Masterclass in Dorsal Capsulodesis and Limited Wrist Arthrodesis
Key Takeaway
Dorsal capsulodesis is a surgical technique designed to correct rotary subluxation of the scaphoid and dorsal intercalated segmental instability (DISI). By utilizing a proximally based capsular flap or the dorsal intercarpal ligament, the scaphoid is tethered to prevent abnormal palmar flexion. This guide details the Blatt technique, Berger modification, and triscaphe arthrodesis, covering indications, biomechanics, step-by-step surgical approaches, and postoperative rehabilitation protocols for optimal carpal kinematics.
Comprehensive Introduction and Patho-Epidemiology
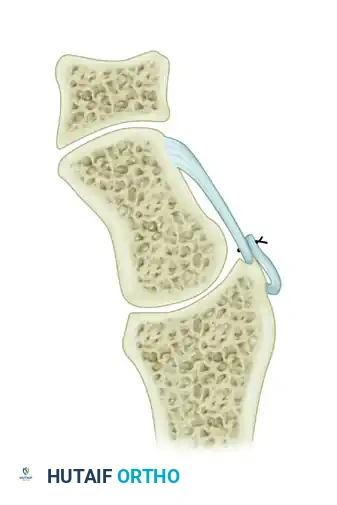
Scapholunate (SL) dissociation represents the most common and clinically significant form of carpal instability encountered by the orthopedic hand and wrist surgeon. The disruption of the scapholunate interosseous ligament (SLIL) complex fundamentally destabilizes the proximal carpal row, precipitating a predictable and unforgiving pattern of kinematic failure. The proximal carpal row acts as an intercalated segment, lacking direct tendinous insertions, and relies entirely on its intricate ligamentous tethers and articular geometry for stability. When the SLIL is compromised, the inherent geometric tendencies of the carpal bones are unleashed. Without the tethering effect of the intact SL ligament, the scaphoid assumes an abnormally palmar-flexed and pronated posture driven by its articulation with the trapezium and trapezoid, while the lunate extends under the uninhibited influence of the triquetrum, resulting in a Dorsal Intercalated Segmental Instability (DISI) deformity.
The epidemiology of scapholunate instability is predominantly linked to acute trauma, most frequently a fall on an outstretched hand (FOOSH) with the wrist positioned in extension, ulnar deviation, and intercarpal supination. This mechanism imparts a tremendous torque across the midcarpal joint, systematically failing the volar radioscaphocapitate ligament, the SLIL, and subsequently the dorsal secondary stabilizers. While acute injuries are often missed in primary care or emergency settings due to the subtle radiographic findings of early dynamic instability, orthopedic surgeons frequently encounter these patients in the subacute or chronic phases. In these delayed presentations, the secondary ligamentous restraints have attenuated, converting a dynamic instability (provocable only under load) into a static, fixed DISI deformity.
If left untreated, the altered contact mechanics between the flexed scaphoid and the elliptical fossa of the radial styloid inevitably progress to Scapholunate Advanced Collapse (SLAC). This degenerative cascade is highly predictable: arthrosis initiates at the radial styloid-scaphoid articulation (Stage I), progresses to involve the entire radioscaphoid fossa (Stage II), and eventually encompasses the capitolunate joint as the capitate migrates proximally into the widened scapholunate interval (Stage III). Notably, the radiolunate joint is typically spared until the very terminal stages of carpal collapse due to the concentric, spherical nature of its articulation. To halt this degenerative cascade before irreversible chondral damage occurs, surgical interventions such as dorsal capsulodesis and limited wrist arthrodesis (triscaphe fusion) have been meticulously developed. These procedures aim to restore the scaphoid to its anatomic alignment, thereby neutralizing aberrant vectors, normalizing carpal kinematics, and preserving joint longevity.
Detailed Surgical Anatomy and Biomechanics
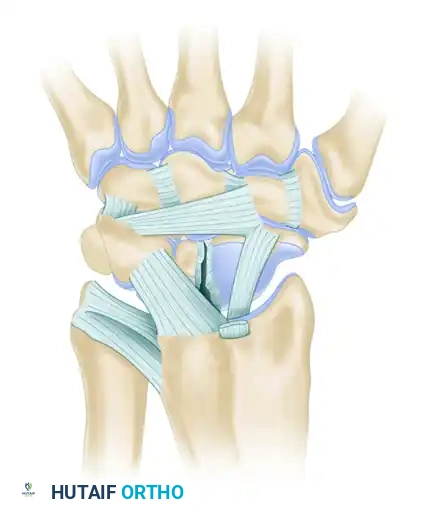
A profound mastery of carpal anatomy and biomechanics is the bedrock upon which successful capsulodesis and limited arthrodesis are built. The scapholunate interosseous ligament (SLIL) is a C-shaped structure divided into three distinct anatomical and biomechanical regions: the dorsal, proximal (membranous), and volar components. The dorsal subregion is the thickest, strongest, and most critical for resisting translation and rotational subluxation. Composed of stout, transversely oriented collagen fibers, it acts as the primary restraint against scaphoid flexion and lunate extension. The volar subregion is thinner but provides essential resistance to rotational forces, while the proximal membranous portion is largely avascular and biomechanically insignificant, serving primarily as a synovial barrier between the radiocarpal and midcarpal joints.
Beyond the primary SLIL, the secondary stabilizers of the scapholunate interval dictate the progression from dynamic to static instability. The dorsal intercarpal (DIC) ligament and the dorsal radiocarpal (DRC) ligament form a critical dorsal V-shaped stabilizing complex. The DIC originates on the triquetrum, courses radially across the lunate (often with a variable attachment), and inserts broadly onto the dorsal ridge of the scaphoid and the trapezium. The DRC originates from the dorsal rim of the distal radius and inserts onto the lunate and triquetrum. Together, these extrinsic ligaments function as a robust secondary restraint. When the SLIL ruptures, the DIC and DRC can temporarily maintain carpal alignment; however, chronic cyclical loading eventually attenuates these structures, leading to the classic static DISI deformity and rotary subluxation of the scaphoid.
Biomechanically, the normal wrist functions through complex, coupled motions, most notably the "dart-thrower's motion" arc, which moves from radial extension to ulnar flexion. During physiologic wrist motion, the scaphoid must flex to clear the radial styloid during radial deviation and extend during ulnar deviation. When the SLIL is torn, the scaphoid's uncoupled flexion drastically reduces the contact area within the radioscaphoid fossa, concentrating massive peak loads on the dorsal rim of the scaphoid and the radial styloid. The primary objective of dorsal capsulodesis is not to reconstruct the anatomic scapholunate ligament—which is often biologically impossible in the chronic setting—but rather to create a robust dorsal tether that prevents the scaphoid from rotating into abnormal palmar flexion. This effectively neutralizes the deforming forces that drive DISI progression, restoring a more physiologic load distribution across the radiocarpal articulation.
Exhaustive Indications and Contraindications
The decision to proceed with a soft-tissue capsulodesis versus a limited wrist arthrodesis hinges upon a meticulous evaluation of the chronicity of the injury, the reducibility of the carpus, and the presence of any chondral degradation. Patient selection is paramount; applying a soft-tissue tether to a fixed, arthritic deformity is a guaranteed mechanism for catastrophic surgical failure. Standard posteroanterior (PA), lateral, and dynamic (clenched fist, ulnar deviation) views must be scrutinized to determine the extent of SL dissociation, the SL angle, and the rotary subluxation of the scaphoid (the "cortical ring sign").
The Blatt dorsal capsulodesis and its Berger modification (DIC capsulodesis) are primarily indicated for subacute to chronic dynamic or reducible static scapholunate instability where direct primary repair of the SLIL is no longer viable due to tissue retraction or poor tissue quality. The absolute prerequisite for any capsulodesis is a completely reducible scaphoid and lunate, alongside pristine articular cartilage in the radiocarpal and midcarpal joints. Conversely, limited wrist arthrodesis—specifically the Scapho-Trapezio-Trapezoid (STT) or triscaphe fusion—is indicated when soft-tissue capsulodesis is insufficient due to chronicity, fixed deformity, or early degenerative changes isolated to the STT joint. By fusing the scaphoid to the distal carpal row, the scaphoid is permanently locked in a perpendicular position relative to the forearm, preventing palmar flexion and stabilizing the entire proximal row.
💡 Clinical Pearl: The Biomechanical Goal
The primary objective of dorsal capsulodesis is not to reconstruct the anatomic scapholunate ligament, but rather to create a robust dorsal tether that prevents the scaphoid from rotating into abnormal palmar flexion. This effectively neutralizes the deforming forces that drive DISI progression.
Indications and Contraindications Matrix
| Procedure Category | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Blatt / Berger Capsulodesis | Chronic, reducible SL instability; Failed primary SL repair; Pre-dynamic or dynamic SL dissociation. | Fixed/irreducible scaphoid flexion; Radioscaphoid or midcarpal arthrosis (SLAC); Incompetent secondary dorsal stabilizers. | Heavy manual laborers; Generalized ligamentous laxity; Patient non-compliance with rehab. |
| Triscaphe (STT) Arthrodesis | Isolated STT osteoarthritis; Chronic, irreducible SL dissociation (without radioscaphoid arthritis); Complex radial column instability. | Radioscaphoid arthritis (early-phase SLAC); Pre-existing capitolunate arthrosis; Thumb CMC joint severe arthrosis. | Rheumatoid arthritis (due to pan-carpal involvement); Severe osteopenia compromising hardware fixation. |
⚠️ Surgical Warning: The Blatt Criterion
Blatt established a strict, singular criterion for this procedure: The surgeon must be able to anatomically reduce the scaphoid at the time of surgery. If the scaphoid is fixed in a flexed position due to secondary capsular contractures or early arthritic changes, a soft-tissue capsulodesis will fail, and a salvage procedure (e.g., proximal row carpectomy or limited arthrodesis) is indicated.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning requires a comprehensive imaging battery. Standard radiographs must include a zero-rotation PA view, a true lateral view, and dynamic stress views. On the PA view, the surgeon must evaluate the scapholunate interval; a gap greater than 3 mm (the "Terry Thomas" sign) is highly suggestive of complete disruption. The lateral view is critical for assessing the SL angle (normal 30-60 degrees; >70 degrees indicates DISI) and the radiolunate angle (>15 degrees of extension indicates DISI). Advanced imaging, such as a high-resolution MRI or MR arthrogram, is frequently utilized to assess the integrity of the SLIL, the extrinsic ligaments, and the vascularity of the proximal pole of the scaphoid. However, diagnostic wrist arthroscopy remains the gold standard for evaluating both the competence of the ligaments and the status of the articular cartilage, often serving as the definitive step in surgical decision-making immediately prior to the open procedure.
Templating for limited wrist arthrodesis requires precise measurement of the scaphoid dimensions and the intended angles of reduction. The surgeon must calculate the trajectory for Kirschner wires or headless compression screws to ensure maximal bone purchase across the STT joint without violating the radioscaphoid or capitolunate articulations. Fusing the scaphoid in a flexed position will lead to catastrophic radiocarpal impingement; therefore, the template must account for reducing the scaphoid into an extended, anatomic posture (an SL angle approaching 45 degrees) prior to definitive fixation.
Patient positioning is standardized but requires meticulous attention to detail to facilitate intraoperative fluoroscopy and unimpeded surgical access. The patient is positioned supine with the operative extremity extended on a radiolucent hand table. Satisfactory regional anesthesia (e.g., supraclavicular or axillary block) or general anesthesia is administered. A well-padded upper arm tourniquet is applied and typically inflated to 250 mm Hg after exsanguination with an Esmarch bandage. The fluoroscopy unit (C-arm) should be positioned parallel to the arm board, entering from the distal or contralateral side to allow the surgeon unimpeded access to the dorsal wrist while permitting seamless orthogonal imaging throughout the procedure.
Step-by-Step Surgical Approach and Fixation Technique
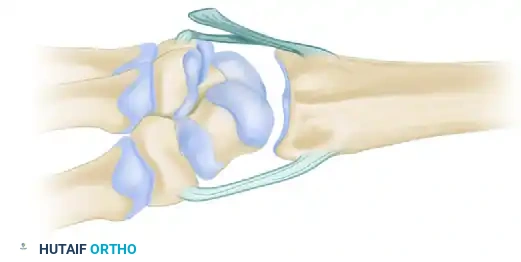
Dorsal Capsulodesis: The Blatt Procedure
Originally described by Blatt, dorsal capsulodesis utilizes a proximally based flap of the dorsal wrist capsule to tether the distal pole of the scaphoid to the dorsal rim of the distal radius.
1. Patient Positioning and Approach
Ensure satisfactory regional or general anesthesia, prepare and drape the upper extremity in a standard sterile fashion, and inflate the tourniquet. Make a longitudinal dorsoradial incision centered over Lister's tubercle, extending distally toward the base of the third metacarpal. This incision allows extensile access to the radiocarpal and midcarpal joints.
2. Exposure and Retraction
Identify and meticulously protect the sensory branches of the superficial radial nerve, which are highly susceptible to traction neurapraxia. Open the third dorsal extensor compartment and transpose the extensor pollicis longus (EPL) tendon radially. Elevate the fourth dorsal compartment subperiosteally, retracting the wrist extensors laterally and the finger extensors medially to expose the dorsal capsule.
3. Capsular Flap Creation
Make a longitudinal incision through the dorsal capsule near the longitudinal axis of the scaphoid to expose its full length. Preserve a robust 1-cm wide flap of the dorsal wrist capsule, developing this flap from the ulnar side of the capsular incision. Release the flap distally, leaving its proximal origin firmly attached to the stout periosteum and ligaments of the dorsum of the distal radius.
4. Joint Inspection and Scaphoid Reduction
Inspect the interosseous and dorsal scapholunate ligaments to confirm their rupture and assess irreparability. Evaluate the articular surfaces to ensure no early SLAC changes are present. Reduce the scaphoid by applying firm thumb pressure on the scaphoid tubercle from the palmar aspect while simultaneously bringing the wrist into slight ulnar deviation and extension to correct the scaphoid's flexed posture.
5. Kirschner Wire Fixation
Once anatomic reduction is achieved and confirmed via fluoroscopy, transfix the scaphoid using 0.045-inch (1.16-mm) Kirschner wires. Drive the wires from the distal pole of the scaphoid into the capitate and the base of the third metacarpal to hold the reduction rigidly. A supplementary wire from the scaphoid to the lunate may also be utilized to maintain the SL interval.
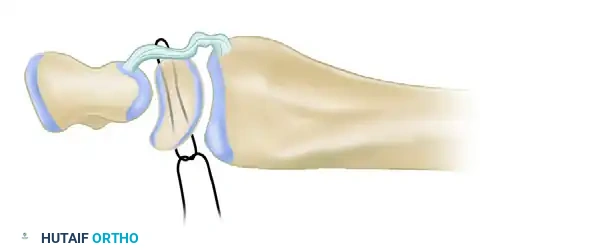
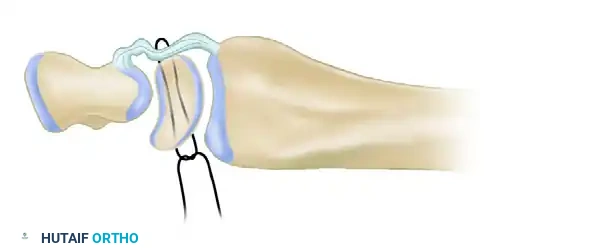
6. Scaphoid Preparation and Flap Insertion
Using a narrow osteotome or a small rongeur, create a transverse notch in the dorsal cortex of the distal pole of the scaphoid. This notch must be proximal to the distal articular surface and distal to the midaxis of rotation of the scaphoid to maximize the mechanical advantage of the tenodesis.
Trim the proximally based dorsal capsuloligamentous flap to the appropriate length, ensuring it is under physiological tension when the wrist is in neutral. Secure the flap into the prepared scaphoid notch using a 4-0 stainless steel pull-out wire suture or, in modern iterations, a bone anchor. If using a pull-out wire, pass the suture through fine drill holes directed toward the volar tubercle of the scaphoid.
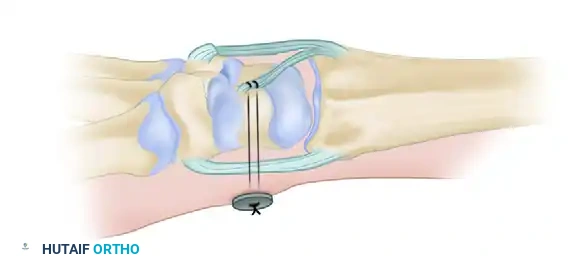
Tie the pull-out wire at the level of the palmar skin over a felt pad and a button to secure the tenodesis effect. Deflate the tourniquet, obtain meticulous hemostasis, and close the skin in layers.
The Berger Modification: Dorsal Intercarpal (DIC) Ligament Capsulodesis
Recognizing the biomechanical limitations of a non-specific capsular flap, Berger described a highly effective modification utilizing the Dorsal Intercarpal (DIC) ligament. This technique leverages the native, robust collagenous architecture of the DIC to provide a stronger, more anatomically aligned vector of pull.
Surgical Technique (Berger Modification)
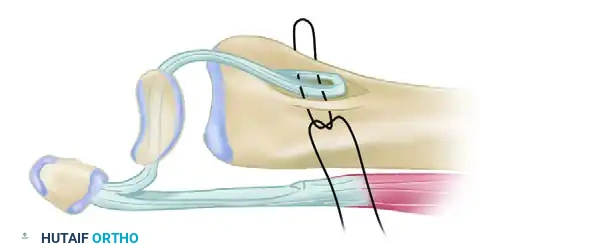
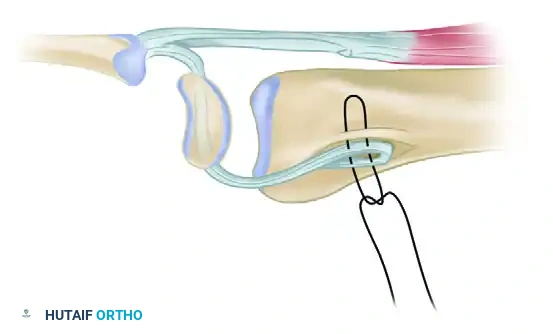
Instead of raising a standard capsular flap, the surgeon identifies the robust dorsal intercarpal ligament coursing transversely across the proximal carpal row. Incise down the length of the DIC ligament to detach its proximal half, carefully preserving the lateral insertion of the ligament firmly attached to the distal scaphoid. Detach the medial (triquetral) end of the ligament, creating a robust, scaphoid-based ligamentous sling.
Reduce the scaphoid into an extended, anatomic position and secure it with K-wires as previously described. Suture the free, triquetral end of the DIC ligament to the dorsal rim of the distal radius. This attachment can be made directly to bone using suture anchors or sutured to the stout origin of the dorsal radiocarpal ligament.
💡 Biomechanical Advantage of the Berger Technique
By utilizing the DIC ligament, the Berger modification provides a stronger, more anatomically aligned vector of pull to resist scaphoid flexion compared to the traditional Blatt capsular flap. It directly counteracts the rotary subluxation forces while minimizing the loss of physiologic wrist flexion.
Limited Wrist Arthrodesis: Triscaphe (STT) Fusion
When soft-tissue capsulodesis is insufficient, limited wrist arthrodesis becomes the procedure of choice. The surgical execution of an STT fusion requires meticulous joint preparation. Through a dorsal approach, the capsule is elevated to expose the scaphotrapezial and scaphotrapezoidal joints. The articular surfaces are meticulously decorticated using a high-speed burr or fine osteotomes down to bleeding subchondral bone. It is imperative to preserve the overall geometry of the bones to prevent carpal collapse during compression.
The scaphoid is anatomically reduced out of its flexed posture. Kleinman noted that in a review of 41 cases, the development of postoperative arthrosis was directly related to imperfect reduction of the scaphoid prior to fusion. Fusing the scaphoid in a flexed position will lead to catastrophic radiocarpal impingement. Once extended, the STT joint is packed tightly with cancellous bone graft, typically harvested from the distal radius (Lister's tubercle) or iliac crest.
Fixation is achieved using multiple divergent 0.045-inch or 0.062-inch K-wires, or modern headless compression screws. If using screws, precise guidewire placement is critical to ensure the threads fully cross the arthrodesis site without violating the radioscaphoid or trapeziometacarpal joints. The construct is evaluated under live fluoroscopy through a full range of motion to confirm stability and the absence of hardware impingement.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, both dorsal capsulodesis and limited wrist arthrodesis carry a significant complication profile. The most ubiquitous complication following any dorsal capsulodesis is a predictable loss of terminal wrist flexion. Patients typically lose 20 to 30 degrees of palmar flexion due to the intentional dorsal tethering of the scaphoid. While this is mechanically necessary to prevent DISI recurrence, it must be explicitly discussed with the patient preoperatively. Recurrent instability or stretching of the capsulodesis flap occurs in up to 15-20% of cases, particularly in non-compliant patients or those with unrecognized fixed deformities.
For STT arthrodesis, nonunion is a formidable complication, historically reported at rates between 5% and 15%. The complex, multi-planar geometry of the STT joint makes rigid compression challenging. Furthermore, hardware complications, such as K-wire migration, pin-tract infections, or symptomatic screw heads, frequently necessitate secondary hardware removal procedures. The most devastating complication of STT fusion is the accelerated progression of radioscaphoid arthrosis, almost exclusively resulting from fusing the scaphoid in a non-anatomic, palmar-flexed position, which creates a severe dorsal impingement against the radial styloid.
Complications and Salvage Protocol Table
| Complication | Incidence Rate | Etiology / Risk Factors | Salvage Management / Intervention |
|---|---|---|---|
| Loss of Wrist Flexion | 80-100% (Expected) | Intentional dorsal tethering; capsular scarring. | Aggressive postoperative therapy after 8 weeks; rarely requires surgical release. |
| Recurrent SL Instability | 10-20% | Flap attenuation; unrecognized fixed deformity; premature K-wire removal. | Conversion to limited arthrodesis (STT or SC fusion) or Proximal Row Carpectomy (PRC). |
| STT Nonunion | 5-15% | Inadequate decortication; poor bone grafting; thermal necrosis from burr; smoking. | Revision arthrodesis with structural iliac crest bone graft and rigid screw fixation. |
| Radioscaphoid Arthrosis | 10-25% (Long-term) | Malreduction (scaphoid fused in flexion); pre-existing occult chondral damage. | Proximal Row Carpectomy (PRC) or Scaphoid Excision + 4-Corner Fusion. |
| Hardware Failure / Migration | 5-10% | Poor screw trajectory; K-wire backing out; cyclical loading before union. | Hardware removal; revision fixation if union is not yet achieved. |
When these procedures fail and the patient develops intractable pain and progressive SLAC wrist, salvage operations must be employed. Proximal Row Carpectomy (PRC) involves the excision of the scaphoid, lunate, and triquetrum, allowing the capitate to articulate directly with the lunate fossa of the radius. Alternatively, a Scaphoid Excision and Four-Corner Fusion (capitate, hamate, lunate, triquetrum) preserves the radiolunate articulation. Both salvage procedures reliably relieve pain while preserving approximately 50% of the native wrist arc of motion.
Phased Post-Operative Rehabilitation Protocols
Strict adherence to postoperative protocols is critical to prevent stretching of the capsulodesis or disruption of the arthrodesis before robust biologic healing occurs. The rehabilitation timeline is phased to balance the protection of the surgical construct with the prevention of debilitating stiffness.
Phase I: Maximum Protection (0 to 14 Days)
Immediately postoperatively, the patient is immobilized in a bulky, rigid thumb spica splint or cast. Elevation and strict digital range-of-motion exercises are instituted immediately to prevent tendon adhesions and reduce edema. At 10 to 14 days, the initial dressing is removed, the surgical incision is inspected, skin sutures are extracted, and a new, well-molded, short-arm thumb spica cast is applied.
Phase II: Continued Immobilization and Early Healing (2 to 8 Weeks)
The secondary cast remains in place for an additional 6 weeks, totaling 8 weeks of continuous rigid immobilization for capsulodesis procedures. For STT fusions, this phase may be extended depending on radiographic evidence of consolidation. During this period, patients must continue aggressive active motion of the fingers, elbow, and shoulder.
Phase III: Hardware Removal and Early Motion (8 to 12 Weeks)
At approximately 8 weeks postoperatively, the cast is removed. For the Blatt technique, the pull-out wire and the transfixing K-wires are removed in the clinic under local anesthesia. For STT fusions utilizing K-wires, removal is typically delayed until 10 to 12 weeks when radiographic union is definitively confirmed. Once hardware is removed, gentle, active range-of-motion (ROM) exercises for the wrist are initiated under the guidance of a certified hand therapist. Passive stretching, forceful gripping, and weight-bearing are strictly prohibited.
Phase IV: Strengthening and Return to Function (12+ Weeks)
At 12 weeks, provided clinical and radiographic stability is maintained, progressive strengthening exercises are introduced. Dynamic splinting may be cautiously utilized if severe stiffness persists, though the surgeon must weigh the risk of attenuating the capsulodesis flap. Forceful stress activities, heavy lifting, and impact sports are restricted for approximately 4 to 6 months to ensure complete bony consolidation and structural remodeling of the arthrodesis mass.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical management for scapholunate instability is deeply rooted in several landmark publications that continue to dictate modern clinical guidelines. In 1987, Blatt published his seminal work on dorsal capsulodesis, providing a reliable soft-tissue tether for dynamic instability. His strict criterion—that the scaphoid must be anatomically reducible—remains the absolute rule for this procedure. Long-term follow-up studies of the Blatt procedure have demonstrated reliable pain relief and prevention of SLAC progression in appropriately selected patients, albeit with a universal, permanent decrease in terminal wrist flexion.
Berger’s 1998 description of the Dorsal Intercarpal (DIC) ligament capsulodesis represented a critical biomechanical advancement. By utilizing a native ligamentous structure rather than a non-specific capsular flap, Berger demonstrated improved resistance to scaphoid flexion and a more anatomic axis of restraint. Biomechanical studies have consistently validated that the DIC modification provides superior yield strength and stiffness compared to the traditional Blatt flap, making it the preferred soft-tissue technique for many contemporary hand surgeons.
In the realm of limited wrist arthrodesis, the works of Watson and Hempton in the 1980s popularized the triscaphe (STT) fusion. They demonstrated its profound effectiveness in resisting the massive forces of carpal movement and permanently correcting the DISI deformity. Kleinman’s subsequent extensive reviews refined the indications and highlighted the critical pitfalls of the procedure. Kleinman definitively proved that imperfect reduction of the scaphoid prior to fusion is the primary driver of postoperative radiocarpal arthrosis. Current clinical guidelines derived from these landmark papers dictate that STT fusion is a powerful tool for chronic instability, provided the radiocarpal joint is pristine and the surgeon achieves absolute anatomic extension of the scaphoid prior to definitive fixation.
This academic synthesis is based on established protocols from Hutaifortho's Operative Orthopaedics and ---
