Triple Arthrodesis

Comprehensive Introduction and Patho-Epidemiology
The triple arthrodesis remains a cornerstone in the armamentarium of the orthopedic foot and ankle surgeon, functioning as a definitive, albeit salvage-oriented, surgical intervention for severe, rigid, and complex deformities of the hindfoot. Historically conceptualized and popularized by Ryerson in 1923, the procedure involves the systematic fusion of the talocalcaneal (subtalar), calcaneocuboid, and talonavicular joints. While the advent of modern joint-sparing osteotomies and advanced orthotic management has narrowed its primary indications, triple arthrodesis is most commonly indicated for the salvage of severe, rigid deformities of the hindfoot that are entirely unresponsive to less invasive methods of treatment. The procedure effectively transforms a painful, deformed, and unstable hindfoot into a plantigrade, stable, and painless platform for ambulation.
The spectrum of deformities amenable to this procedure is broad, encompassing equinovarus, equinovalgus, and cavovarus, as well as their clinical variants including calcaneovalgus, calcaneovarus, calcaneocavus, and equinocavus. These complex multiplanar deformities rarely present as isolated bony anomalies; rather, they represent the terminal stage of a progressive pathophysiological cascade. While some deformities possess a structural component at birth—such as congenital vertical talus or severe syndromic clubfoot—the vast majority develop gradually. They typically begin as flexible deformities driven by dynamic muscle imbalances, progress to reducible soft tissue contractures, and ultimately culminate in fixed, rigid bony malalignment characterized by progressive adaptive changes in the osteocartilaginous structures.

The patho-epidemiology of these deformities is heavily rooted in neuromuscular pathology, though congenital and post-traumatic etiologies are also prevalent. An equinovarus deformity may be present at birth in a congenital clubfoot or may result from spastic muscle imbalance in patients with cerebral palsy (most frequently spastic hemiplegia) or flaccid muscle imbalance, such as that seen in poliomyelitis. Conversely, an equinovalgus deformity is most common in patients with a congenital vertical talus or cerebral palsy (most commonly spastic diplegia), while a rigid valgus hindfoot is frequently the sequela of an untreated tarsal coalition. The cavovarus foot is classically associated with hereditary motor and sensory neuropathies, most notably Charcot-Marie-Tooth (CMT) disease, where specific patterns of muscle denervation drive the progressive deformity.
Chronologically, this procedure has traditionally been reserved for older adolescents and adults to avoid the premature arrest of midfoot growth centers, which inevitably shortens the foot and can be cosmetically objectionable. However, contemporary literature and refined surgical techniques have demonstrated that triple arthrodesis can be successfully performed in children as young as 8 years of age in highly selected cases. In these younger cohorts, the deformity must be of such severity that it precludes bracing and ambulation, and the surgeon must meticulously avoid excessive resection of the cartilaginous anlagen. Despite these pediatric applications, the definitive timing of surgical intervention requires a delicate balance between arresting deformity progression and allowing for maximal skeletal maturation of the foot.
Detailed Surgical Anatomy and Biomechanics
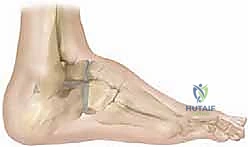
A profound understanding of the functional anatomy and interdependent biomechanics of the hindfoot joints—specifically the ankle, subtalar, talonavicular, and calcaneocuboid articulations—is mandatory for executing a successful triple arthrodesis. The ankle joint, functioning primarily as a hinge, dictates plantarflexion and dorsiflexion. Because the transmalleolar axis is externally rotated relative to the coronal plane, dorsiflexion is obligatorily associated with outward deviation (abduction) of the foot, while plantarflexion is associated with inward deviation (adduction). It is critical to differentiate true ankle equinus from midfoot equinus (a "midfoot break" or forefoot plantarflexion) to avoid the common and disastrous mistake of performing an isolated Achilles tendon lengthening when the pathology lies distal to the ankle joint.

The subtalar (talocalcaneal) joint represents the foundational linkage between the ankle mortise and the distal articulations of the foot. Anatomically, it consists of anterior, middle, and posterior facets, with the anterior and middle facets frequently confluent in a significant subset of patients. The spatial orientation of the subtalar joint axis is highly complex, averaging 23 degrees medially in the transverse plane and 42 degrees dorsally in the sagittal plane. This inclined axis allows the subtalar joint to function as a directional hinge, converting the transverse plane rotations of the tibia into coronal and sagittal plane movements of the foot. During a normal gait cycle, the subtalar joint everts at initial heel strike to unlock the midfoot for shock absorption, and subsequently inverts progressively to lock the midfoot, providing a rigid lever arm for terminal stance and push-off.
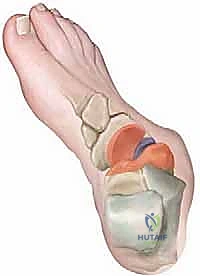
The talonavicular and calcaneocuboid joints collectively form the transverse tarsal joint (Chopart's joint), which operates in direct biomechanical synchrony with the subtalar joint. The mechanical coupling of these joints is a marvel of evolutionary engineering. When the calcaneus is everted (valgus), the axes of the talonavicular and calcaneocuboid joints become parallel, maximizing flexibility and accommodating uneven terrain during early stance. Conversely, when the calcaneus is inverted (varus), these axes become divergent and nonparallel, effectively locking the transverse tarsal joints into a rigid construct. In the setting of a fixed hindfoot deformity, this delicate locking and unlocking mechanism is obliterated, leading to massive compensatory stresses on adjacent joints and the development of severe degenerative arthrosis.

From a functional and dynamic standpoint, the pathogenesis of these deformities is intimately tied to the vectors of the muscles crossing the ankle and subtalar joints. Plantarflexion is driven by the gastrocnemius, soleus, tibialis posterior, flexor digitorum longus (FDL), and flexor hallucis longus (FHL), while dorsiflexion is powered by the tibialis anterior, extensor digitorum longus (EDL), and extensor hallucis longus (EHL). Inversion is controlled by the tibialis anterior and posterior, FDL, and FHL; eversion is dominated by the peroneus longus, brevis, and tertius. In conditions like Charcot-Marie-Tooth disease, a primary weakness of the tibialis anterior relative to a strong peroneus longus results in unrestrained plantarflexion of the first ray (forefoot valgus). To compensate for this fixed forefoot valgus and maintain a plantigrade foot during stance, the hindfoot is forced into a compensatory varus alignment. Over time, contractures of the plantar fascia and intrinsic muscles solidify this dynamic imbalance into a rigid cavovarus deformity.
Exhaustive Indications and Contraindications
The decision to proceed with a triple arthrodesis is predicated on the presence of a severe, rigid, and symptomatic hindfoot deformity that has proven entirely recalcitrant to exhaustive nonoperative management. The procedure is definitively indicated for the salvage of end-stage arthrosis of the subtalar and transverse tarsal joints, whether primary, post-traumatic, or inflammatory (e.g., rheumatoid arthritis) in nature. Furthermore, it is the procedure of choice for fixed neurogenic deformities, such as the rigid cavovarus foot seen in advanced Charcot-Marie-Tooth disease, severe spastic equinovalgus in cerebral palsy, or flaccid paralytic deformities secondary to poliomyelitis. In the realm of congenital anomalies, neglected or multiply recurrent clubfeet, severe rigid flatfoot secondary to an untreated tarsal coalition, and rigid congenital vertical talus represent primary indications when joint-sparing osteotomies are no longer viable.

Conversely, triple arthrodesis carries absolute and relative contraindications that must be rigorously respected to avoid catastrophic outcomes. The most critical absolute contraindication is the presence of an active, untreated infection in the foot or ankle, including osteomyelitis of the tarsal bones. Severe peripheral arterial disease that precludes adequate wound healing is also an absolute contraindication, necessitating vascular optimization prior to any reconstructive consideration. A relative, yet highly significant, contraindication is the presence of an insensate foot, such as that seen in severe myelomeningocele or advanced diabetic neuropathy. Performing a massive fusion in an insensate foot dramatically increases the risk of postoperative Charcot neuroarthropathy, hardware failure, and devastating ulceration at adjacent joints due to altered biomechanical stress profiles.
Furthermore, the age of the patient plays a pivotal role in the decision-making process. While not an absolute contraindication, performing a triple arthrodesis in young children (typically under the age of 8 to 10 years) is strongly discouraged. The procedure requires the excision of osteocartilaginous wedges, which invariably damages the growth potential of the tarsal bones, leading to a severely shortened and functionally compromised foot at skeletal maturity. In these younger populations, extra-articular procedures, such as the Grice-Green subtalar arthrodesis or extensive soft tissue releases, are preferred to bridge the patient until skeletal maturity is reached.
Finally, a critical caveat in the indication for triple arthrodesis is the necessity of addressing the underlying dynamic muscle imbalance. Performing a bony fusion without concurrently balancing the deforming muscular forces (via appropriate tendon transfers or lengthenings) is a recipe for surgical failure. If the deforming forces are left unchecked, the deformity will inexorably recur, either through the fusion mass (causing malunion or pseudarthrosis) or by transferring the deforming forces to the adjacent ankle or midfoot joints, leading to rapid and severe adjacent segment disease.
Indications and Contraindications Summary
| Category | Specific Conditions / Factors |
|---|---|
| Primary Indications | Rigid cavovarus (CMT), Spastic equinovalgus (Cerebral Palsy), Flaccid equinovarus (Polio), Neglected/Recurrent Clubfoot. |
| Secondary Indications | End-stage post-traumatic arthrosis, Rheumatoid arthritis of the hindfoot, Stage IV Posterior Tibial Tendon Dysfunction. |
| Absolute Contraindications | Active local or systemic infection, Severe peripheral vascular disease, Medically unstable patient. |
| Relative Contraindications | Insensate foot (Myelomeningocele, severe diabetic neuropathy), Young age (< 8-10 years), Unaddressed dynamic muscle imbalance. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the bedrock of a successful triple arthrodesis, beginning with a comprehensive and nuanced physical examination. The surgeon must meticulously evaluate the skin for the presence and location of callosities, which serve as a roadmap to the abnormal weight-bearing mechanics of the foot. A rigorous assessment of the relationship between the forefoot and hindfoot is paramount. The Coleman block test is absolutely critical in the evaluation of the cavovarus foot; by placing the patient's lateral heel and foot on a wooden block and allowing the plantarflexed first ray to drop off the edge, the surgeon can definitively determine if the hindfoot varus is flexible (driven by the forefoot valgus) or rigid (requiring structural correction). Manual muscle testing must be systematically performed to assess the relative strengths of motor units across the ankle and subtalar joints, dictating the necessity and type of adjunctive tendon transfers.
Radiographic evaluation demands high-quality, weight-bearing imaging in all cases. A standard series includes standing anteroposterior (AP) and lateral radiographs of the foot, as well as a standing AP of the ankle to rule out compensatory or primary ankle joint pathology. On the standing AP radiograph, the talocalcaneal (Kite) angle is measured (normal range: 10 to 56 degrees); values less than 20 degrees suggest hindfoot varus, while angles exceeding 40 to 50 degrees indicate hindfoot valgus. The talus–first metatarsal angle is also assessed (normal range: 10 to 30 degrees), with deviations indicating forefoot varus or valgus. On the standing lateral radiograph, the lateral talocalcaneal angle (normal: 25 to 55 degrees) and the tibiocalcaneal angle (normal: 55 to 95 degrees) are crucial for quantifying equinus, calcaneus, varus, and valgus deformities. The lateral talus–first metatarsal angle (Meary’s angle) dictates the presence of midfoot cavus (>20 degrees) or a midfoot break (<0 degrees).

Advanced imaging modalities, such as Computed Tomography (CT) or Magnetic Resonance Imaging (MRI), are selectively deployed. A fine-cut CT scan with 3D reconstructions is invaluable in cases of suspected tarsal coalition, severe post-traumatic distortion of the bony anatomy, or when assessing the quality of the remaining bone stock for hardware purchase. MRI is less frequently utilized for the bony planning of a triple arthrodesis but may be indicated if there is a suspicion of avascular necrosis of the talus or to evaluate the integrity of specific tendon complexes (e.g., the posterior tibial tendon or peroneal tendons) prior to planned transfers. Preoperative templating on digital radiographs is essential to estimate the size, location, and geometry of the bony wedges that must be resected to achieve a plantigrade foot without excessive shortening.
Patient positioning in the operating room must be optimized to provide simultaneous access to both the medial and lateral aspects of the hindfoot. The patient is typically placed in the supine position on a radiolucent operating table. Because the lower extremity naturally rests in external rotation, a well-padded bump is placed under the ipsilateral hip to internally rotate the leg until the patella points directly toward the ceiling. This neutral rotation is critical for accurately assessing the alignment of the foot relative to the transmalleolar axis intraoperatively. A pneumatic tourniquet is applied around the proximal thigh to ensure a bloodless surgical field, which is vital for the meticulous identification of neurovascular structures and the thorough denudation of articular cartilage. Fluoroscopy is positioned to enter from the contralateral side of the table, allowing for unobstructed AP, lateral, and oblique views of the foot throughout the procedure.

Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of a triple arthrodesis is traditionally performed via a dual-incision technique, providing comprehensive access to the intricate anatomy of the hindfoot while minimizing soft tissue complications. The primary lateral incision is made from the tip of the lateral malleolus, extending distally and slightly anteriorly toward the base of the fourth metatarsal. This approach provides direct access to the subtalar and calcaneocuboid joints. The sural nerve and lesser saphenous vein must be carefully identified and protected during the superficial dissection. The extensor digitorum brevis (EDB) muscle belly is sharply elevated from its origin on the lateral calcaneus and reflected distally, exposing the calcaneocuboid joint and the lateral aspect of the subtalar joint. The contents of the sinus tarsi, including the interosseous talocalcaneal ligament and the cervical ligament, are aggressively evacuated to fully visualize the posterior, middle, and anterior facets of the subtalar joint.
The medial incision is centered over the talonavicular joint, typically extending from the anterior margin of the medial malleolus to the navicular tuberosity. Extreme care must be taken to protect the saphenous nerve and vein superficially, and the tibialis anterior and posterior tibial tendons deeper in the wound. The capsule of the talonavicular joint is incised longitudinally. It is of paramount importance to limit the dorsal and plantar stripping of the talar neck during this exposure to preserve its tenuous blood supply and mitigate the catastrophic risk of iatrogenic avascular necrosis of the talus. Once all three joints are adequately exposed, the meticulous preparation of the fusion beds commences.

Correction of the rigid deformity is achieved through the precise resection of biplanar osteocartilaginous wedges. The fundamental principle of wedge resection is that the base of the excised wedge must be located on the convex side of the deformity. For instance, in a severe cavovarus deformity, a dorsolateral-based wedge is resected from the midtarsal joints to correct both the varus and the midfoot equinus, while a lateral-based wedge is taken from the subtalar joint to correct the hindfoot varus. The articular cartilage and subchondral bone are deeply denuded using osteotomes, curettes, and high-speed burrs until punctate bleeding (the "paprika sign") is observed, ensuring a biologically active bed for arthrodesis. The surgeon must constantly balance the need for complete deformity correction with the imperative to minimize foot shortening.

Following the resection of the wedges, the foot is manually reduced into a plantigrade position—defined by neutral to slight valgus alignment of the hindfoot (0 to 5 degrees), neutral dorsiflexion/plantarflexion, and a forefoot that is parallel to the floor. The joints are provisionally stabilized using large-diameter Kirschner wires. The sequence of definitive fixation is critical: the subtalar joint is typically secured first, followed by the talonavicular, and finally the calcaneocuboid joint. Fixation of the subtalar joint is most commonly achieved with one or two large (6.5 mm or 7.0 mm) cannulated lag screws directed from the posterior calcaneal tuberosity into the body and dome of the talus. For the transverse tarsal joints, biomechanical studies have demonstrated no significant difference in stability when comparing fixation with memory-compression staples versus smaller (4.0 mm or 4.5 mm) cannulated screws. Any remaining osseous defects are meticulously packed with autogenous bone graft (harvested from the resected wedges or proximal tibia) or structural allograft to optimize the fusion environment.

Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, triple arthrodesis is associated with a distinct profile of postoperative complications, ranging from minor wound healing issues to catastrophic hardware failure and nonunion. The most dreaded complication is pseudarthrosis (nonunion), which occurs most frequently at the talonavicular joint. The talonavicular joint's inherent spherical geometry, its extensive arc of motion, and the difficulty in achieving rigid compression across its complex surfaces contribute to a nonunion rate reported to be between 5% and 15% in the literature. Subtalar and calcaneocuboid nonunions are comparatively rare. A symptomatic pseudarthrosis typically presents with persistent midfoot pain, swelling, and radiographic evidence of a lucent line or hardware breakage. Salvage management necessitates a revision arthrodesis, which often requires the aggressive debridement of fibrous tissue, the utilization of structural autograft (e.g., iliac crest) to restore column length, and augmented rigid internal fixation, frequently supplemented with orthobiologics.

Malunion is another significant complication, resulting from either the undercorrection of the primary deformity or iatrogenic overcorrection. A common pitfall is the failure to recognize and correct a rigid forefoot valgus; if the hindfoot is fused in neutral but the forefoot remains in valgus, the patient will experience severe lateral column overload, leading to intractable callosities under the 5th metatarsal base and recurrent pain. Conversely, fixing the hindfoot in excessive varus eliminates the shock-absorbing capacity of the foot and dramatically accelerates adjacent joint arthrosis. Salvage of a symptomatic malunion is highly complex and may require profound reconstructive efforts, including supramalleolar osteotomies, midfoot corrective osteotomies, or a complete takedown and revision of the triple arthrodesis.

The long-term natural history of a successful triple arthrodesis almost invariably includes the development of adjacent joint arthrosis, specifically at the ankle joint and the tarsometatarsal articulations. Because the arthrodesis completely eliminates the compensatory motion and shock absorption of the subtalar and transverse tarsal joints, these mechanical stresses are transferred directly to the ankle mortise. Long-term follow-up studies indicate that up to 50% of patients will develop radiographic evidence of ankle arthritis within 10 to 20 years postoperatively. While not all radiographic arthritis is clinically symptomatic, patients developing severe, intractable ankle pain may ultimately require an ankle arthrodesis or total ankle arthroplasty as a definitive salvage procedure.
Complications and Salvage Management Summary
| Complication | Estimated Incidence | Primary Etiology / Risk Factor | Salvage Management Strategy |
|---|---|---|---|
| Talonavicular Nonunion | 5% - 15% | Spherical joint geometry, inadequate compression, smoking. | Revision arthrodesis with structural autograft and rigid plate/screw fixation. |
| Malunion (Varus/Valgus) | 5% - 10% | Poor preoperative templating, failure to address forefoot alignment. | Corrective midfoot or supramalleolar osteotomy; revision fusion. |
| Adjacent Joint Arthrosis | > 50% at 15 years | Altered biomechanics, loss of hindfoot shock absorption. |
Clinical & Radiographic Imaging Archive