Comprehensive Surgical Management of the Cavus Foot and Lambrinudi Arthrodesis
Key Takeaway
The surgical management of the cavus foot requires a meticulous understanding of multiplanar deformity, joint flexibility, and underlying neuromuscular etiology. While triple arthrodesis remains a powerful tool for achieving a plantigrade foot, procedures like the Lambrinudi arthrodesis are specifically indicated for fixed equinus and drop foot deformities. This guide details the biomechanical principles, preoperative templating, and step-by-step surgical execution required to optimize patient outcomes and minimize adjacent joint degeneration.
Comprehensive Introduction and Patho-Epidemiology
The cavus foot presents one of the most profoundly complex biomechanical challenges encountered in orthopedic foot and ankle surgery. Characterized fundamentally by an abnormally high medial longitudinal arch, the deformity is rarely isolated and is frequently accompanied by a constellation of structural abnormalities, including hindfoot varus, forefoot pronation, and rigid plantarflexion of the first ray (cavovarus). The etiology of the cavus foot is overwhelmingly neuromuscular in origin, with Charcot-Marie-Tooth (CMT) disease—specifically the type 1A variant involving the PMP22 gene duplication—accounting for the vast majority of hereditary cases. Other significant etiologies include poliomyelitis, spinal dysraphism (such as myelomeningocele), cerebral palsy, Friedreich’s ataxia, and post-traumatic sequelae following compartment syndrome or severe lower extremity crush injuries.
Understanding the patho-epidemiology of the cavus foot requires a meticulous analysis of the progressive muscle imbalances that drive the deformity. In classic CMT disease, the intrinsic musculature of the foot and the anterior compartment of the leg undergo progressive denervation and weakness earlier than the extrinsic musculature. Specifically, the profound weakness of the tibialis anterior allows the relatively preserved peroneus longus to overpower the first ray, driving it into rigid plantarflexion. Simultaneously, weakness of the peroneus brevis allows the robust tibialis posterior to invert the hindfoot, creating a relentless varus moment. Over time, these dynamic muscular imbalances transition from flexible, reducible deformities into rigid, fixed osseous adaptations that severely compromise the weight-bearing mechanics of the foot.
Successful surgical management mandates a profound understanding of these evolving biomechanics, a meticulous clinical examination, and a highly tailored surgical approach that addresses both the bony architecture and the underlying soft-tissue imbalances. The primary goal is never merely cosmetic correction; rather, it is the restoration of a stable, plantigrade, and sensate foot capable of accommodating the immense ground reaction forces encountered during the gait cycle. In the presence of progressive neuromuscular decline, the surgeon must balance the desire for joint-sparing, soft-tissue procedures with the pragmatic reality that definitive osseous stabilization—such as the Lambrinudi arthrodesis—may ultimately be required to prevent catastrophic adjacent joint breakdown and recalcitrant ulceration.
Furthermore, the surgeon must recognize that the adolescent cavus foot behaves drastically differently than the adult cavus foot. Triple arthrodesis performed in adolescents with Charcot-Marie-Tooth disease is significantly less likely to produce satisfactory long-term results than when performed in adults over 40 years of age. The adolescent foot lacks the adaptive capacity of the mature skeleton, and progressive neuromuscular imbalance can lead to severe adjacent joint breakdown, particularly at the tibiotalar articulation. Therefore, joint-sparing osteotomies and tendon transfers are heavily favored in the younger demographic, reserving complex arthrodesis for end-stage, rigid deformities or severe paralytic conditions.
Detailed Surgical Anatomy and Biomechanics
The surgical anatomy of the cavus foot is dictated by the complex interplay of the osseous architecture, the ligamentous restraints, and the dynamic muscular forces acting across the subtalar and transverse tarsal (Chopart) joints. The hallmark of the cavovarus foot is the plantarflexed first ray, which acts as a rigid kickstand during the stance phase of gait. As the patient bears weight on this plantarflexed medial column, the ground reaction force drives the forefoot into pronation. To keep the foot flat on the ground, the hindfoot is forced into a compensatory varus alignment. This phenomenon, known as a forefoot-driven hindfoot varus, is the critical biomechanical concept underpinning the Coleman block test. If the hindfoot corrects to neutral when the first ray is allowed to drop off a block, the deformity is flexible; if the hindfoot remains in varus, the subtalar joint has undergone fixed, rigid adaptation.
The osseous anatomy of the midfoot and hindfoot in a cavus deformity undergoes significant morphologic alteration over time. The talus is often dorsiflexed within the ankle mortise to compensate for the severe plantarflexion of the forefoot, leading to a functional equinus. The calcaneus exhibits an increased pitch angle, and the navicular is frequently subluxated dorsally and laterally relative to the talar head. The ligamentous structures, particularly the spring ligament complex (calcaneonavicular ligaments) and the plantar fascia, become severely contracted, further tethering the medial column in its exaggerated arch configuration. The lateral ligamentous complex, specifically the anterior talofibular and calcaneofibular ligaments, is subjected to chronic attenuation due to the relentless varus thrust, predisposing the patient to chronic lateral ankle instability.
For patients presenting with a paralytic drop foot or severe, fixed equinus deformity—historically common in poliomyelitis but now seen in severe peripheral neuropathies—the Lambrinudi arthrodesis offers a specialized biomechanical solution. The biomechanical genius of the Lambrinudi procedure lies in its exploitation of the anterior capsule of the ankle joint. By surgically locking the talus in maximal equinus (plantarflexion) within the ankle mortise, the anterior capsule becomes maximally taut, preventing any further plantarflexion of the talar body. The remainder of the foot is then fused to the talus in a neutral or slightly equinus position.
Consequently, when the patient attempts to bear weight or swing the leg during the swing phase of gait, the locked talus prevents the foot from dropping into equinus. This effectively substitutes for the absent or profoundly weak ankle dorsiflexors (tibialis anterior, extensor hallucis longus, extensor digitorum longus). However, this delicate biomechanical construct completely relies on the integrity of the anterior ankle capsule and the precise geometry of the bony wedge resected from the talus. Any error in templating or execution can result in either residual drop foot or an unacceptable calcaneus deformity, drastically altering the biomechanics of the entire lower extremity kinetic chain.
Exhaustive Indications and Contraindications
The decision-making process for executing a triple arthrodesis or a highly specialized Lambrinudi arthrodesis is dictated by a systematic, algorithm-driven evaluation of the deformity. The surgeon must ascertain whether the deformity is multiplanar, whether it is forefoot- or hindfoot-driven, and most importantly, whether the components are fixed or flexible. Fixed deformities necessitate structural bony correction via arthrodesis or osteotomy, whereas flexible deformities may respond to aggressive soft-tissue balancing. The Lambrinudi procedure, specifically, is reserved for a very distinct subset of patients who present with severe, rigid equinus or paralytic drop foot that cannot be managed with an Ankle-Foot Orthosis (AFO) or isolated tendon transfers.
A critical prognostic determinant is the presence of a sensory deficit. The presence of profound peripheral neuropathy drastically alters the surgical algorithm. In an insensate foot, the surgeon must adhere to the clinical pearl: the least that can be done to alleviate a specific symptom is often the best treatment. Over-correction, excessive rigid fixation, or prolonged immobilization in an insensate foot dramatically increases the risk of Charcot neuroarthropathy, hardware failure, and recalcitrant plantar ulcerations. Therefore, arthrodesis in the neuropathic patient must be approached with extreme caution, utilizing ultra-rigid fixation constructs and extended periods of non-weight-bearing.
Contraindications to the Lambrinudi and traditional triple arthrodesis include flexible deformities that are fully correctable with soft-tissue procedures, active deep space infections, and severe peripheral vascular disease that precludes adequate soft-tissue healing. Furthermore, significant pre-existing degenerative joint disease of the tibiotalar (ankle) joint is a relative contraindication to a Lambrinudi arthrodesis. Because the Lambrinudi procedure locks the talus in equinus and forces the ankle to accommodate the entire sagittal plane motion of the foot, pre-existing ankle arthritis will rapidly accelerate, leading to debilitating pain and potentially necessitating a subsequent pantalar arthrodesis.
| Clinical Parameter | Indications for Lambrinudi / Triple Arthrodesis | Contraindications (Absolute & Relative) |
|---|---|---|
| Deformity Flexibility | Rigid, fixed hindfoot varus and unyielding equinus | Flexible deformity correctable via Coleman block test |
| Neuromuscular Status | Paralytic drop foot (Polio), severe progressive CMT | Spasticity overpowering potential arthrodesis (Relative) |
| Ankle Joint Health | Pristine tibiotalar cartilage with preserved motion | Pre-existing moderate-to-severe tibiotalar arthritis |
| Sensory Function | Intact sensation or mild neuropathy | Profound sensory neuropathy / Charcot arthropathy (Relative) |
| Vascular Status | Palpable pulses, ABI > 0.9, brisk capillary refill | Severe peripheral arterial disease, ABI < 0.5 (Absolute) |
| Age and Skeletal Maturity | Skeletally mature adults (typically > 40 years for best outcomes) | Skeletally immature adolescents (high risk of adjacent joint disease) |
Pre-Operative Planning, Templating, and Patient Positioning
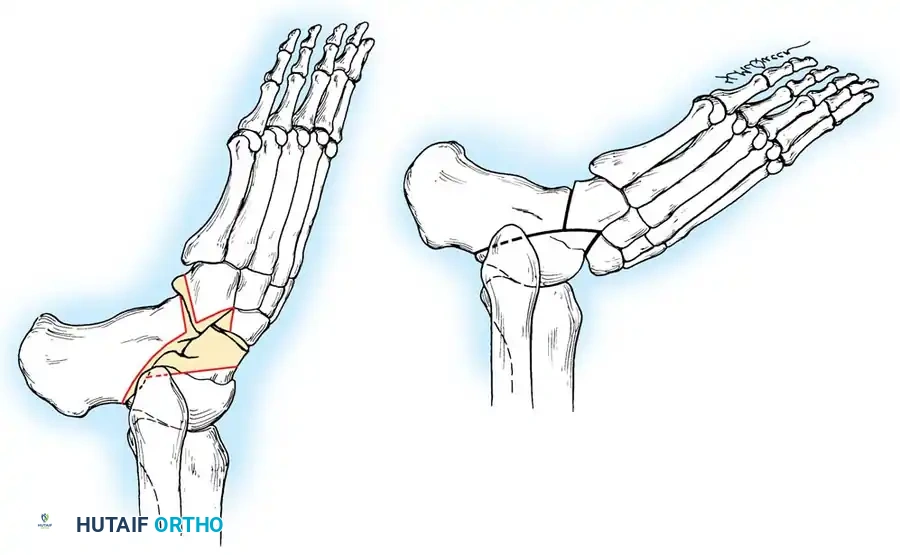
Accurate preoperative planning is the absolute cornerstone of a successful Lambrinudi arthrodesis. Unlike a standard triple arthrodesis where the joint surfaces are simply denuded of cartilage and contoured in situ, the Lambrinudi procedure requires the precise mathematical resection of a geometric wedge from the talus to achieve the desired postoperative alignment. The exact dimensions of this bony wedge must be calculated meticulously before the patient ever enters the operating theater to ensure the foot is perfectly plantigrade postoperatively.
The templating process begins with obtaining a strict, weight-bearing lateral radiograph of the foot and ankle with the ankle held in extreme, maximal plantarflexion. This position mimics the final locked position of the talus within the mortise. The surgeon then traces the radiographic film onto acetate paper, or more commonly in modern practice, utilizes advanced digital orthopedic templating software. The tracing is cut into three distinct pieces along the outlines of the subtalar and midtarsal joints. From these pieces, the surgeon determines the exact amount of bone to be removed from the plantar and distal aspects of the talar body and neck.
A crucial alignment principle during templating is that the line representing the tibiotalar articulation must be left completely undisturbed. The line corresponding to the plantar and distal parts of the talus is angled and cut so that when the navicular and calcaneocuboid joints are fitted to it, the foot rests in slight equinus relative to the tibia. The final position of the foot should be templated to exactly 5 to 10 degrees of equinus. If the affected extremity has a significant limb length discrepancy (shortening), which is common in polio survivors, slightly more equinus may be desirable to assist with limb length equalization.
Patient positioning and operating room setup must facilitate unhindered access to the lateral and posterior aspects of the hindfoot. The patient is typically placed in the lateral decubitus position, or alternatively, in the supine position with a large, firm bump placed under the ipsilateral hip. This bump internally rotates the leg, bringing the lateral malleolus and the sinus tarsi directly into the surgeon's primary visual field. A proximal thigh tourniquet is applied over copious padding, and the entire lower extremity is prepped and draped free to allow for dynamic intraoperative assessment of ankle dorsiflexion and hindfoot alignment. Fluoroscopy must be positioned to easily enter the field for orthogonal intraoperative imaging.
Step-by-Step Surgical Approach and Fixation Technique
The surgical exposure for the Lambrinudi arthrodesis is classically performed through a long, laterally based curved incision, often referred to as an extended Ollier approach. The incision begins approximately 2 centimeters distal and posterior to the tip of the lateral malleolus, curving gently across the sinus tarsi, and extending distally toward the base of the fourth metatarsal. Meticulous subcutaneous dissection is required to identify and protect the sural nerve and the lesser saphenous vein, which frequently cross the posterior and inferior margins of the incision. The inferior extensor retinaculum is sharply incised and mobilized as a continuous flap, which will later be utilized for closure and coverage of the arthrodesis sites.
Deep dissection involves exposing the peroneal tendon sheath. The peroneus longus and brevis tendons are carefully sectioned using a Z-shaped cut. This step is critical; it not only allows for unhindered, wide exposure of the subtalar and calcaneocuboid joints but also permits the subsequent repair of these tendons under appropriate tension, which is vital for postoperative dynamic stabilization. Following tendon retraction, the talonavicular and calcaneocuboid joints are widely opened. To sufficiently mobilize the hindfoot, the surgeon must sharply divide the interosseous talocalcaneal ligament located deep within the sinus tarsi, as well as the fibular collateral ligaments of the ankle if necessary. This extensive soft-tissue release permits the complete medial dislocation of the tarsus at the subtalar joint, fully exposing the articular surfaces of the talus and calcaneus.
Bony resection is the most technically demanding phase of the procedure. A small, high-speed oscillating power saw is highly recommended over the use of chisels or osteotomes. Osteotomes can cause microfractures and uncontrolled propagation of fracture lines into the fragile talar body, potentially leading to avascular necrosis. A power saw provides the precise, planar cuts required for the complex geometric fit of the Lambrinudi procedure. The predetermined wedge of bone is meticulously resected from the plantar and distal parts of the neck and body of the talus, mirroring the preoperative template. Next, the cartilage and subchondral bone are removed from the superior surface of the calcaneus to form a perfectly flat plane that is strictly parallel with the longitudinal axis of the foot.
The midfoot is then prepared by making a precise V-shaped trough transversely in the inferior part of the proximal navicular. The calcaneocuboid joint is denuded of enough bone to correct any pre-existing lateral or varus deformity. Reduction involves firmly wedging the sharp, newly created distal margin of the remaining talus into the prepared V-shaped trough in the navicular, while simultaneously apposing the raw osseous surfaces of the calcaneus and talus. A critical positioning step is placing the distal margin of the talus well medially within the navicular trough. Failure to translate the talus medially will result in an unsatisfactory, lateralized position of the foot, exacerbating forefoot pronation. Furthermore, no attempt should be made to compensate in the foot for any pre-existing tibial torsion; attempting to derotate the foot through the arthrodesis will severely compromise the bony contact area and lead to nonunion. Once the talus is mechanically locked in the ankle joint in complete equinus, the arthrodesis sites are secured using modern rigid internal fixation, such as large fragment (6.5mm or 7.3mm) cannulated compression screws, ensuring absolute stability across the subtalar, talonavicular, and calcaneocuboid joints.
Complications, Incidence Rates, and Salvage Management
The Lambrinudi arthrodesis, while a powerful reconstructive tool, carries a significant risk profile due to the extensive bony resections, the complex geometric requirements for stable reduction, and the inherently compromised soft-tissue envelope of the dysvascular or neuropathic limb. Nonunion and delayed union are among the most frequent complications, with the talonavicular joint being the most notorious site for pseudoarthrosis. The talonavicular joint is inherently difficult to compress and has a tenuous blood supply, particularly after the extensive stripping required for the Lambrinudi exposure. Malunion is another severe complication, most commonly presenting as residual hindfoot varus or inadequate equinus locking, which completely negates the biomechanical purpose of the procedure and leaves the patient with a persistent drop foot.
When managing the cavus foot, the surgeon must also be acutely aware of concurrent nerve entrapment syndromes, which can severely complicate the postoperative recovery if left unaddressed. The altered biomechanics of the cavovarus foot—specifically the rigid hindfoot varus and forefoot overload—predispose patients to secondary neuropathies. The tibial nerve and its branches are highly susceptible to traction and compression within the fibro-osseous tarsal tunnel. In the cavovarus foot, the varus alignment of the calcaneus increases tension on the flexor retinaculum. Patients frequently present with burning pain and paresthesias radiating into the plantar aspect of the foot. When performing reconstructive bony surgery for the cavus foot, concurrent tarsal tunnel release should be strongly considered if preoperative electrodiagnostic studies confirm entrapment.
Similarly, the cavus foot architecture inherently forces the metatarsals into a more plantarflexed position, drastically increasing forefoot contact pressures during the terminal stance phase of gait. This mechanical overload frequently leads to perineural fibrosis of the common digital nerve, most commonly in the third intermetatarsal space, known as Morton's Neuroma. Diagnosis is primarily clinical, characterized by sharp, burning forefoot pain and a palpable Mulder's click. If conservative measures fail, surgical excision of the neuroma via a dorsal approach is highly effective and can be performed concurrently with the hindfoot reconstruction. The surgeon must ensure the nerve is resected well proximal to the deep transverse metatarsal ligament to prevent the formation of a symptomatic stump neuroma in the weight-bearing area.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Prevention |
|---|---|---|---|
| Talonavicular Nonunion | 5% - 15% | Inadequate compression, thermal necrosis from saw, smoking | Revision arthrodesis with structural bone graft and rigid plate fixation |
| Residual Drop Foot | 5% - 10% | Inadequate wedge resection, failure to lock talus in maximal equinus | Revision osteotomy, AFO bracing, or conversion to pantalar arthrodesis |
| Adjacent Joint Arthritis | 40% - 60% (at 10+ years) | Increased stress on tibiotalar joint due to locked hindfoot | Conservative management (bracing, injections), Tibiotalar arthrodesis |
| Sural Nerve Injury | 2% - 8% | Iatrogenic transection or traction during the extended Ollier approach | Meticulous dissection, nerve mapping; excision and burying of stump if neuroma forms |
| Wound Dehiscence | 3% - 7% | Poor soft-tissue envelope, premature suture removal, severe edema | Prolonged immobilization, negative pressure wound therapy, rotational flaps |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a Lambrinudi arthrodesis is a protracted and meticulously phased process, requiring strict patient compliance and close clinical monitoring. Due to the massive osseous resections and the reliance on absolute bony stability for successful fusion, the initial phase of recovery is heavily focused on protecting the fixation construct and managing the inevitable soft-tissue edema. Phase 1 spans from postoperative day zero to six weeks. During this critical window, the patient is maintained strictly non-weight-bearing. Immediately following surgery, the limb is placed in a rigid, well-padded short-leg cast in the exact corrected position. Strict elevation above the level of the heart is mandatory for the first two weeks to mitigate postoperative swelling and reduce the risk of wound dehiscence. Deep vein thrombosis (DVT) prophylaxis is routinely administered during this non-weight-bearing period, tailored to the patient's individual risk profile.
Phase 2 encompasses weeks six through twelve. At the six-week mark, the initial cast is removed, and high-quality, multi-planar radiographs are obtained to assess for early trabecular bridging across the subtalar, talonavicular, and calcaneocuboid arthrodesis sites. If clinical examination reveals an absence of pain at the fusion sites and radiographic signs of union are progressing satisfactorily, the patient is transitioned to a removable controlled ankle motion (CAM) boot. Progressive partial weight-bearing is initiated, typically starting at 20% of body weight and advancing slowly under the guidance of a physical therapist. During this phase, active range of motion of the toes and isometric strengthening of the proximal musculature (quadriceps, hamstrings, gluteals) are heavily emphasized to prevent profound deconditioning.
Phase 3 begins at twelve weeks and extends indefinitely. Full weight-bearing is only permitted once solid bony union is unequivocally confirmed on orthogonal radiographs or, if clinically ambiguous, via a fine-cut computed tomography (CT) scan. Once full weight-bearing is achieved, the patient is transitioned out of the CAM boot into supportive athletic footwear. Custom orthotics or a specialized ankle-foot orthosis (AFO) may be utilized to support the transverse arch, accommodate any residual muscular imbalances, and protect the adjacent tibiotalar joint from excessive shear forces. Physical therapy focuses on proprioceptive retraining, gait mechanics optimization, and maximizing the functional capacity of the salvaged limb.
Summary of Landmark Literature and Clinical Guidelines
The evolution of the surgical management of the cavus foot is deeply rooted in historical orthopedic literature, with the Lambrinudi arthrodesis representing a paradigm shift in the treatment of paralytic deformities. First described by Constantine Lambrinudi in 1927, the procedure was revolutionary for its time, offering a purely mechanical solution to the devastating drop foot deformities caused by the rampant poliomyelitis epidemics. Lambrinudi's original insight—that the anterior capsule of the ankle could act as a robust check-rein if the talus was locked in equinus—remains a foundational concept in foot and ankle biomechanics. Subsequent landmark studies by authors such as Saltzman and Myerson have further refined the indications for hindfoot arthrodesis, emphasizing the critical importance of concurrent soft-tissue balancing and the preservation of adjacent joint mechanics whenever feasible.
Modern clinical guidelines, heavily influenced by long-term outcome studies in Charcot-Marie-Tooth populations, advocate for a staged, joint-sparing approach as the primary line of defense against the progressive cavovarus foot. The contemporary consensus dictates that osteotomies (such as a dorsiflexing first metatarsal osteotomy or a lateralizing calcaneal osteotomy) combined with tendon transfers (like the Jones or Hibbs procedures) should be exhausted before resorting to a triple arthrodesis. Arthrodesis is now largely reserved as a salvage procedure for rigid, end-stage deformities accompanied by severe arthrosis.
When arthrodesis is deemed necessary, current guidelines stress the absolute necessity of achieving a plantigrade foot. The literature overwhelmingly demonstrates that residual varus malalignment following a triple or Lambrinudi arthrodesis leads to catastrophic failure, characterized by lateral column overload, recalcitrant fifth metatarsal base ulcerations, and rapid degeneration of the ankle mortise. Therefore, meticulous preoperative templating, precise intraoperative execution with modern rigid fixation, and a profound respect for the underlying neuromuscular pathology remain the undisputed pillars of successful cavus foot reconstruction.
🔗 Read the comprehensive guide: Operative Principles of Lower Extremity Arthrodesis: Ankle and Knee
