Midfoot Arthrodesis: An Intraoperative Masterclass for Complex Deformity

Key Takeaway
This masterclass guides fellows through midfoot arthrodesis, a definitive treatment for arthrosis and deformity. We cover essential anatomy, meticulous preoperative planning, and step-by-step intraoperative execution, including dual dorsal approaches and precise hardware application. Critical pearls on neurovascular protection, deformity reduction, and preventing malunion are emphasized, alongside comprehensive postoperative care protocols to ensure optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater and to this definitive masterclass on midfoot arthrodesis. Today, we are addressing a highly challenging case of complex midfoot deformity requiring meticulous arthrodesis. This procedure remains a foundational cornerstone in advanced reconstructive foot and ankle surgery. It is precisely designed to definitively treat midfoot arthrosis, whether isolated or presenting with severe, multi-planar deformity. Our ultimate surgical objective is unambiguous: to restore a rigid, plantigrade foot that is fundamentally capable of effective, pain-free push-off during the terminal stance phase of the gait cycle. Achieving this requires not just mechanical carpentry, but a profound understanding of foot biomechanics.
With progressive midfoot deformity, we consistently observe a predictable, devastating cascade of biomechanical failures. The hindfoot, initially attempting to compensate for midfoot instability, eventually loses its physiologic alignment. It typically drifts into a greater-than-physiologic valgus posture, shifting the mechanical axis laterally. This altered alignment invariably leads to secondary shortening of the gastroc-soleus complex and the Achilles tendon, manifesting clinically as a rigid equinus contracture. In extreme, long-standing cases—particularly those involving neuroarthropathy—this pathological cascade can lead to incongruence within the ankle joint itself, placing abnormal, asymmetric stresses proximally and leading to pantalar degeneration.
The midfoot's architecture is an elegant but unforgiving complex of osseous structures, forming critical arches in both the longitudinal and transverse planes. Any traumatic injury or insidious degenerative process here, particularly involving the crucial "Lisfranc ligament" complex spanning the base of the second metatarsal and the medial cuneiform, catastrophically destabilizes this architecture. This destabilization initiates a gradual, progressive arch collapse, almost universally accompanied by forefoot abduction. The intermediate (second) cuneiform acts as the vital keystone to the transverse arch; its structural or ligamentous compromise has profound, global effects on foot biomechanics, effectively destroying the foot's ability to act as a rigid lever.

When this normally compact and highly stable midfoot anatomy is compromised, the crucial talo–first metatarsal relationship (Meary's line) is disrupted. This loss of colinearity directly translates to a massive loss of mechanical advantage during the stance and push-off phases of gait, leading to debilitating pain and functional impairment. In the sagittal plane, this presents as a loss of the longitudinal arch, clinically recognized as a "midfoot sag." With advanced disease progression, this can culminate in a severe "rocker-bottom deformity," where the arch entirely reverses, and the midfoot pathologically becomes the primary weight-bearing surface. Concurrently, in the coronal plane, the forefoot drifts into severe abduction relative to the hindfoot. A normal plantigrade foot distributes weight evenly across a tripod consisting of the first metatarsal head, the fifth metatarsal head, and the calcaneal tuberosity; midfoot collapse obliterates this balance, shifting immense load directly onto the collapsing, painful midfoot articulations.
Detailed Surgical Anatomy and Biomechanics
Let us systematically review the critical surgical anatomy of the midfoot, as a precise, three-dimensional understanding is absolutely paramount for successful arthrodesis and avoidance of catastrophic iatrogenic complications.
Osteology and Columnar Biomechanics
The midfoot is composed of five tarsal bones (the navicular, the cuboid, and the medial, intermediate, and lateral cuneiforms) articulating with the bases of the five metatarsals. The key articulations targeted for arthrodesis typically include the Tarsometatarsal (TMT) joints. The first TMT joint lies between the medial cuneiform and the first metatarsal. The second TMT joint, recessed proximally between the medial and lateral cuneiforms, forms the absolute keystone of the transverse arch; its stability is non-negotiable. The third TMT joint connects the lateral cuneiform and the third metatarsal, while the fourth and fifth TMT joints articulate with the cuboid. Arthrodesis may also need to encompass the naviculocuneiform joints and the intercuneiform articulations depending on the extent of the arthritic or deformative process.
In the coronal and sagittal planes, the midfoot must be conceptualized as three distinct functional columns. The medial column comprises the first ray (medial cuneiform and first metatarsal). The middle column comprises the second and third rays (intermediate cuneiform, lateral cuneiform, second and third metatarsals). The lateral column comprises the fourth and fifth rays (cuboid, fourth and fifth metatarsals). Physiologically, the medial and middle columns are characterized by highly congruent joints and incredibly tight ligamentous restraints, allowing minimal physiologic motion. This inherent stiffness is biomechanically crucial, enabling the medial aspect of the foot to function as a rigid lever for propulsion.
Conversely, the lateral column (fourth and fifth rays) is relatively supple and mobile. This mobility allows the foot to accommodate to uneven terrain and absorb shock during heel strike and early stance. This stark physiological distinction dictates our surgical philosophy: arthrodesis of the medial and middle columns in anatomic alignment creates very few functional deficits and is highly successful. However, arthrodesis of the lateral column is generally contraindicated unless absolutely necessary (e.g., severe gross instability or recalcitrant pain), as it sacrifices the foot's vital accommodative capacity, drastically increasing stresses on adjacent joints and frequently leading to lateral column overload and nonunion.
Ligamentous and Neurovascular Restraints
The ligamentous anatomy of the midfoot is robust, with the plantar ligaments being significantly thicker and stronger than their dorsal counterparts. The Lisfranc ligament is paramount; it is a massive, short oblique ligament originating from the lateral-plantar aspect of the medial cuneiform and inserting onto the medial-plantar aspect of the base of the second metatarsal. This ligament, functioning in concert with the dorsal and interosseous TMT ligaments, provides critical stability to the second TMT joint and prevents lateral subluxation of the lesser metatarsals. Disruption of this ligamentous complex is the defining hallmark of a Lisfranc injury and the primary catalyst for post-traumatic midfoot collapse.

When executing dorsal surgical approaches, the operating surgeon must be acutely aware of the superficial and deep neurovascular bundles. The Superficial Peroneal Nerve (SPN) emerges from the deep fascia in the distal third of the leg, dividing into medial and intermediate dorsal cutaneous nerves. These branches traverse the dorsal aspect of the midfoot and are highly variable in their arborization. They are extremely vulnerable during dorsal skin incisions, particularly the lateral-based incisions, and iatrogenic injury can lead to debilitating neuromas. Meticulous blunt dissection in the subcutaneous tissues is mandatory.
The Deep Peroneal Nerve (DPN) and the Dorsalis Pedis Artery form the deep neurovascular bundle. This bundle runs immediately deep to the extensor hallucis longus (EHL) tendon and medial to the extensor hallucis brevis (EHB) muscle belly. The DPN provides essential motor innervation to the extensor digitorum brevis and critical sensation to the first web space. The dorsalis pedis artery is the primary arterial supply to the dorsal foot. These structures are at extreme risk during deep dissection, particularly during the medial dorsal approach to the first and second TMT joints. The EHB muscle-tendon unit serves as a reliable surgical landmark; retracting the EHB laterally generally protects the deep neurovascular bundle beneath it.
Exhaustive Indications and Contraindications
The decision to proceed with a midfoot arthrodesis must be predicated on a rigorous evaluation of the patient's pathology, functional demands, and medical comorbidities. Patient selection is arguably as critical as the surgical execution itself.
Primary Indications for Arthrodesis
The most frequent indication for midfoot arthrodesis is post-traumatic osteoarthritis, classically following a missed, mismanaged, or severely comminuted Lisfranc fracture-dislocation. These patients typically present months to years after the initial injury with progressive midfoot collapse, intractable pain with weight-bearing, and inability to wear standard footwear due to dorsal osteophyte formation and forefoot abduction. Arthrodesis in this setting aims to re-establish the structural integrity of the medial and middle columns, resect the painful arthritic surfaces, and restore the longitudinal arch.
Primary osteoarthritis, while less common than post-traumatic etiologies, frequently affects the first and second TMT joints, particularly in older females. Inflammatory arthropathies, such as Rheumatoid Arthritis, can lead to global midfoot destruction, requiring extensive pan-tarsal fusions. Furthermore, Charcot neuroarthropathy represents a unique and incredibly challenging indication. In the diabetic Charcot foot, midfoot arthrodesis (often termed midfoot reconstruction or super-construct fixation) is indicated for severe deformity, instability, or impending/active ulceration that cannot be managed with total contact casting or custom orthotics. The goal here is salvage of a plantigrade, braceable foot to prevent major amputation.

Absolute and Relative Contraindications
Absolute contraindications to midfoot arthrodesis include active, untreated deep soft tissue or bone infection (osteomyelitis). In cases of active infection, the primary goal must be eradication through debridement and targeted antibiotic therapy before any definitive reconstructive arthrodesis can be entertained. Severe peripheral arterial disease (PAD) is another absolute contraindication; a foot with inadequate perfusion will not heal a complex fusion and is at massive risk for catastrophic wound necrosis and subsequent amputation. Non-invasive vascular studies (ABIs, toe pressures) are mandatory in any patient with absent pulses or a history of vascular disease.
Relative contraindications require careful preoperative optimization and patient counseling. Uncontrolled diabetes mellitus (HbA1c > 8.0%) significantly increases the risk of nonunion and surgical site infection. Active tobacco use is a profound risk factor for nonunion; many surgeons, myself included, require laboratory-confirmed smoking cessation (negative cotinine levels) for at least 4-6 weeks prior to elective midfoot arthrodesis. Severe osteoporosis can compromise hardware purchase, necessitating the use of specialized locking plates, prolonged non-weight-bearing periods, or adjunctive biologic stimulation.
| Category | Specific Conditions | Clinical Management / Considerations |
|---|---|---|
| Absolute Indications | End-stage post-traumatic arthrosis; Painful primary OA of TMT joints; Unstable Charcot neuroarthropathy with impending ulceration. | Requires rigid internal fixation and anatomic realignment. |
| Relative Indications | Flexible flatfoot with symptomatic midfoot sag; Rheumatoid arthritis with midfoot involvement. | May attempt conservative care (orthotics, bracing) prior to surgical intervention. |
| Absolute Contraindications | Active deep infection/osteomyelitis; Severe peripheral arterial disease (ABI < 0.5 or flat toe pressures). | Infection eradication and vascular bypass/angioplasty must precede orthopedic reconstruction. |
| Relative Contraindications | Active smoking; Uncontrolled Diabetes (HbA1c > 8%); Severe osteopenia/osteoporosis. | Mandate smoking cessation; Optimize glycemic control; Plan for augmented fixation (locking plates, orthobiologics). |
Pre-Operative Planning, Templating, and Patient Positioning
Preoperative planning is the absolute bedrock of a successful outcome in complex midfoot reconstruction. Failure to plan is planning to fail, particularly when addressing multi-planar deformities.
Clinical Evaluation and Imaging
The physical examination must be performed with the patient weight-bearing, if tolerated. We assess the overall alignment, comparing it to the contralateral limb to establish the patient's baseline physiologic alignment. We look for the classic signs of advanced disease: loss of the medial longitudinal arch, forefoot abduction, and the presence of a medial bony prominence (uncovered navicular or medial cuneiform). The "piano key test" is utilized to isolate pathology to specific TMT joints by individually stressing each metatarsal dorsally and plantarly. A rigorous neurologic examination using Semmes-Weinstein monofilaments is mandatory to rule out unrecognized neuropathy. Furthermore, the Silfverskiöld test is critical to evaluate for isolated gastrocnemius tightness versus a combined gastroc-soleus equinus contracture, which dictates the type of posterior lengthening required.
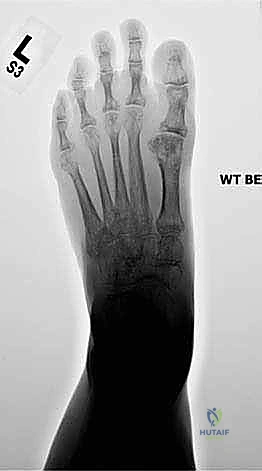
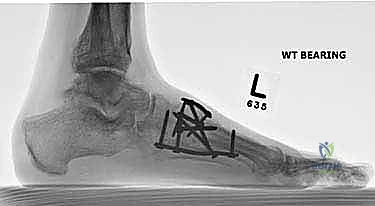
Radiographic evaluation begins with high-quality, weight-bearing AP, lateral, and oblique views of the foot. On the AP view, we assess the alignment of the medial border of the second metatarsal with the medial border of the intermediate cuneiform, and the congruity of the talo-first metatarsal axis. The oblique view is crucial for evaluating the lateral column (cuboid and 4th/5th TMTs). The lateral view is essential for assessing the sagittal profile, specifically looking for midfoot sag at the TMT or naviculocuneiform joints. Meary's line should be colinear; any plantar or dorsal angulation indicates structural collapse.
While standard radiographs are sufficient for straightforward cases, advanced imaging is often required for complex post-traumatic deformities. A fine-cut CT scan with 3D reconstructions provides invaluable, granular detail regarding the extent of joint destruction, the presence of subchondral cysts, the degree of bone loss, and the exact apex of the deformity. In cases where the pain generator is ambiguous, selective fluoroscopically-guided intra-articular diagnostic injections of local anesthetic can definitively isolate the symptomatic joints, guiding the extent of the planned arthrodesis.
Templating and Operative Setup
Preoperative templating involves determining the optimal hardware constructs and anticipating the need for bone grafting. If there is significant bone loss or a severe deformity requiring structural lengthening (e.g., restoring the lateral column after a nutcracker cuboid fracture), structural allograft or autograft (iliac crest) must be planned. For straightforward in situ fusions, local bone graft augmented with cancellous allograft or orthobiologics may suffice. The surgeon must mentally rehearse the sequence of joint preparation, deformity correction, and hardware application.

For this procedure, the patient is positioned supine on a radiolucent operating table. A bump or small pillow is placed under the ipsilateral hip to internally rotate the leg slightly, bringing the foot into a neutral position and allowing excellent access to the medial column. A well-padded thigh tourniquet is applied to provide a bloodless surgical field, which is absolutely critical for identifying neurovascular structures and ensuring meticulous joint preparation. The tourniquet is typically inflated to 250-300 mmHg after exsanguination with an Esmarch bandage. The C-arm fluoroscopy unit must be positioned to allow rapid, unimpeded access for AP, oblique, and lateral imaging without compromising the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
We now transition to the operative execution. The tourniquet is inflated, and we have established a pristine, bloodless field. Precision in exposure and joint preparation dictates the biological success of the arthrodesis.
Dual Dorsal Incisional Approach
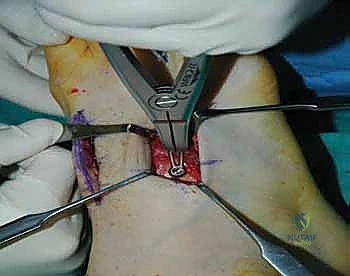
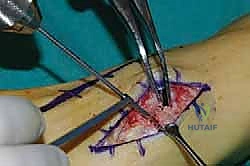
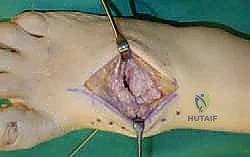
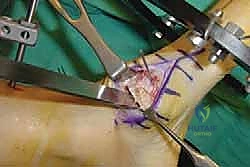
For a comprehensive midfoot arthrodesis involving the medial and middle columns, a dual dorsal longitudinal incisional approach provides optimal exposure while preserving a vital angiosome-based skin bridge. The medial incision is centered over the first and second TMT joints, extending from the midshaft of the first metatarsal proximally to the naviculocuneiform joint. The deep dissection must carefully identify and retract the EHL medially and the EHB laterally. Immediately deep to the EHB lies the deep neurovascular bundle (DPN and dorsalis pedis artery), which must be meticulously mobilized and protected throughout the procedure.

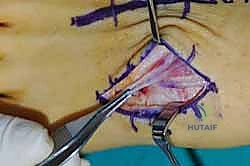
The lateral incision is placed over the third and fourth TMT joints, typically in line with the third metatarsal. It is imperative to maintain a wide skin bridge between the medial and lateral incisions—an absolute minimum of 5 to 7 centimeters—to prevent catastrophic skin necrosis. The superficial peroneal nerve branches are highly vulnerable during this lateral approach and must be identified and gently retracted using vessel loops. Deep dissection exposes the third TMT joint and the intercuneiform articulations. Subperiosteal flaps are raised carefully to expose the joint capsules, minimizing stripping to preserve the tenuous dorsal blood supply to the tarsal bones.
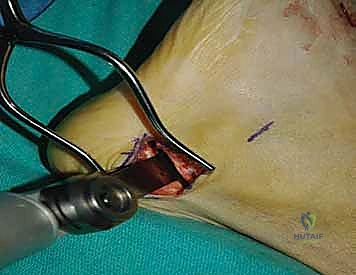
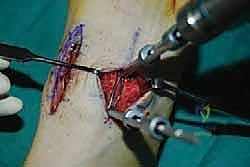
Radical Joint Preparation and Deformity Correction
The biological foundation of a successful arthrodesis is radical, meticulous joint preparation. The goal is to remove all articular cartilage and dense subchondral bone until healthy, bleeding cancellous bone is exposed on both sides of the articulation. I utilize a combination of sharp osteotomes, curettes, and high-speed burrs. For joints with minimal deformity, in situ preparation using a 2.0mm drill bit to aggressively "fish-scale" or "shingle" the subchondral plate is highly effective. This technique breaks the subchondral barrier, allowing for the ingress of osteoprogenitor cells and vascular ingrowth while preserving the native architecture and preventing shortening.
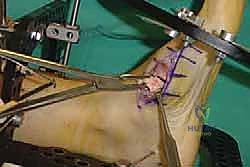
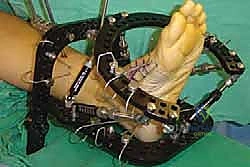
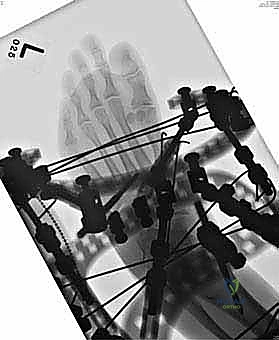
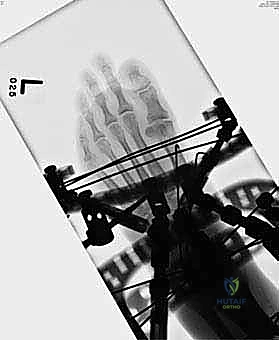
In cases of severe deformity, corrective osteotomies or planar resections may be required. If the forefoot is severely abducted, the medial joints (1st TMT) may require a closing wedge resection, or the lateral joints may require an opening wedge structural graft to restore colinearity. Deformity correction must proceed in a logical sequence. First, any equinus contracture is addressed via a percutaneous Achilles tendon lengthening or a gastrocnemius recession. Next, the forefoot abduction is corrected in the transverse plane, followed by restoration of the longitudinal arch in the sagittal plane. Temporary fixation is achieved using multiple stout Kirschner wires (0.062 inch). Fluoroscopy is utilized extensively at this stage to confirm absolute anatomic reduction; Meary's line must be perfectly restored on both AP and lateral views before any definitive hardware is placed.
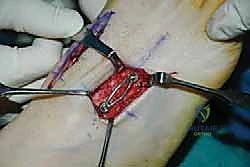
Definitive Rigid Internal Fixation
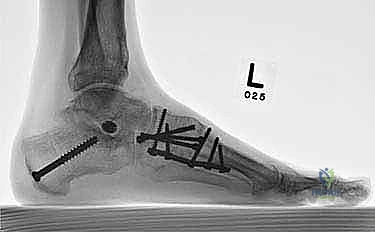
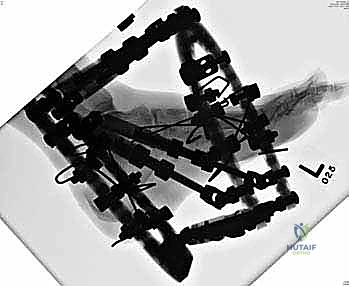
Once anatomic reduction is confirmed, we proceed with definitive rigid internal fixation. The biomechanical goal is to provide absolute stability and compression across the arthrodesis sites. For the medial column, I favor a combination of interfragmentary compression screws and dorsal or medial neutralization plating. The classic "homerun screw" is placed from the medial aspect of the medial cuneiform, directed distally and laterally into the base of the second metatarsal. This screw replicates the vector of the native Lisfranc ligament and provides immense stability to the keystone of the midfoot.

Following the homerun screw, individual solid or cannulated screws (typically 3.5mm or 4.0mm) are used to compress the 1st, 2nd, and 3rd TMT joints. The trajectory of these screws must be carefully planned to cross the joints perpendicular to the joint line to maximize compression and avoid shear forces. In highly unstable cases, or in neuropathic (Charcot) patients, dorsal spanning plates are applied over the TMT joints to act as a tension band, neutralizing the plantar-gapping forces experienced during weight-bearing. Recently, plantar plating techniques have gained popularity due to their superior biomechanical profile (placing the plate on the tension side of the foot), though the surgical approach is significantly more complex and carries higher risks to the plantar neurovascular structures. All hardware placement is meticulously verified with orthogonal fluoroscopic views before final closure.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, midfoot arthrodesis carries a significant risk profile. The surgeon must be prepared to identify and manage these complications aggressively.
Nonunion and Malunion
Nonunion is the most feared biological complication, with reported incidence rates ranging from 5% to 15% in standard post-traumatic cases, and exponentially higher in smokers or Charcot patients. The second and third TMT joints are particularly prone to nonunion due to their recessed anatomy and challenging preparation. Clinically, nonunion presents as persistent midfoot pain, swelling, and hardware failure (screw breakage or plate pullout) months after surgery. Management of a symptomatic nonunion requires revision surgery: removal of broken hardware, aggressive re-debridement of the nonunion site down to bleeding bone, application of structural autograft (usually iliac crest), and revision fixation using stiffer, more robust constructs, often incorporating locking plates and orthobiologic adjuncts (e.g., BMP-2).

Malunion occurs when the arthrodesis heals in a non-anatomic position. Residual forefoot abduction or a persistent midfoot sag alters the biomechanics of the entire lower extremity. A dorsiflexed first ray malunion will lead to devastating transfer metatarsalgia, overloading the lesser metatarsal heads and potentially causing intractable plantar keratoses or stress fractures. A plantarflexed first ray will cause sesamoiditis and hallux rigidus. Salvage of a symptomatic malunion is incredibly complex, requiring corrective osteotomies through the solid fusion mass, realignment, and complex revision fixation. Prevention through rigorous intraoperative fluoroscopic assessment is paramount.
Soft Tissue and Hardware Complications
Wound dehiscence and superficial infections are common, particularly with dorsal approaches where the soft tissue envelope is thin. Maintaining a wide skin bridge and utilizing meticulous, layered, tension-free closure techniques are essential preventative measures. Deep infections require immediate surgical debridement, hardware removal (if stability is compromised), and targeted intravenous antibiotics.
Hardware prominence is a frequent patient complaint, particularly over the medial cuneiform or the dorsal aspect of the first TMT joint. If the hardware becomes painful or causes skin irritation after solid radiographic union is achieved (typically after 6-12 months), elective hardware removal is a reasonable option. Iatrogenic nerve injury, particularly to the superficial peroneal nerve branches, can result in debilitating, painful neuromas. If conservative measures (gabapentinoids, desensitization, targeted injections) fail, surgical excision of the neuroma and burying the nerve stump into deep muscle or bone may be necessary.
| Complication | Estimated Incidence | Prevention and Salvage Management Strategies |
|---|---|---|
| Nonunion / Delayed Union | 5% - 15% (Higher in smokers/diabetics) | Prevention: Meticulous joint prep, rigid compression, strict NWB protocols. Salvage: Revision with structural autograft, BMP-2, and upgraded locking plate constructs. |
| Malunion (Residual Deformity) | 3% - 8% | Prevention: Rigorous intra-op fluoroscopy, Meary's line restoration. Salvage: Corrective closing/opening wedge osteotomies through the fusion mass. |
| Wound Dehiscence / Necrosis | 2% - 10% | Prevention: >5cm skin bridge, atraumatic soft tissue handling, tension-free closure. Salvage: Local wound care, negative pressure wound therapy, rarely local rotational flaps. |
| Symptomatic Hardware | 10% - 20% | Prevention: Low-profile implants, countersinking screw heads. Salvage: Elective hardware removal only after confirmed solid radiographic union (typically >9 months). |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a midfoot arthrodesis is lengthy and requires strict patient compliance. The protocol is divided into distinct, biologically driven phases.
Phase I: Maximum Protection (Weeks 0-2)
Immediately postoperatively, the patient is placed in a bulky, well-padded short leg splint. The primary goals during this phase are wound healing, edema control, and pain management. The patient is strictly non-weight-bearing (NWB) on the operative extremity. Strict elevation—keeping the foot above the level of the heart—is mandated for the first 48 to 72 hours to mitigate swelling, which can threaten the dorsal incisions. At the two-week mark, the patient returns to the clinic for splint removal, wound inspection, and suture removal. If the incisions are healing appropriately, the patient is transitioned into a removable controlled ankle motion (CAM) boot.

Phase II: Continued Protection and Early Motion (Weeks 2-6)
During this phase, the patient remains strictly non-weight-bearing. However, with the transition to the CAM boot, they are instructed to remove the boot multiple times a day to perform active range of motion (ROM) exercises of the ankle (dorsiflexion and plantarflexion) and the metatarsophalangeal joints, provided these joints were not pinned during the surgery. This early motion prevents profound stiffness and aids in edema mobilization. Radiographs are typically
Clinical & Radiographic Imaging Archive