Arthroscopic Management of Ankle Instability, Fractures, and Arthrodesis
Key Takeaway
Arthroscopic management of ankle pathology has evolved significantly, offering minimally invasive solutions for chronic instability, impingement syndromes, osteochondral lesions, and end-stage arthritis. This comprehensive guide details evidence-based surgical techniques, including arthroscopic-assisted lateral ligament repair, syndesmotic evaluation, and arthroscopic ankle arthrodesis. By minimizing soft tissue compromise and addressing concomitant intraarticular pathology, these advanced arthroscopic interventions optimize functional outcomes and accelerate postoperative rehabilitation in complex foot and ankle surgery.
Comprehensive Introduction and Patho-Epidemiology
The evolution of ankle arthroscopy has unequivocally transformed the management of complex foot and ankle pathology. Originally utilized primarily as a diagnostic adjunct in the late 20th century, arthroscopic techniques have advanced at an exponential rate to become the definitive therapeutic modality for a wide spectrum of conditions. This spectrum ranges from chronic lateral ankle instability (CAI) and anterior or posterior impingement syndromes to complex intraarticular fractures, osteochondral lesions of the talus (OLTs), and end-stage tibiotalar arthritis. The transition from open arthrotomy to minimally invasive arthroscopic techniques reflects a broader surgical paradigm shift prioritizing the preservation of the delicate soft tissue envelope of the ankle, minimizing surgical site morbidity, and accelerating functional rehabilitation.
Epidemiologically, acute ankle sprains represent one of the most ubiquitous injuries encountered in both emergency departments and orthopedic clinics, accounting for up to 40% of all sports-related injuries. While the majority of these inversion injuries resolve with functional rehabilitation, up to 20% to 30% of patients will develop chronic ankle instability. This chronic state is characterized by mechanical laxity, persistent pain, and recurrent subjective sensations of "giving way." The pathophysiological cascade initiated by CAI leads to altered joint kinematics, specifically an abnormal anterior translation and internal rotation of the talus within the mortise during the stance phase of gait. This asymmetric loading significantly increases shear forces across the articular cartilage, predisposing the patient to the development of osteochondral lesions and, ultimately, post-traumatic osteoarthritis.
Furthermore, the integration of arthroscopy into the management of acute ankle fractures and syndesmotic injuries has revolutionized our understanding of intraarticular pathology. Traditional fluoroscopic evaluation often fails to detect subtle syndesmotic diastasis or concomitant chondral shear injuries, which are present in up to 70% of rotational ankle fractures. By employing arthroscopy, the orthopedic surgeon can achieve direct, magnified visualization of the articular surface, ensuring anatomic reduction and addressing occult pathology simultaneously. For the practicing orthopedic surgeon, mastering these advanced techniques requires a profound understanding of ankle biomechanics, precise portal anatomy to avoid catastrophic neurovascular injury, and a rigorous adherence to evidence-based indications. This masterclass expands upon the foundational principles of operative orthopedics to provide a comprehensive, step-by-step guide to arthroscopic interventions in the ankle.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of ankle anatomy is the absolute prerequisite for safe and effective arthroscopy. The ankle joint, or talocrural joint, is a highly congruent, modified hinge joint formed by the distal tibia, the medial malleolus, the lateral malleolus of the fibula, and the talus. The osseous architecture provides inherent stability, particularly in dorsiflexion, as the talar dome is trapezoidal—wider anteriorly than posteriorly. Consequently, during dorsiflexion, the wider anterior aspect of the talus engages the mortise, tensioning the syndesmotic ligaments and providing maximum osseous stability. Conversely, in plantarflexion, the narrower posterior talus occupies the mortise, relying heavily on the lateral ligamentous complex for stability.
The lateral collateral ligamentous complex is the primary restraint against inversion and internal rotation. It consists of three distinct structures: the anterior talofibular ligament (ATFL), the calcaneofibular ligament (CFL), and the posterior talofibular ligament (PTFL). The ATFL is an intracapsular, extra-articular structure that originates from the anterior margin of the distal fibula and inserts onto the talar body. It is the weakest of the lateral ligaments and the first to rupture during a plantarflexion-inversion injury. Recent anatomical studies have delineated the ATFL into superior and inferior fascicles; the inferior fascicle shares a continuous footprint with the CFL at the fibula, a critical anatomical nuance when performing an anatomic arthroscopic repair. The syndesmotic complex, comprising the anterior inferior tibiofibular ligament (AITFL), posterior inferior tibiofibular ligament (PITFL), interosseous ligament (IOL), and the transverse ligament, is paramount for maintaining the integrity of the ankle mortise.
Precise portal placement is dictated by the complex arborization of the neurovascular structures crossing the anterior and posterior ankle. The standard anteromedial (AM) portal is established medial to the tibialis anterior tendon, placing the saphenous nerve and the great saphenous vein at risk if the incision is extended too far medially. The anterolateral (AL) portal is established lateral to the peroneus tertius tendon. The absolute critical structure at risk here is the superficial peroneal nerve (SPN), specifically its intermediate dorsal cutaneous branch. The SPN typically bifurcates 5 to 7 cm proximal to the ankle joint and crosses the joint line approximately 4.5 mm from the standard AL portal. Transillumination of the skin using the arthroscope from the AM portal is a mandatory maneuver to visualize and avoid the SPN prior to establishing the AL portal. Posteriorly, the posterolateral and posteromedial portals are established adjacent to the medial and lateral borders of the Achilles tendon, respectively. The posteromedial portal places the posterior tibial artery and tibial nerve at significant risk; thus, instruments must always be directed laterally toward the midline to avoid the neurovascular bundle.
Exhaustive Indications and Contraindications
The decision to proceed with arthroscopic intervention in the ankle must be predicated on a meticulous clinical examination, advanced imaging, and a clear understanding of the patient's functional demands. While arthroscopy is minimally invasive, it is not without risk, and strict adherence to established indications is required to optimize clinical outcomes.
Surgical intervention for chronic ankle instability is indicated when prolonged conservative management—including a minimum of 3 to 6 months of aggressive peroneal strengthening, proprioceptive rehabilitation, and bracing—fails to provide dynamic stability. Arthroscopic management of osteochondral lesions of the talus (OLTs) is indicated for symptomatic, unstable lesions, or those that have failed non-operative management. End-stage tibiotalar arthritis is the classic indication for arthroscopic ankle arthrodesis, particularly in patients with minimal coronal plane deformity (less than 10 to 15 degrees of varus or valgus).
Contraindications must be strictly respected to avoid catastrophic complications. Absolute contraindications include active localized or systemic infection, severe peripheral vascular disease precluding wound healing, and active Charcot neuroarthropathy. Relative contraindications for arthroscopic arthrodesis include severe osseous deformity requiring extensive structural bone grafting or major corrective osteotomies, as the limited visualization of arthroscopy makes complex multi-planar corrections exceedingly difficult.
| Clinical Condition | Primary Indications for Arthroscopy | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Chronic Ankle Instability (CAI) | Failure of >3-6 months conservative therapy; recurrent symptomatic giving way; concomitant intraarticular pathology (OLT, loose bodies). | Active joint infection; severe generalized ligamentous laxity (e.g., Ehlers-Danlos) requiring open augmentation. | Severe rigid hindfoot varus (requires concomitant calcaneal osteotomy); poor soft tissue envelope. |
| Osteochondral Lesions (OLT) | Symptomatic lesions >1cm; failed conservative management; detached or unstable osteochondral fragments. | Active infection; advanced diffuse tibiotalar osteoarthritis (kissing lesions). | Massive cystic lesions requiring bulk structural allograft (better suited for open OATS/medial malleolar osteotomy). |
| Ankle Impingement (Anterior/Posterior) | Painful mechanical block to motion; failed conservative care/injections; symptomatic Os Trigonum in athletes. | Asymptomatic osteophytes discovered incidentally on imaging. | Extensive heterotopic ossification bridging the joint space. |
| End-Stage Ankle Arthritis | Post-traumatic or degenerative OA with intractable pain; minimal to moderate deformity (<15° coronal plane deformity). | Active infection; severe Charcot neuroarthropathy; inadequate vascular supply. | Severe bone loss requiring structural grafting; >15° fixed varus/valgus deformity. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the cornerstone of successful ankle arthroscopy. A comprehensive radiographic series, including weight-bearing anteroposterior (AP), lateral, and mortise views, is mandatory. Stress radiography (anterior drawer and talar tilt) can quantify the degree of mechanical instability, though its routine use has been largely supplanted by advanced imaging. Magnetic Resonance Imaging (MRI) is the gold standard for evaluating the integrity of the lateral ligamentous complex, assessing the syndesmosis, and characterizing osteochondral lesions. For OLTs, T2-weighted fat-suppressed sequences are critical for delineating the extent of subchondral bone marrow edema, while Computed Tomography (CT) is invaluable for precisely mapping the osseous architecture and cystic volume of the lesion, which dictates the choice between microfracture and osteochondral autograft transfer.
Patient positioning must be meticulously planned based on the targeted pathology. For standard anterior ankle arthroscopy, the patient is positioned supine on the operating table with a thigh tourniquet. The distal leg is allowed to hang freely off the end of the table, or a specialized leg holder is utilized to maintain the knee in a flexed position, relaxing the gastrocnemius-soleus complex and facilitating ankle dorsiflexion. Non-invasive distraction using a standardized ankle strap applied over the hindfoot and midfoot is often necessary. The distractor is secured to the operating table, allowing the application of controlled, in-line traction (typically 15 to 30 lbs) to open the highly congruent tibiotalar joint space, preventing iatrogenic scuffing of the tibial plafond during instrument insertion.
When complex pathology dictates that access to both the anterior and posterior aspects of the joint is necessary, intraoperative repositioning (switching the patient from supine to prone) can be highly cumbersome, significantly increasing operative time and compromising the sterile field. Advanced alternative setup strategies have been developed to mitigate this.
* The Supine External Rotation Technique: The surgeon performs the anterior ankle arthroscopy with the patient supine as standard. Once complete, the leg is externally rotated maximally (often requiring a large sandbag under the ipsilateral hip) to place two posteromedial portals. While this avoids repositioning, access to the far lateral aspect of the posterior compartment can be somewhat restricted.
* The Prone Flexion Technique: The patient is positioned prone for standard posterior arthroscopy (utilizing posteromedial and posterolateral portals adjacent to the Achilles tendon). To access the anterior ankle, the knee is flexed to 90 degrees, allowing the surgeon to reach over the top of the foot to establish anterior portals. This requires a highly experienced arthroscopist as the spatial orientation is inverted.
Step-by-Step Surgical Approach and Fixation Technique
Diagnostic Arthroscopy and Portal Placement
The procedure universally begins with a systematic diagnostic arthroscopy. The anteromedial (AM) portal is established first, using a #11 blade to incise only the skin, followed by blunt dissection with a mosquito hemostat to spread the subcutaneous tissues, pushing the saphenous nerve and vein out of harm's way. A 4.0-mm or 2.7-mm 30-degree arthroscope is introduced with a blunt trocar. The joint is insufflated with normal saline. The anterolateral (AL) portal is then established under direct intra-articular visualization. The arthroscope light is used to transilluminate the skin, identifying the arborization of the superficial peroneal nerve. A spinal needle is utilized to localize the optimal trajectory before making the AL incision. A thorough 21-point diagnostic sweep of the anterior, medial, and lateral gutters, the talar dome, and the syndesmosis is mandatory.
Arthroscopic Management of Ankle Instability
Historically, thermal capsular shrinkage was proposed as a minimally invasive adjunct for managing micro-instability and capsular laxity. The theoretical biomechanical advantage relied on the application of radiofrequency energy to denature type I collagen, thereby reducing capsular volume. However, there is sparse evidence in the contemporary orthopedic literature supporting its efficacy. High rates of recurrent laxity, coupled with the risk of iatrogenic thermal injury to the superficial peroneal nerve (SPN) and sural nerve, have led to a Grade C recommendation (poor evidence). This procedure has largely been abandoned in modern practice.
Today, Arthroscopic-Assisted Lateral Ligament Repair (the "Arthroscopic Broström") is the procedure of choice.
1. Accessory Portal Placement: An accessory anterolateral portal is established under direct visualization, typically slightly inferior and anterior to the standard AL portal, ensuring the SPN branches are strictly protected.
2. Preparation of the Fibular Footprint: The lateral gutter is aggressively cleared of hypertrophic synovitis. The fibular footprint of the ATFL is decorticated using a motorized 4.0-mm shaver or burr to expose bleeding subchondral bone, promoting a robust biological healing response.
3. Anchor Placement: One or two suture anchors (typically 2.5 mm to 3.0 mm biocomposite or all-suture anchors) are placed into the distal fibula arthroscopically, approximately 1 cm proximal to the distal tip of the fibula.
4. Suture Passage: Using specialized curved suture-passing devices (e.g., MicroLasso or similar) through the accessory portal, the sutures are passed through the attenuated ATFL and the extensor retinaculum, effectively incorporating the Gould modification to reinforce the subtalar joint.
5. Knot Tying: The sutures are retrieved and tied using a sliding-locking knot configuration with the ankle held in neutral dorsiflexion and slight eversion to appropriately tension the construct.
Osteochondral Lesions of the Talus (OLT)
The highly congruent nature of the tibiotalar joint makes accessing posterior or central dome lesions exceptionally difficult. Noninvasive distraction is critical. The primary surgical goal is the complete excision of unstable cartilage, removal of the necrotic subchondral bone cyst, and penetration of the subchondral plate. Once the lesion is identified, a ring curette is used to remove all loose articular cartilage until stable, vertical margins are achieved (the "containment" principle). The necrotic base is debrided. Microfracture awls or a retrograde drill are then utilized to penetrate the subchondral plate to a depth of 2 to 4 mm, spaced 2 to 3 mm apart. It is critical that subchondral penetration is performed perpendicular to the lesion. If the lesion is located far posteriorly, transmalleolar drilling through the medial or lateral malleolus, or the use of specialized curved guides, may be required to achieve the correct orthogonal trajectory.
Ankle Fractures and Syndesmotic Instability
Arthroscopy is increasingly utilized to assist with the anatomic reduction of complex articular fractures, including pilon fractures and posterior malleolar fractures. For syndesmotic instability, arthroscopy offers diagnostic superiority over standard stress radiographs. The "arthroscopic stress test" involves introducing a 3-mm probe into the tibiofibular articulation; widening greater than 2 mm under direct visualization confirms dynamic instability. For chronic syndesmosis injuries without lateral displacement of the talus, aggressive arthroscopic debridement of the hypertrophic scar tissue in the syndesmotic recess is often sufficient. If chronic widening is present, debridement is followed by the percutaneous placement of syndesmotic screws or dynamic button constructs across the articulation after precise anatomic reduction is achieved using a large reduction clamp.
Arthroscopic Ankle Arthrodesis
End-stage tibiotalar arthritis is definitively managed via ankle arthrodesis. The primary advantage of the arthroscopic approach is the preservation of the periosteal blood supply, minimizing the risk of wound dehiscence—a critical factor in patients with long-standing diabetes mellitus or severe vascular compromise.
Joint Preparation: Following standard portal placement and distraction, an aggressive synovectomy is performed. The remaining articular cartilage is removed using ring curettes and Cobb elevators.
FIGURE 50-11 Ankle arthrodesis. Motorized burr used to remove thin layer of subchondral bone (approximately 2 mm).
As demonstrated in Figure 50-11, a motorized burr is systematically utilized to remove a thin layer of the subchondral bone plate (approximately 2 mm). The surgical objective is to expose healthy, bleeding, punctate cancellous bone while strictly preserving the anatomic contour of the talar dome and the tibial plafond. Maintaining this ball-and-socket architecture provides intrinsic multi-planar stability to the construct, which is vital for primary bone healing.
Positioning the Arthrodesis: The distractor is removed. The ankle is positioned in the optimal alignment for fusion: Neutral dorsiflexion (0 degrees), 0 to 5 degrees of valgus, 5 to 10 degrees of external rotation (matching the contralateral limb), and slight posterior translation of the talus under the tibia to optimize the biomechanical lever arm of the Achilles tendon.
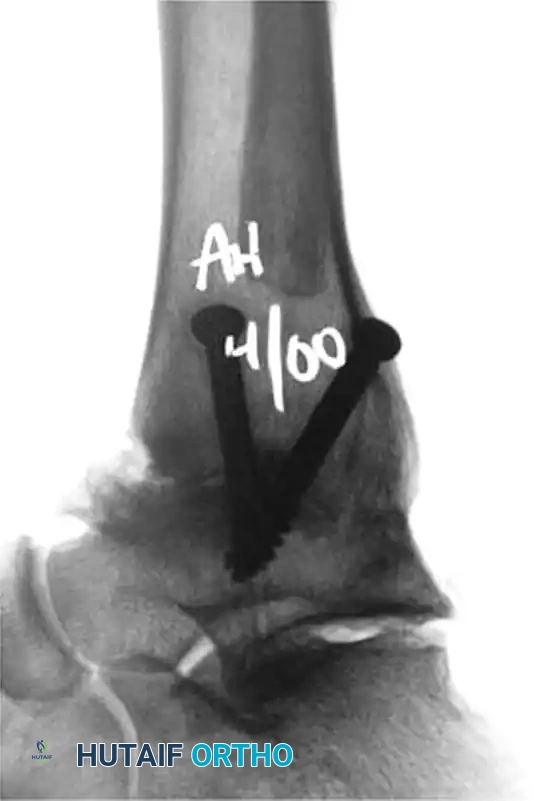
Percutaneous Fixation: Rigid compression is paramount. Fixation is typically achieved using two or three large-diameter (6.5-mm or 7.3-mm) cannulated, partially threaded screws.

FIGURE 50-12 Fixation with two 6.5-mm cannulated screws (Anteroposterior View).
FIGURE 50-13 Fixation with two 6.5-mm cannulated screws (Lateral View).
As seen in the radiographic imaging (Figures 50-12 and 50-13), a standard crossed-screw configuration is employed. Guidewires are placed percutaneously under fluoroscopic guidance.
* The First Screw (Home Run Screw): Typically directed from the posterior aspect of the distal tibia (inserted just lateral to the Achilles tendon), aiming anteriorly and inferiorly into the dense bone of the talar neck. This screw provides the most robust compression.
* The Second Screw: Directed from the medial malleolus, crossing the joint line to engage the lateral aspect of the talar body.
* Optional Third Screw: If rotational stability is questionable, a third screw can be placed from the anterolateral tibia into the central or medial talus.
Complications, Incidence Rates, and Salvage Management
While arthroscopic techniques significantly reduce the morbidity associated with open exposures, they are not immune to complications. Neurological injury remains the most frequently reported complication in ankle arthroscopy, with an overall incidence ranging from 3% to 9%. The superficial peroneal nerve (SPN) is the most commonly injured structure, typically due to improper placement of the anterolateral portal or aggressive use of standard, non-hooded shavers in the lateral gutter. Injury can range from transient neuropraxia due to traction, to complete transection resulting in painful neuroma formation.
Infection rates in ankle arthroscopy are exceedingly low, generally reported at less than 1%. However, the introduction of hardware (suture anchors or large cannulated screws for arthrodesis) slightly elevates this risk. Nonunion or delayed union is the most dreaded complication following arthroscopic ankle arthrodesis, occurring in 5% to 10% of cases, heavily influenced by patient comorbidities such as smoking, diabetes, and non-compliance with weight-bearing restrictions.
Complex Regional Pain Syndrome (CRPS) is a devastating, albeit rare, complication that can occur following any foot and ankle intervention. It is characterized by disproportionate pain, allodynia, sudomotor changes, and trophic skin alterations. Early recognition and aggressive multidisciplinary management, including sympathetic nerve blocks and rigorous physical therapy, are critical to preventing permanent disability.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management & Prevention |
|---|---|---|---|
| Superficial Peroneal Nerve (SPN) Injury | 3% - 9% | Blind placement of AL portal; aggressive shaving in lateral gutter; excessive traction. | Prevention: Transillumination, "nick and spread" technique. Salvage: Gabapentinoids for neuropraxia; surgical excision and burying of neuroma into muscle belly for transection. |
| Nonunion of Arthrodesis | 5% - 10% | Smoking, uncontrolled diabetes, inadequate subchondral bone preparation, failure to achieve rigid compression. | Prevention: Meticulous burring to punctate bleeding bone; rigid multi-planar fixation. Salvage: Revision open arthrodesis with structural bone grafting and robust plating systems (e.g., anterior or lateral locking plates). |
| Recurrent Instability (Post-Broström) | 5% - 8% | Premature return to sport; unrecognized generalized laxity; failure to address severe hindfoot varus. | Prevention: Concomitant calcaneal osteotomy for rigid varus; prolonged immobilization in non-compliant patients. Salvage: Open anatomic reconstruction using allograft (e.g., semitendinosus) or autograft. |
| Complex Regional Pain Syndrome (CRPS) | 1% - 3% | Idiopathic hyper-reactive sympathetic nervous system response to surgical trauma or tourniquet ischemia. | Prevention: Minimize tourniquet time; meticulous soft tissue handling; adequate post-operative analgesia. Salvage: Early aggressive physical therapy, Vitamin C supplementation, pharmacological management (pregabalin), lumbar sympathetic blocks. |
Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation protocol must be meticulously tailored to the specific procedure performed, the biological healing timeline of the tissues involved, and the patient's baseline functional status. Premature advancement through rehabilitation phases is a primary driver of procedural failure, particularly in ligamentous reconstructions and arthrodesis.
Rehabilitation following Arthroscopic Lateral Ligament Repair (Broström):
* Phase 1: Protection (Weeks 0-2): The patient is placed in a well-padded short leg splint in neutral dorsiflexion and slight eversion. The patient is strictly non-weight-bearing (NWB) on crutches. The primary goals are edema control and wound healing.
* Phase 2: Controlled Mobilization (Weeks 2-6): The splint is transitioned to a controlled ankle motion (CAM) boot. Weight-bearing is progressively advanced from partial to full weight-bearing as tolerated. Active range of motion (ROM) exercises are initiated, focusing strictly on sagittal plane motion (dorsiflexion and plantarflexion). Inversion and eversion are strictly prohibited to protect the healing ATFL construct.
* Phase 3: Strengthening and Proprioception (Weeks 6-12): The CAM boot is discontinued, and the patient transitions to a lace-up ankle brace. Aggressive physical therapy commences, focusing on peroneal muscle strengthening, isometric exercises, and proprioceptive training utilizing balance boards and dynamic stabilization drills.
* Phase 4: Return to Sport (Months 3-6): Sport-specific functional drills are introduced. Return to competitive play is permitted when the patient demonstrates symmetrical strength, full pain-free ROM, and the ability to perform dynamic cutting maneuvers without apprehension.
Rehabilitation following Arthroscopic Ankle Arthrodesis:
The arthroscopic approach significantly accelerates the rehabilitation timeline compared to traditional open arthrodesis, primarily due to the absence of massive soft tissue dissection and the preservation of the extensor retinaculum. However, the biology of bone healing remains unchanged.
* Phase 1: Strict Immobilization (Weeks 0-4): Postoperatively, the patient is placed in a rigid short leg cast or splint and maintained strictly non-weight-bearing.
* Phase 2: Protected Weight-Bearing (Weeks 4-8): Following initial soft tissue healing, the patient is transitioned to a CAM boot. Serial radiographs are obtained. If early trabecular bridging is visible, progressive partial weight-bearing is initiated.
* Phase 3: Full Weight-Bearing and Transition (Weeks 8-12): Progressive weight-bearing is advanced to full weight-bearing based on definitive radiographic evidence of fusion across the joint space. Once clinical and radiographic union is confirmed, the patient is transitioned to supportive athletic footwear, often utilizing a rocker-bottom sole modification to facilitate a normalized gait pattern in the absence of tibiotalar motion.
Summary of Landmark Literature and Clinical Guidelines
The integration of arthroscopic techniques into the standard orthopedic armamentarium is supported by a robust, albeit evolving, body of literature. It is imperative for the practicing surgeon to understand the levels of evidence supporting various interventions to guide clinical decision-making and patient counseling.
For Chronic Ankle Instability, the literature strongly supports arthroscopic and arthroscopic-assisted lateral ligament repair. However, as previously noted, historical adjuncts such as thermal capsular shrinkage carry a Grade C recommendation (poor evidence) due to unacceptably high rates of recurrent laxity and iatrogenic nerve injury. Diagnostic arthroscopy prior to any stabilization procedure is universally recommended to address concomitant intraarticular pathology, which is present in over 90% of CAI cases.
For Osteochondral Lesions of the Talus, the current literature supports a Grade B recommendation (fair evidence) for the arthroscopic treatment of OLTs via bone marrow stimulation (microfracture). Long-term outcomes demonstrate excellent pain relief and functional improvement for lesions smaller than 1.5 cm squared. Larger or cystic lesions may require more invasive open techniques such as osteochondral autograft transfer systems (OATS) or autologous chondrocyte implantation (ACI).
Regarding Posterior Impingement and Os Trigonum Syndrome, arthroscopic excision yields excellent functional results with significantly lower morbidity than open posteromedial or posterolateral approaches. However, a systematic review of the literature currently suggests a Grade C recommendation (poor quality evidence), primarily due to the lack of high-level randomized controlled trials comparing arthroscopic to open techniques, despite widespread, nearly universal clinical acceptance among sports medicine specialists.
Finally, the application of arthroscopy in acute Ankle Fractures is a rapidly expanding frontier. Arthroscopic evaluation before the fixation of an ankle fracture can detect latent syndesmosis injuries and occult chondral shear lesions. However, there remains controversy in the literature regarding whether the immediate treatment of these otherwise unknown pathological processes definitively improves long-term outcomes compared to standard fluoroscopic reduction. Consequently, there is currently a Grade I (incomplete) recommendation for routinely supplementing standard ankle fracture fixation with arthroscopy, highlighting an area ripe for future large-scale, prospective randomized controlled trials.
This academic synthesis is based on established protocols ---
