furthermore, if the deformity is entirely passively correctable without tension, surgical intervention is generally unwarranted, and continued conservative management or observation is advised.
Relative contraindications include severe, rigid osseous deformities of the metatarsal or phalanges that cannot be corrected by soft-tissue release alone. In such cases, osseous procedures (e.g., metatarsal osteotomies or phalangeal wedge resections) may be required in conjunction with, or instead of, the Butler procedure. Additionally, prior failed surgical interventions on the fifth toe that have resulted in severe cicatricial scarring or compromised vascularity to the dorsal or plantar skin flaps make the Butler procedure technically hazardous. In these revision scenarios, alternative approaches, such as amputation or syndactyly, must be heavily considered.
| Category | Indications for Butler Procedure | Contraindications for Butler Procedure |
|---|---|---|
| Clinical Presentation | Painful dorsal callosities/ulcerations; difficulty with shoe wear; severe cosmetic distress. | Asymptomatic, passively correctable deformity; mild cosmetic concern. |
| Pathoanatomy | Rigid dorsiflexion, adduction, and external rotation driven by soft-tissue contracture at the MTP joint. | Primary osseous angular deformity (e.g., severe clinodactyly requiring osteotomy). |
| Patient Factors | Pediatric or adolescent age group (ideal); compliant adults with good vascular status. | Severe peripheral vascular disease; active infection; profound neuropathy. |
| Surgical History | Primary surgical intervention for the deformity. | Extensive prior surgery with severe scarring and compromised local vascularity. |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-Operative Clinical Assessment
A rigorous preoperative clinical examination is the foundation of a successful surgical outcome. The surgeon must meticulously document the resting posture of the fifth toe, quantifying the degrees of dorsiflexion, adduction, and external rotation. Crucially, the examiner must assess the passive correctability of the deformity. In a true overlapping fifth toe suitable for a Butler procedure, the deformity is rigid; attempting to plantarflex and abduct the toe will elicit palpable tension in the EDL tendon and the dorsal skin. The presence, location, and severity of hyperkeratotic lesions or bursitis must be noted, as these areas will dictate the precise placement of the dorsal racquet incision to ensure excision of the diseased skin.
A comprehensive neurovascular examination is absolutely critical. The surgeon must document palpable pedal pulses (dorsalis pedis and posterior tibial arteries) and assess capillary refill in all digits, particularly the fifth toe. Sensory examination using Semmes-Weinstein monofilaments should be performed to rule out underlying neuropathy. Any evidence of vascular compromise or sensory deficit must prompt further investigation (e.g., non-invasive arterial studies) and may necessitate a re-evaluation of the surgical plan. The surgeon must also evaluate the overall foot biomechanics, noting the presence of pes planus, pes cavus, or a hypermobile first ray, as these global biomechanical factors can influence the long-term success of the localized toe correction.
Radiographic Evaluation and Templating
While the diagnosis of an overlapping fifth toe is fundamentally clinical, standard weight-bearing radiographs of the foot are an indispensable component of preoperative planning. A complete series, including anteroposterior (AP), lateral, and oblique views, should be obtained. The AP view will clearly demonstrate the medial deviation (adduction) of the proximal phalanx relative to the fifth metatarsal and the overlapping of the fourth toe. The lateral and oblique views are critical for visualizing the dorsal subluxation or dislocation of the MTP joint.
Radiographic templating involves assessing the congruency of the MTP joint and ruling out concomitant osseous pathologies. The surgeon must evaluate the fifth metatarsal for excessive lateral bowing or a prominent lateral condyle (tailor's bunion), which might necessitate a concurrent distal metatarsal osteotomy. Furthermore, the phalanges should be inspected for structural clinodactyly or symphalangism. If the deformity is purely soft-tissue driven, the bones will appear morphologically normal but spatially misaligned. The radiographs serve as a baseline to ensure that postoperatively, the MTP joint has been anatomically reduced.
Patient Positioning and Operative Setup
Impeccable patient positioning and operating room setup are vital for ensuring optimal surgical exposure and minimizing intraoperative fatigue. The patient is placed in the supine position on a standard operating table. To facilitate access to the lateral aspect of the foot, a well-padded bump or bolster is placed beneath the ipsilateral hemipelvis. This maneuver subtly internally rotates the lower extremity, bringing the fifth toe into a direct, vertical line of sight for the surgeon and preventing the need for awkward, non-ergonomic leaning over the patient.
A sterile pneumatic tourniquet is universally employed to guarantee a completely bloodless surgical field. For isolated forefoot procedures like the Butler, an ankle or calf tourniquet is typically sufficient and minimizes the total volume of ischemic tissue. The tourniquet is inflated to approximately 100 mmHg above the patient's systolic blood pressure after exsanguination of the limb with an Esmarch bandage. The entire foot, ankle, and distal leg are meticulously prepped with a standard surgical antiseptic (e.g., chlorhexidine gluconate or povidone-iodine) and draped in a standard sterile fashion. While the procedure relies heavily on direct visualization and soft-tissue balancing, having a mini C-arm fluoroscopy unit available in the room is highly recommended to confirm the concentric reduction of the MTP joint prior to final skin closure.
Step-by-Step Surgical Approach and Fixation Technique
The Double-Racquet Incision Design
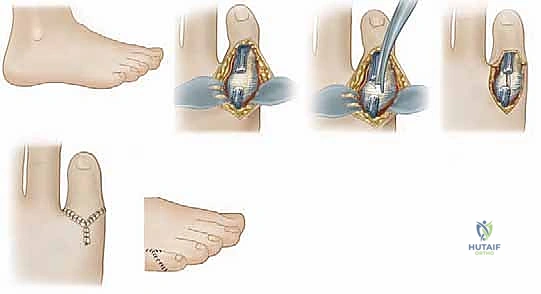
The architectural brilliance of the Butler procedure lies in its unique double-racquet incision. This specific geometry is not merely an approach to the deep structures; it is a dynamic, integral component of the correction itself. The incision is designed to simultaneously excise contracted, redundant dorsal skin while creating a plantar defect that accommodates the toe as it is transposed into its new, corrected position. The design requires meticulous pre-incision marking with a surgical pen.
The surgeon begins by drawing the "dorsal racquet." A curvilinear incision is marked starting just proximal to the MTP joint on the dorsum of the foot. It sweeps distally, curving around the medial aspect of the base of the fifth toe, continues across the dorsal web space, and then curves back proximally along the lateral aspect of the toe to meet the starting point. This creates a racquet head that encompasses the dorsal callosity and the contracted skin. From the proximal apex of this dorsal racquet, the "plantar handle" is marked. This is a longitudinal incision extending distally along the plantar aspect of the foot, aiming slightly laterally toward the base of the fifth toe. Crucially, the plantar handle must be longer than the dorsal defect to allow the toe to "drop" into the plantar space without creating tension on the proximal apex during closure.
Skin Flap Elevation and Neurovascular Protection
Once the incision is made using a #15 scalpel blade, the critical phase of skin flap elevation commences. The surgeon must elevate full-thickness dermocutaneous flaps, maintaining a robust layer of subcutaneous fat attached to the skin to preserve the subdermal vascular plexus. Dissection is performed with meticulous care, utilizing fine dissecting scissors or a blunt-tipped instrument to separate the subcutaneous tissue from the underlying extensor tendon and MTP joint capsule.
During this elevation, the surgeon must be hyper-vigilant regarding the neurovascular bundles. The dorsal digital nerves and vessels are encountered first and must be gently retracted medially and laterally with the skin flaps. As the dissection proceeds plantarly to develop the handle of the racquet, the larger plantar digital neurovascular bundles come into proximity. These structures lie just deep to the subcutaneous fat, adjacent to the flexor tendon sheath. The surgeon must avoid deep, blind dissection in the plantar aspect of the wound. Meticulous hemostasis using bipolar electrocautery (avoiding monopolar cautery near the nerves) is essential to maintain visibility and prevent postoperative hematoma, which could compromise flap viability.
Extensor Tenotomy and Dorsomedial Capsular Release
With the deep structures adequately exposed, the surgeon targets the primary deforming forces. The extensor digitorum longus (EDL) tendon is readily identified as a taut, fibrotic band crossing the dorsal aspect of the MTP joint. Using a curved mosquito hemostat, the surgeon carefully isolates the EDL tendon, passing the instrument deep to the tendon but superficial to the joint capsule to protect the underlying articular cartilage. A complete transverse tenotomy is then performed using a #15 blade or tenotomy scissors. A palpable release of tension is immediately appreciated as the tendon ends retract.
Following the tenotomy, the surgeon addresses the contracted MTP joint capsule. A dorsal capsulotomy is performed by making a transverse incision through the capsule just proximal to the base of the proximal phalanx. This incision is then extended medially to release the medial collateral ligament and the medial capsule. This dorsomedial release is the crux of the deep dissection; it liberates the proximal phalanx from its tethered, adducted, and dorsiflexed position. The surgeon must ensure the release is complete, extending plantarly enough on the medial side to allow the toe to derotate and translate laterally. Care must be taken not to score the articular cartilage of the metatarsal head during these capsular cuts.
Intraoperative Assessment and Soft Tissue Balancing
After the sequential release of the EDL tendon and the dorsomedial capsule, the surgeon must critically assess the degree of correction. The fifth toe is gently manipulated. It should now easily and passively drop into a plantarflexed, abducted (laterally translated), and derotated position. The toe should comfortably rest within the defect created by the plantar handle of the racquet incision. There should be absolutely no elastic resistance or tendency for the toe to spring back into its preoperative overriding position.
If residual tension exists, the surgeon must systematically re-evaluate the releases. Is the lateral slip of the EDB tendon tethering the toe? If so, it must be sectioned. Is the plantar plate or the plantar capsule preventing full plantarflexion? In severe, chronic cases, a careful, limited release of the plantar capsule off the metatarsal neck may be required, though this must be done judiciously to avoid creating MTP joint instability. The goal is a completely flaccid, tension-free reduction of the MTP joint. The surgeon may utilize the mini C-arm at this juncture to confirm that the proximal phalanx is concentrically reduced on the metatarsal head in both the AP and lateral planes.
Skin Closure and Stabilization
The final, and arguably most technically demanding, step of the Butler procedure is the skin closure. The closure itself acts as the primary stabilizing force for the newly positioned toe. The surgeon first addresses the dorsal defect. The redundant island of skin encompassed by the dorsal racquet head is sharply excised. The toe is then physically manipulated down into the plantar handle of the incision.
The skin closure begins at the proximal apex of the dorsal incision. Using fine, absorbable monofilament or braided sutures (e.g., 4-0 or 5-0 Monocryl, Vicryl, or Chromic gut), the surgeon approximates the medial and lateral skin flaps over the dorsum of the joint. As the closure proceeds distally, the tension of the sutured skin effectively pushes the toe plantarly and laterally. The plantar aspect of the incision is then closed. Because the toe has been transposed proximally and plantarly, the plantar handle closes in a V-Y advancement fashion, further securing the toe in its corrected alignment. The surgeon must ensure that the skin edges are perfectly everted and that there is no undue tension on the flaps, which could lead to marginal necrosis. Deep dermal sutures are generally avoided to minimize foreign body reaction and the risk of strangulating the delicate dermal microcirculation.
Complications, Incidence Rates, and Salvage Management
Neurovascular Compromise and Flap Necrosis
The most feared and potentially catastrophic complication of the Butler procedure is iatrogenic neurovascular compromise. Given the complex geometry of the double-racquet incision and the extensive soft-tissue undermining required, the vascular supply to the skin flaps—particularly the distal tip of the dorsal flap—is tenuous. Vascular compromise can manifest as arterial insufficiency (pale, cool flaps with absent capillary refill) or venous congestion (violaceous, engorged flaps with rapid, dark capillary refill). The incidence of partial flap necrosis is reported to be between 2% and 5%, while complete digital ischemia is exceedingly rare but devastating.
Prevention is paramount: the surgeon must handle tissues with atraumatic technique, maintain thick subcutaneous flaps, avoid excessive tourniquet times, and ensure the skin closure is entirely tension-free. If arterial insufficiency is noted intraoperatively upon tourniquet deflation, the surgeon must immediately remove sutures to relieve tension, apply warm saline compresses, and consider the application of topical vasodilators (e.g., papaverine). If venous congestion occurs, loosening sutures and elevating the limb are first-line steps. Postoperatively, superficial flap epidermolysis usually heals secondarily with meticulous local wound care. However, full-thickness necrosis may require subsequent debridement, healing by secondary intention, or, in severe cases, skin grafting or delayed amputation.
Recurrence and Under-Correction
Recurrence of the overlapping deformity or persistent under-correction is the most common mechanical complication, with literature reporting incidence rates ranging from 5% to 15%. Recurrence is almost exclusively the result of an inadequate initial surgical release. Failure to completely transect the EDL tendon, incomplete release of the dorsomedial capsule, or failure to recognize and release a contracted plantar plate will inevitably lead to the toe migrating back to its preoperative position as the tissues heal and scar contracture occurs.
Furthermore, if the plantar handle of the racquet incision is cut too short, the toe will not be able to transpose sufficiently plantarly, leading to immediate under-correction. Salvage management for a recurrent overlapping fifth toe is technically challenging due to the presence of dense cicatricial scar tissue from the index procedure. Revision surgery requires a meticulous re-exploration, often necessitating more extensive capsular releases, potential flexor tenotomies, or even osseous procedures such as a proximal phalangeal hemiphalangectomy (Ruiz-Mora procedure) or a syndactyly to the fourth toe to mechanically tether the digit in a corrected position.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Partial Flap Necrosis | 2% - 5% | Tension on closure; thin flaps; aggressive cautery; venous congestion. | Suture removal; local wound care; topical vasodilators; rarely skin grafting. |
| Recurrence / Under-correction | 5% - 15% | Incomplete EDL tenotomy; inadequate capsular release; short plantar incision. | Revision capsulotomy; Ruiz-Mora procedure; syndactyly to 4th toe. |
| Digital Ischemia / Loss | < 1% | Direct arterial transection; severe tension; prolonged tourniquet time. | Immediate tension release; vascular surgery consultation; amputation if non-viable. |
| Infection (Superficial) | 1% - 3% | Poor patient hygiene; early exposure to moisture; compromised flap viability. | Oral antibiotics; local wound care; close clinical monitoring. |
| Floating Toe Deformity | 2% - 4% | Over-release of plantar structures; excessive EDL resection without flexor balancing. | Flexor tendon transfer (Girdlestone-Taylor); plantar capsulorrhaphy. |
Phased Post-Operative Rehabilitation Protocols
Immediate Post-Operative Phase (Weeks 0-2)
The immediate postoperative period is focused on protecting the delicate soft-tissue reconstruction, minimizing edema, and ensuring flap viability. Upon completion of the procedure, a bulky, non-adherent compressive dressing is applied in the operating room. The fifth toe is meticulously splinted in its new, corrected (plantarflexed and abducted) position using sterile gauze woven between the toes and secured with cohesive bandage. The patient is typically discharged on the same day with strict instructions for continuous limb elevation above the level of the heart for the first 48 to 72 hours to combat venous congestion and swelling.
Weight-bearing status is generally restricted to heel-weight-bearing only in a rigid, postoperative shoe or a controlled ankle motion (CAM) boot. Direct forefoot loading is strictly prohibited to prevent tension on the plantar incision and to avoid displacing the MTP joint before early capsular healing can occur. The patient is instructed to keep the dressing entirely clean, dry, and intact. The first postoperative clinical evaluation occurs at approximately 10 to 14 days. During this visit, the bulky dressing is carefully removed, and the skin flaps are meticulously inspected for signs of marginal necrosis, dehiscence, or infection. If non-absorbable sutures were utilized, they are typically removed at this time, provided the incision lines are stable.
Intermediate Phase (Weeks 2-6)
Assuming uncomplicated wound healing, the intermediate phase transitions toward maintaining the correction while allowing for gradual mobilization. Following suture removal or confirmation of absorbable suture dissolution, the patient is transitioned to a specialized toe-taping protocol. The fifth toe is "buddy taped" to the adjacent fourth toe, ensuring it is held in a neutral or slightly plantarflexed alignment. This taping acts as a dynamic splint, countering any residual tendinous pull and guiding the maturing scar tissue to heal in the elongated position.
Weight-bearing is progressively advanced to full weight-bearing as tolerated, though the patient must continue to utilize a stiff-soled postoperative shoe or a wide-toebox athletic shoe to prevent lateral compression of the fifth digit. The patient and family are instructed on gentle, passive plantarflexion stretching exercises of the MTP joint to prevent recurrent dorsal capsular contracture. Activities are restricted; high-impact loading, running, and jumping are strictly prohibited during this phase to allow the deep capsular tissues to achieve adequate tensile strength.
Long-Term Follow-Up and Return to Activity
The long-term rehabilitation phase, extending from 6 weeks to 3 months postoperatively, focuses on returning the patient to full, unrestricted activity and normal footwear. By the 6-week mark, the buddy taping can typically be discontinued, though some surgeons advocate for continued nighttime taping for up to 3 months in severe cases. The patient is encouraged to transition into standard, comfortable footwear, emphasizing shoes with a wide and deep toe box to accommodate the foot without exerting medial pressure on the fifth toe.
Clinical follow-up is recommended at 3 months and 6 months to assess the durability of the correction and monitor for any signs of recurrence. The surgeon must evaluate the toe for a "floating" posture (inability to purchase the ground during stance phase), which can occasionally occur if the plantar structures were over-released. By 3 months, the vast majority of patients can resume all high-impact sports and recreational activities without restriction. The final cosmetic appearance of the toe, including the maturation of the dorsal and plantar scars, should be discussed with the patient, noting that maximal scar fading can take up to a full year.
Summary of Landmark Literature and Clinical Guidelines
Historical Context and Evolution of the Procedure
The surgical management of the overlapping fifth toe has evolved significantly over the past century. Early interventions often relied on aggressive osseous resections, such as the Ruiz-Mora procedure (excision of the proximal phalanx), which, while effective at eliminating the dorsal prominence, frequently resulted in a functionally compromised, shortened,
