Total Wrist Arthrodesis & Scaphoid Subluxation Guide

Key Takeaway
Total wrist arthrodesis is a highly reliable salvage procedure for end-stage radiocarpal and midcarpal arthritis. Utilizing the Weiss and Hastings technique with a contoured dynamic compression plate ensures rigid fixation and optimal positioning. Concurrently, recognizing rotary subluxation of the scaphoid—often presenting with a positive Watson shift test and dorsal intercalated segment instability (DISI)—is critical to preventing progressive carpal collapse and advanced arthritic degeneration.
Comprehensive Introduction and Patho-Epidemiology
Total wrist arthrodesis remains the unequivocal gold-standard salvage procedure for patients suffering from end-stage pancarpal arthritis, severe carpal instability, paralytic deformities, and debilitating post-traumatic conditions. Historically, the evolution of wrist fusion techniques has transitioned from the use of non-rigid fixation methods, such as Steinmann pins and Rush rods combined with prolonged cast immobilization, to the modern era of rigid internal fixation. The advent of the dorsal spanning plate, popularized by Weiss and Hastings, revolutionized the procedure by providing superior biomechanical stability, achieving fusion rates exceeding 95%, and drastically reducing the need for postoperative casting. This paradigm shift has allowed for earlier rehabilitation, decreased rates of nonunion, and significantly improved patient-reported functional outcomes.
The epidemiology of conditions necessitating total wrist arthrodesis is broad, encompassing both inflammatory arthropathies and post-traumatic degenerative cascades. Rheumatoid arthritis was once the leading indication for total wrist arthrodesis; however, the advent of disease-modifying antirheumatic drugs (DMARDs) and biologic therapies has significantly reduced the incidence of end-stage rheumatoid wrist destruction. Today, the most common indications stem from post-traumatic osteoarthritis, specifically Scapholunate Advanced Collapse (SLAC) and Scaphoid Nonunion Advanced Collapse (SNAC). These conditions represent the predictable, progressive articular deterioration that occurs following untreated or failed management of specific carpal ligamentous injuries and fractures.
Recognizing the precursor to these end-stage conditions—most notably rotary subluxation of the scaphoid driven by scapholunate dissociation—is paramount for the orthopedic surgeon. Scapholunate dissociation is the most common and clinically significant form of carpal instability. It typically results from a high-energy fall on an extended, ulnarly deviated, and intercarpal-supinated wrist. Unfortunately, the severity of this initial trauma is frequently underestimated in acute settings, leading to a misdiagnosis of a benign wrist sprain. When the critical stabilizing ligaments are disrupted and left untreated, the altered carpal kinematics initiate a vicious cycle of abnormal shear forces across the radiocarpal and midcarpal joints, inevitably culminating in the SLAC wrist pattern.
The primary goal of total wrist arthrodesis in the setting of these end-stage pathologies is to provide a highly stable, completely painless wrist joint while maximizing the residual functional capacity of the hand and digits. By fusing the radius to the carpus and the third metacarpal, the surgeon eliminates the painful micro-motion of arthritic joints. While all radiocarpal and midcarpal motion is sacrificed, preserving forearm pronosupination and maximizing digital dexterity allows patients to return to a surprisingly high level of function, including heavy manual labor and demanding physical activities.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of carpal osteology, ligamentous anatomy, and wrist kinematics is essential for executing a successful total wrist arthrodesis and for understanding the pathogenesis of rotary scaphoid subluxation. The carpus is a highly complex, intercalated osseous segment situated between the distal radius and the metacarpal bases, lacking any direct tendinous insertions to guide its motion. Instead, carpal kinematics are entirely dependent on articular geometry and a dense, intricate network of intrinsic and extrinsic ligaments.
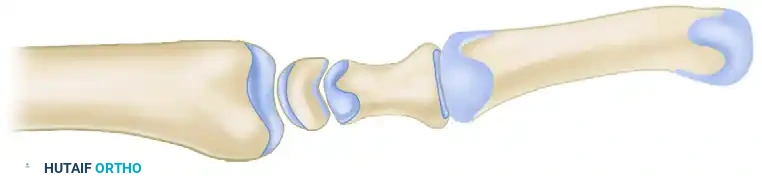
The scaphoid serves as the critical mechanical bridge linking the proximal and distal carpal rows. Its stability relies heavily on the scapholunate interosseous ligament (SLIL), particularly its thick, robust dorsal subregion, which is the primary stabilizer of the scapholunate articulation. Secondary volar stabilizers include the long radiolunate ligament and the radioscaphocapitate (RSC) ligament. Under normal physiological loading, the scaphoid has an inherent biomechanical tendency to flex volarly, while the triquetrum has a strong tendency to extend dorsally. The lunate, centrally located and mechanically coupled to both, is balanced by these opposing forces, maintaining a neutral posture.
Upon complete rupture of the SLIL and its secondary stabilizers, this delicate synchronous motion is catastrophically uncoupled. The scaphoid, freed from the lunate, rotates dorsally at its proximal pole and assumes a fixed, vertically flexed orientation. The lunate, now uncoupled from the scaphoid but still tethered to the triquetrum via the intact lunotriquetral ligament, follows the triquetrum's mechanical pull and extends dorsally. This divergent collapse pattern is clinically recognized as Dorsal Intercalated Segment Instability (DISI). Over time, the flexed scaphoid creates abnormal, concentrated shear forces against the radial styloid, initiating the predictable progression of SLAC arthritis: first involving the radial styloid, progressing to the entire radioscaphoid fossa, and finally encompassing the capitolunate joint.
Biomechanically, the success of a total wrist arthrodesis hinges on meticulous preoperative planning regarding the final position of fusion. The universally accepted functional position of the wrist is 10 to 15 degrees of extension with slight ulnar deviation. This specific spatial orientation is not arbitrary; it maximizes the mechanical advantage of the extrinsic finger flexors through the tenodesis effect, thereby optimizing grip strength. Excessive wrist extension, defined as greater than 20 degrees, must be strictly avoided. Hyper-extension alters the vector of the extensor tendons, leading to chronic extensor tendon irritation against the hardware, fatigue of the intrinsic hand musculature, and significant difficulty with activities of daily living, particularly perineal care and workspace ergonomics.
Exhaustive Indications and Contraindications
The decision to proceed with total wrist arthrodesis must be carefully weighed against motion-preserving alternatives, such as proximal row carpectomy (PRC) or limited intercarpal fusions (e.g., four-corner fusion). Total wrist arthrodesis is generally reserved for patients with advanced, pan-carpal disease where motion-preserving procedures are either contraindicated or have previously failed.
Indications for total wrist arthrodesis include SLAC or SNAC arthritis that has progressed to Stage III (involving the capitolunate joint) or Stage IV (pancarpal involvement). In these advanced stages, the capitate migrates proximally into the scapholunate interval, rendering limited intercarpal fusions mechanically unviable. Rheumatoid arthritis with severe carpal collapse, ulnar translocation of the carpus, and extensive radiocarpal destruction is another classic indication. Additionally, patients with severe spasticity or paralytic deformities, such as those resulting from cerebral palsy, severe stroke, or traumatic brachial plexus injuries, benefit immensely from the stable platform that a total wrist fusion provides.
Contraindications must be rigorously respected to prevent catastrophic surgical failures. Absolute contraindications include the presence of an active local or systemic infection, which precludes the implantation of extensive orthopedic hardware and bone grafting. Open physes in the pediatric population represent another absolute contraindication, as a spanning plate will arrest longitudinal growth of the distal radius and metacarpal. Relative contraindications require nuanced clinical judgment. Severe osteopenia, often seen in advanced rheumatoid arthritis or prolonged disuse, may compromise screw purchase and necessitate augmented fixation techniques or prolonged postoperative immobilization. Furthermore, an unaddressed, severely arthritic distal radioulnar joint (DRUJ) is a relative contraindication; fusing the radiocarpal joint may exacerbate DRUJ symptoms by funneling torque forces directly into the forearm axis. In such cases, concurrent DRUJ procedures, such as a Darrach resection or Sauvé-Kapandji procedure, must be performed.
| Category | Specific Condition/Factor | Clinical Rationale & Surgical Considerations |
|---|---|---|
| Absolute Indications | SLAC/SNAC Stage III & IV | Severe capitolunate arthritis precludes motion-preserving salvage (e.g., 4-corner fusion). |
| Absolute Indications | Failed Partial Wrist Fusion | Nonunion or progressive adjacent-segment arthritis following previous limited carpal arthrodesis. |
| Absolute Indications | Severe Paralytic Deformity | Provides a stable terminal platform for upper extremity function in brachial plexus palsy or spastic hemiplegia. |
| Relative Indications | High-Demand Manual Laborer | Superior durability and grip strength compared to total wrist arthroplasty, which is prone to loosening under heavy loads. |
| Absolute Contraindications | Active Deep Infection | High risk of hardware colonization, osteomyelitis, and systemic sepsis. Requires eradication prior to fusion. |
| Absolute Contraindications | Open Skeletal Physes | Spanning rigid fixation across the distal radial physis will cause premature physeal closure and severe deformity. |
| Relative Contraindications | Severe Osteopenia | Poor bone stock compromises screw purchase. May require locking plates, structural allograft, or prolonged casting. |
| Relative Contraindications | Symptomatic DRUJ Arthritis | TWA increases rotational torque on the DRUJ. Must be addressed concurrently (e.g., Darrach, Sauvé-Kapandji). |
Pre-Operative Planning, Templating, and Patient Positioning
Successful execution of a total wrist arthrodesis requires meticulous preoperative planning, beginning with a comprehensive clinical and radiographic evaluation. The clinical examination must assess baseline digital range of motion, grip strength, and the functional status of the extrinsic tendons. Particular attention must be paid to the distal radioulnar joint (DRUJ). The surgeon must evaluate for DRUJ instability, pain with pronosupination, and focal tenderness over the ulnar head, as unaddressed DRUJ pathology is a primary cause of persistent postoperative pain following wrist fusion.
When evaluating a patient for early-stage carpal instability—the precursor to SLAC—provocative maneuvers are essential. The Watson Scaphoid Shift Test is the most sensitive clinical tool. By applying volar pressure to the scaphoid tuberosity while moving the wrist from ulnar to radial deviation, the examiner prevents normal scaphoid flexion. In an unstable wrist, the proximal pole of the scaphoid subluxates dorsally over the radial rim, eliciting a painful "clunk." Similarly, the "Catch-Up Clunk" test identifies the sudden, uncoupled snapping of the lunate as it aligns with the scaphoid during dynamic loading.
Radiographic evaluation must include high-quality posteroanterior (PA), lateral, and clenched-fist views. On the PA view, a scapholunate gap greater than 2 mm (the "Terry Thomas Sign") is highly suspicious for dissociation, while a gap greater than 3 mm is pathognomonic. The clenched-fist view dynamically loads the carpus, driving the capitate proximally and unmasking occult instability. The lateral radiograph is definitive for diagnosing DISI deformity; a scapholunate angle greater than 60 degrees and a capitolunate angle greater than 20 degrees confirm the divergent collapse pattern. Advanced imaging, such as a non-contrast CT scan, is highly recommended to assess three-dimensional bone stock, identify cystic changes within the carpus, and plan for the volume of bone graft required.
Preoperative templating is mandatory to ensure appropriate implant selection. The surgeon must utilize digital or acetate templates to size the pre-contoured 3.5-mm dynamic compression plate (DCP) or specialized wrist fusion plate. The plate must be long enough to ensure that at least six bone cortices (three bi-cortical screws) are securely engaged in the diaphysis of the third metacarpal, and a minimum of six cortices are engaged in the distal radius. Patient positioning involves placing the patient supine on the operating table with the operative arm extended on a radiolucent hand table. A well-padded upper arm tourniquet is applied. The C-arm fluoroscopy unit should be positioned parallel to the longitudinal axis of the table, entering from the distal end or the contralateral side, allowing for unimpeded orthogonal imaging throughout the procedure.
Step-by-Step Surgical Approach and Fixation Technique
The surgical technique detailed herein follows the highly successful principles popularized by Weiss and Hastings, utilizing a rigid, pre-contoured dorsal spanning plate augmented with local autogenous bone graft. This approach maximizes biomechanical stability while minimizing donor site morbidity.
1. Incision and Dorsal Exposure
The procedure begins with a 10- to 15-cm dorsal longitudinal incision, perfectly centered over the radiocarpal joint. The incision extends from the distal metaphyseal-diaphyseal junction of the radius to the mid-shaft of the long finger (third) metacarpal. Superficial dissection is carried out sharply through the subcutaneous tissues. It is absolutely critical to identify, mobilize, and protect the dorsal sensory branches of the radial nerve on the radial aspect, and the dorsal branch of the ulnar nerve on the ulnar aspect. Neuroma formation in these sensory branches is a devastating complication that can eclipse the benefits of a successful fusion.
The extensor retinaculum is exposed and incised longitudinally. The standard approach utilizes the interval between the third and fourth extensor compartments. The third compartment is opened, and the extensor pollicis longus (EPL) tendon is transposed radially and protected with a vessel loop. The second and fourth extensor compartments are then elevated subperiosteally. This deep exposure provides a panoramic view of the dorsal aspect of the distal radius, the entire carpus, and the third metacarpal. During this deep dissection, the posterior interosseous nerve (PIN) is identified at the floor of the fourth compartment and routinely resected to provide partial wrist denervation and reduce postoperative pain.
2. Joint Preparation and Decortication
Meticulous joint preparation is the biological cornerstone of a successful arthrodesis. Using a sharp osteotome, Lister's tubercle is excised from the distal radius. This maneuver serves a dual purpose: it creates a perfectly flat dorsal surface for optimal plate seating, and it provides a valuable source of highly osteogenic local cancellous bone graft.
The surgeon then proceeds with the systematic decortication of the target joints. Using a combination of rongeurs, sharp curettes, and a high-speed burr under continuous saline irrigation, the dorsal one-fourth of the scaphoid, lunate, capitate, and the third carpometacarpal (CMC) joint are decorticated down to bleeding subchondral bone.
A critical surgical warning must be heeded during this phase: do not arbitrarily include the ulnar midcarpal joints (triquetrohamate) or the second (index) carpometacarpal joint in the fusion mass unless they exhibit frank, advanced arthritic changes on preoperative imaging or direct intraoperative inspection. Preserving the subtle micro-motion at the index CMC joint and the ulnar column significantly improves postoperative hand function, allowing for better grip accommodation around cylindrical objects.
3. Bone Graft Harvesting and Preparation
While iliac crest bone graft (ICBG) was historically considered the gold standard, the morbidity associated with its harvest is significant. Modern techniques favor local autograft. Utilizing a large (6-mm cup) curet, the surgeon harvests copious amounts of cancellous bone from the distal radial metaphysis. The optimal cortical window for harvest is located slightly radial to the base of the excised Lister's tubercle. This local graft is highly cellular and osteogenic. The harvested cancellous bone is densely packed into the decorticated radiocarpal, intercarpal, and third CMC joint spaces before plate application.
4. Plate Selection and Systematic Fixation
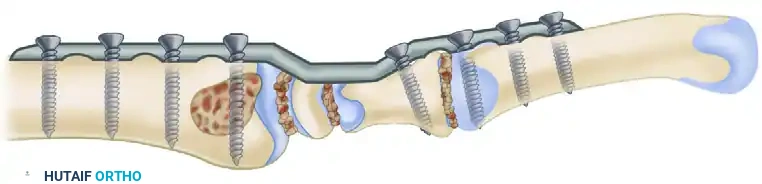
The selection of the implant is paramount. A pre-contoured 3.5-mm dynamic compression plate (DCP) designed specifically for wrist arthrodesis is chosen. Modern plates feature a built-in 10 to 15-degree dorsal bend to recreate the optimal functional extension of the wrist. The plate must span from the radial diaphysis to the third metacarpal diaphysis.

The fixation sequence is meticulously orchestrated to achieve maximum compression across the fusion interfaces:
1. Distal Anchoring: The plate is positioned dorsally. The distal screws are placed into the third metacarpal first, ensuring bi-cortical purchase. This establishes a rigid distal anchor.
2. Graft Interposition: Before the proximal screws are tightened, the surgeon ensures that the harvested cancellous bone graft is tightly packed into the denuded joint spaces, leaving no dead space.
3. Proximal Compression: The plate is fixed to the distal radius. By utilizing the dynamic compression holes in the proximal segment of the plate, the surgeon can actively compress the carpus proximally against the distal radius, loading the fusion site.
4. Carpal Neutralization: To prevent intercalated segment toggle and neutralize rotational forces, one or two cancellous lag screws are placed through the midportion of the plate directly into the carpal bones, most critically the capitate.
During plate positioning, the surgeon must remain hyper-vigilant regarding the distal radioulnar joint (DRUJ). Unless the DRUJ is overtly symptomatic and scheduled for concurrent resection, the plate and screws must not impinge upon it. Screws placed too far ulnarly in the radius can penetrate the sigmoid notch, catastrophically blocking forearm pronosupination.
5. Radiographic Confirmation and Layered Closure
Prior to closure, orthogonal intraoperative fluoroscopy (AP and Lateral views) is mandatory. The surgeon must meticulously verify hardware placement, ensure that no screws violate the CMC joints of adjacent digits, confirm adequate joint compression, and verify that the plate holds the wrist in the optimal 10 to 15 degrees of extension.


Once radiographic confirmation is achieved, the tourniquet is deflated, and meticulous hemostasis is obtained using electrocautery. A closed suction drain may be placed deep to the extensor retinaculum if significant dead space or oozing is present. The dorsal capsule is closed over the plate using interrupted absorbable sutures to provide a critical soft-tissue interposition layer, shielding the extensor tendons from the metallic hardware. The extensor retinaculum is then repaired, leaving the EPL tendon transposed subcutaneously to prevent attrition rupture against the plate. The skin is closed in a standard fashion, and a bulky, sterile compressive dressing supported by a rigid volar short-arm splint is applied.
Complications, Incidence Rates, and Salvage Management
Despite the high success rates associated with modern rigid plating techniques, total wrist arthrodesis is a major reconstructive procedure with a distinct complication profile. The surgeon must be acutely aware of these potential pitfalls, their incidence rates, and the appropriate salvage management strategies. Thorough preoperative patient counseling regarding these risks is a mandatory component of the informed consent process.
The most feared biological complication is nonunion (pseudarthrosis). With modern rigid dorsal plating and meticulous decortication, the nonunion rate has been driven down to approximately 2% to 5%. When nonunion does occur, it most frequently localizes to the third carpometacarpal (CMC) joint. This is biomechanically intuitive, as the third CMC joint represents the distal-most interface and is subject to significant cantilever bending forces during digital flexion. Management of a symptomatic nonunion requires revision surgery, which entails hardware removal, aggressive debridement of the pseudarthrosis, placement of structural iliac crest bone graft, and revision rigid internal fixation, often utilizing a longer plate or orthogonal locking constructs.
Hardware prominence and subsequent extensor tendon irritation represent the most common clinical complications. The dorsal subcutaneous border of the wrist has minimal soft-tissue padding. Even with meticulous capsular closure, the bulk of a 3.5-mm DCP can cause tenosynovitis, particularly of the extensor digitorum communis (EDC). In severe cases, attrition rupture of the extensor tendons can occur. Consequently, symptomatic hardware requiring removal is reported in 15% to 20% of patients. Hardware removal should strictly be delayed until a minimum of 12 to 18 months postoperatively, and only after computed tomography (CT) confirms solid, continuous trabecular bridging across all fusion interfaces.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Treatment |
|---|---|---|---|
| Nonunion (Pseudarthrosis) | 2% - 5% | Inadequate decortication, smoking, poor graft packing, failure to compress. Most common at 3rd CMC. | Revision ORIF, structural ICBG, electrical bone stimulation. |
| Hardware Prominence / Pain | 15% - 20% | Thin dorsal soft-tissue envelope, prominent screw heads, inadequate capsular closure. | Hardware removal (after CT confirmation of solid fusion at >12 months). |
| Extensor Tendon Rupture | 1% - 3% | Attrition over plate edges or screw heads. Failure to transpose EPL subcutaneously. | Tendon transfer (e.g., EIP to EPL), hardware removal, tenolysis. |
| DRUJ Impingement | 2% - 4% | Radial screws placed too long or too ulnarly, penetrating the sigmoid notch. | Immediate screw exchange if found intra-op. Late presentation requires hardware removal or Darrach procedure. |
| Deep Infection | < 2% | Immunosuppression (RA patients on biologics), prolonged operative time, hematoma. | Urgent I&D, hardware retention if stable, IV antibiotics. Hardware removal if fusion is solid or fixation fails. |
Another critical complication is iatrogenic injury to the distal radioulnar joint (DRUJ). If proximal screws are directed too ulnarly, they can breach the sigmoid notch, leading to mechanical block of pronosupination and rapid destruction of the DRUJ articular cartilage. Intraoperative fluoroscopy is the primary defense against this error. If late DRUJ arthritis develops, whether iatrogenic or due to the altered biomechanics of a fused radiocarpal joint, salvage options include the Darrach procedure (distal ulnar resection) or the Sauvé-Kapandji procedure (DRUJ arthrodesis with proximal ulnar pseudoarthrosis).
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a total wrist arthrodesis is a carefully phased process designed to protect the surgical construct while maximizing the functional recovery of the digits and forearm. Because the rigid dorsal plate acts as an internal load-sharing device, prolonged rigid cast immobilization—which historically led to severe digital stiffness and complex regional pain syndrome (CRPS)—is no longer required.
Phase 1: Immediate Postoperative Period (Days 0 to 14)
Immediately following surgery, the patient is immobilized in a bulky compressive dressing reinforced with a rigid volar short-arm splint. The primary goals during this phase are strict edema control, pain management, and the prevention of tendon adhesions. The patient is instructed to keep the extremity elevated above heart level. Crucially, active and passive range of motion exercises for all digits, as well as the thumb, are initiated on postoperative day one. The patient must achieve full composite digital flexion and extension to ensure the extrinsic flexor and extensor tendons glide smoothly past the dorsal surgical site.
Phase 2: Intermediate Protection Phase (Weeks 2 to 6)
At the 10- to 14-day mark, the patient returns to the clinic for suture removal and wound inspection. The bulky surgical splint is discontinued, and a custom-molded, removable thermoplastic short-arm splint is fabricated by a certified hand therapist. This splint holds the wrist in the fused position but leaves the metacarpophalangeal (MCP) joints entirely free. The patient is instructed to wear the splint continuously, removing it only for hygiene and structured therapy sessions. Therapy focuses on aggressive scar massage to prevent skin tethering, continued digital range of motion, and the initiation of active forearm pronation and supination exercises (provided the DRUJ is intact and stable).
Phase 3: Consolidation and Strengthening (Weeks 6 to 12)
At approximately 6 to 8 weeks postoperatively, new radiographs are obtained to assess for trabecular bridging across the radiocarpal and midcarpal joints. Once early radiographic consolidation is confirmed and the patient is non-tender to palpation over the fusion mass, the weaning process from the thermoplastic splint begins. The patient transitions to using the splint only during heavy lifting or high-risk activities. A progressive strengthening program is initiated, focusing on grip strengthening using putty and hand dynamometers, as well as extrinsic flexor/extensor strengthening.
Return to unrestricted heavy manual labor, contact sports, or activities involving high-impact loading of the upper extremity is typically delayed until 12 to 16 weeks postoperatively, contingent upon definitive radiographic evidence of a solid arthrodesis. Patients must be counseled that while grip strength will significantly improve compared to their preoperative arthritic state, it may take up to a full year to achieve maximal medical improvement and neurological adaptation to the fused wrist.
Summary of Landmark Literature and Clinical Guidelines
The contemporary approach to total wrist arthrodesis is heavily grounded in decades of biomechanical research and clinical outcome studies. The foundational literature that shifted the paradigm from pin fixation to rigid plating was authored by Weiss and Hastings in 1995. Their landmark study demonstrated that the use of a pre-contoured 3.5-mm dynamic compression plate yielded a 96% fusion rate, eliminated the need for postoperative casting, and allowed for rapid return to functional activities. This paper established the dorsal spanning plate as the absolute gold standard for wrist fusion.
Understanding the indications for wrist fusion relies equally on the seminal work of Watson and Ballet (1984), who first described the
