Tibiocalcaneal Arthrodesis Using Blade Plate Fixation
Comprehensive Introduction and Patho-Epidemiology
Evolution of Tibiocalcaneal Arthrodesis
The surgical management of severe hindfoot and ankle deformities, particularly those complicated by profound bone loss, avascular necrosis, or neuropathic collapse, has undergone a radical evolution over the past several decades. Before the 1990s, the prevailing dogma in orthopedic surgery dictated that reconstructive efforts such as pan-talar and tibiotalocalcaneal fusions strictly required an intact talus, robust vascularity, and an absolute absence of prior or current infection. Consequently, the presence of a fragmented talus or a Charcot joint rendered fusion virtually impossible under the classical paradigms. For the vast majority of these patients, the standard of care inevitably defaulted to a below-knee amputation, a devastating outcome with profound implications for patient morbidity and mortality.
The paradigm shifted significantly after 1990, driven by the pioneering work of surgeons such as Richard Alvarez, Delan Gaines, and Mark E. Easley. Their introduction of blade plate fixation for tibiocalcaneal arthrodesis revolutionized the approach to the unsalvageable ankle. This technique provided a robust mechanical solution that offered immediate deformity correction, rigid internal fixation, and reliable soft-tissue closure, even in the setting of severe talar fragmentation, avascular necrosis, or aggressive bone resorption. Soon after, this foundational work paved the way for complementary techniques, including intramedullary rods and Ilizarov circular external fixation. While each modality holds a critical place in the modern armamentarium, the 90-degree or 95-degree blade plate remains a cornerstone technique, uniquely suited for achieving massive compression and rotational stability in the compromised hindfoot.
Because of the steadily increasing life expectancy of patients with diabetes mellitus, neuropathic arthropathy (Charcot joint) has transitioned from a rare clinical curiosity to a highly prevalent and formidable orthopedic challenge. The resulting severe ankle and hindfoot deformities frequently progress to a non-braceable state. Attempting to bear weight on such profound malalignments introduces catastrophic ipsilateral stresses across the knee, leg, ankle, hindfoot, and forefoot. This abnormal biomechanical loading inevitably causes severe ligamentous laxity, stress fractures, and recurrent ulcerations. Left unchecked, these ulcerations serve as a direct conduit for polymicrobial cellulitis, deep space abscesses, and contiguous osteomyelitis, creating a limb-threatening triad that demands decisive surgical intervention.

Pathogenesis of Charcot Neuroarthropathy
The pathogenesis of Charcot neuroarthropathy is a complex, multifactorial cascade that requires the foundational presence of peripheral neuropathy, encompassing autonomic, sensory, and motor deficits. While the exact initiating mechanism remains a subject of academic debate—often divided between the neurotraumatic and neurovascular theories—it is universally accepted that the synergistic failure of these three nerve populations leads to the rapid and devastating destruction of the pedal architecture. Most commonly, this severe ankle and hindfoot deformity, characterized by talar fragmentation and resorption, is observed in patients with long-standing type 2 diabetic neuropathy. However, the differential etiology includes tabes dorsalis, Hansen disease, syringomyelia, alcoholic neuropathy, Charcot-Marie-Tooth disease, lumbar radiculopathy, peripheral nerve lesions, Riley-Day syndrome, renal dialysis, congenital insensitivity to pain, and repetitive intra-articular steroid injections.
Autonomic neuropathy plays a highly destructive, yet frequently underappreciated, role in the early stages of the disease. The sympathetic nervous system is responsible for supplying the small vessels, sweat glands, sebaceous glands, and the erector pilae muscles of the hair follicles. A deficit in these autonomic nerves results in the classic clinical presentation of dry, flaky, and warm skin with markedly decreased skin appendages. More insidiously, the profound loss of vasomotor tone produces a dramatic, unregulated increase in peripheral circulation. This creates an effect identical to a surgical sympathectomy: localized warmth, intense vasodilation, and a hyperemic state. This increased blood flow actively washes out bone mineral density, leading to localized osteopenia that renders the tarsal bones exceptionally susceptible to mechanical failure under normal physiological loads.
Sensory neuropathy acts as the permissive factor in this destructive cycle. Historically, medical teaching posited that complete anesthesia of the lower extremities was a prerequisite for the development of a Charcot joint and subsequent ulcerations. Modern clinical experience, however, reveals that patients frequently retain some degree of sensation, often complaining of dysesthesias such as stinging, burning, or cramping. The critical deficit lies in the loss of protective sensation (pain and pressure) and proprioception. Decreased proprioceptive feedback results in profound balance and gait abnormalities, predisposing the patient to repetitive microtrauma from falls, missed steps, or abnormal foot strikes. Because of the blunted pain response, these injuries—ranging from capsular sprains to overt fractures—are often perceived as minor by the patient, and occasionally missed by the initial evaluating physician or podiatrist. For the diabetic patient presenting with continued pain and swelling out of proportion to the reported injury, a high index of suspicion for an acute Charcot event must be maintained.
The Nutcracker Effect and Biomechanical Collapse
Motor neuropathy completes the triad by fundamentally altering the dynamic biomechanics of the lower extremity. The progressive denervation and subsequent weakness of the intrinsic and extrinsic muscles of the leg and foot create a profound muscle imbalance. Because the plantarflexors of the ankle possess a significantly greater cross-sectional area than the anterior dorsiflexors, this motor deficit inevitably leads to an overpowering, rigid equinus contracture, clinically manifesting as a tight heel cord. This fixed equinus position drastically alters the normal gait cycle, forcing the midfoot and forefoot to absorb massive, unphysiologic shear and compressive forces during the stance phase of walking.
In the hindfoot, this tight heel cord is directly responsible for exponentially increased stress on the talus. Normally, the ankle joint functions as a highly congruent hinge, allowing the tibia to rotate smoothly over the talar dome during dorsiflexion. In the presence of a rigid equinus contracture, this normal rotation is abruptly halted. Instead of gliding, the anterior lip of the distal tibia acts as a fulcrum, crushing down directly into the talar body. This phenomenon, widely referred to in orthopedic literature as the "nutcracker effect," subjects the talus to massive compressive forces that exceed its structural yield point, particularly when the bone is already osteopenic from autonomic hyperemia.
The result of the nutcracker effect is the catastrophic fragmentation and extrusion of the talar body. As the talus disintegrates, the hindfoot rapidly collapses into severe, non-braceable varus or valgus deformities. The mechanical axis of the lower extremity is completely lost, and the patient frequently ends up bearing weight directly on the medial or lateral malleolus. This devastating deformity is highly unstable, not amenable to traditional orthotic management, and is almost universally accompanied by a large, full-thickness pressure ulceration at the tip of the prominent malleolus. Without aggressive surgical realignment and stabilization, such as a tibiocalcaneal arthrodesis with a blade plate, the limb is destined for amputation.

Detailed Surgical Anatomy and Biomechanics
Osteology and Articular Relationships
A profound understanding of the complex osteology of the hindfoot is paramount when executing a tibiocalcaneal arthrodesis. The procedure fundamentally bypasses the tibiotalar and subtalar articulations, requiring the surgeon to create a direct, stable osseous bridge between the distal tibia and the calcaneus. In the setting of severe Charcot neuroarthropathy or advanced avascular necrosis, the talus is often reduced to a fragmented, necrotic shell. Total or subtotal talectomy is frequently required to debride this dead space and allow for direct apposition of the tibial plafond to the superior surface of the calcaneus. This massive structural alteration significantly shortens the limb, a necessary trade-off to achieve a plantigrade, braceable foot and to close the soft tissue envelope over the previously prominent malleoli.
The distal tibia presents a broad, metaphyseal flare that must be meticulously prepared. The articular cartilage and subchondral bone of the tibial plafond must be radically resected to expose bleeding, healthy cancellous bone. Similarly, the superior surface of the calcaneus, particularly the posterior facet, must be decorticated. The calcaneus itself is a trabecular bone with a thin cortical shell; its internal architecture is designed to withstand compressive loads but is highly susceptible to hardware pullout in osteoporotic or Charcot patients. Therefore, maximizing the surface area of contact between the broad tibial metaphysis and the decorticated calcaneal body is critical for achieving a successful arthrodesis.
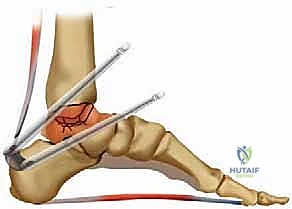
The fibula plays a dual role in this surgical approach. The lateral transfibular approach requires an osteotomy of the distal fibula, typically 10 to 14 centimeters proximal to the tip of the lateral malleolus. This excised fibular segment serves two vital purposes: it provides unparalleled, wide exposure to the lateral aspect of the tibiotalar and subtalar joints, and the excised bone can be morselized and utilized as highly osteogenic autograft to pack the arthrodesis site. The remaining lateral soft tissue envelope must be handled with extreme care, as the vascular supply to the skin flaps is often tenuous in this patient population.
Vascular Anatomy and Angiosomes
The vascular anatomy of the distal leg and hindfoot dictates the surgical approach and the viability of the postoperative soft tissue envelope. The concept of angiosomes—three-dimensional blocks of tissue supplied by specific source arteries—is highly relevant in diabetic limb salvage. The lateral approach utilized for blade plate fixation primarily traverses the angiosome of the peroneal artery. The peroneal artery descends along the medial crest of the fibula, giving off crucial calcaneal branches that supply the lateral heel and the lateral soft tissue envelope. Preservation of these perforating vessels, whenever possible, is essential for wound healing.
In diabetic patients, peripheral vascular disease frequently manifests as medial calcific sclerosis (Mönckeberg's arteriosclerosis), rendering the arteries rigid and non-compressible. Radiographs showing heavily calcified vessels are an early warning of impending neuropathic problems and compromised microvascular perfusion. Even if palpable pulses are present, the microcirculatory environment may be severely impaired. The surgeon must be acutely aware that correcting a severe valgus deformity via a lateral approach places the medial skin under significant tension, while the lateral skin may become redundant or kinked, potentially compromising the delicate microvascular perfusion and leading to catastrophic flap necrosis.
Preoperative vascular assessment is non-negotiable. If there is any question of adequate circulation, a toe-level Doppler index or transcutaneous oxygen index (TcPO2) at the first web space must be obtained. A TcPO2 reading greater than 45 mmHg is generally accepted as predictive of a 96% wound healing rate. If the vascular parameters fall below this threshold, mandatory consultation with a vascular surgeon for potential endovascular or open revascularization is required before any reconstructive orthopedic intervention is attempted. Proceeding with a massive hindfoot reconstruction in an ischemic limb is a direct pathway to major amputation.

Biomechanics of the Blade Plate Construct
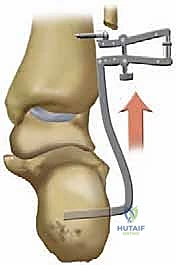
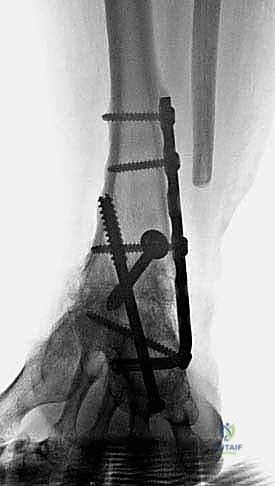
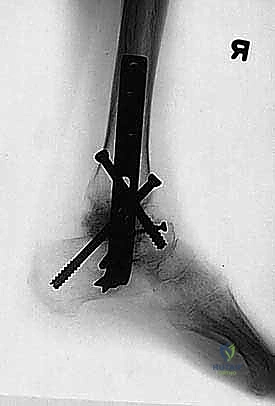
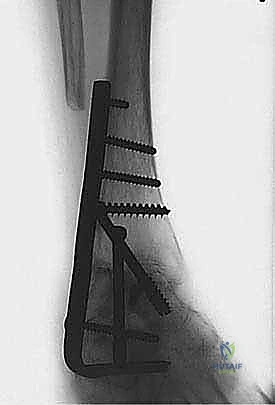
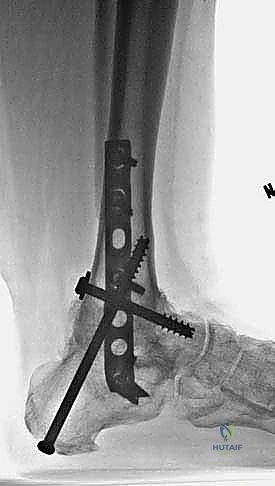
The biomechanical rationale for utilizing a 90-degree or 95-degree blade plate in tibiocalcaneal arthrodesis centers on its ability to provide exceptional multi-planar stability and massive dynamic compression. Originally designed for proximal femoral osteotomies and trauma, the blade plate has been ingeniously adapted for the hindfoot. Unlike intramedullary nails, which rely on the structural integrity of the calcaneus for distal locking and can act as an intramedullary stress riser, the blade plate functions as a fixed-angle cantilever device. The blade is driven directly into the dense trabecular bone of the posterior calcaneal tuberosity, providing a robust, rotationally stable anchor even in compromised bone stock.
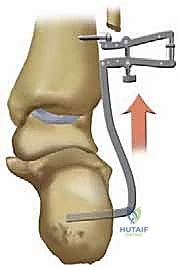
The application of the plate to the lateral aspect of the tibia allows the surgeon to utilize an articulated tension device (ATD) to generate immense compressive forces across the tibiocalcaneal interface. This compression is critical for two reasons: it maximizes the friction between the osteotomized bone ends, thereby neutralizing shear forces, and it directly stimulates primary bone healing through the principles of absolute stability. Furthermore, the lateral position of the plate acts as a tension band against the natural varus-inducing forces of the lower extremity during the stance phase of gait.
In cases of simultaneous tibiotalar and subtalar traumatic arthritis—frequently caused by talar fractures and untreated varus or valgus adult-acquired hindfoot deformities—the blade plate allows for precise, immediate deformity correction. By altering the angle of the seating chisel during insertion into the calcaneus, the surgeon can dial in the exact amount of valgus and sagittal plane alignment required before lagging the plate to the tibial shaft. This rigid, fixed-angle construct effectively immobilizes the entire hindfoot complex, shielding the healing arthrodesis site from the deleterious micromotion that typically leads to hypertrophic nonunion in the Charcot patient.


Exhaustive Indications and Contraindications
Patient Selection Criteria
The decision to proceed with a tibiocalcaneal arthrodesis using blade plate fixation is reserved for severe, limb-threatening pathology where conservative measures have been exhausted or are biomechanically impossible. The primary indication is an unbraceable Charcot neuroarthropathy characterized by profound talar body fragmentation, resorption, and impending or actual soft tissue compromise. When the deformity progresses to a point where a custom ankle-foot orthosis (AFO) or a Charcot Restraint Orthotic Walker (CROW) causes recurrent ulcerations due to unremitting pressure over bony prominences (such as the medial malleolus), surgical realignment becomes the only viable alternative to major amputation.
An additional, highly relevant indication for the blade plate is the presence of simultaneous tibiotalar and subtalar post-traumatic arthritis. This is frequently encountered in the sequelae of severe, high-energy talar fractures (e.g., Hawkins Type III or IV) that have progressed to avascular necrosis and subsequent structural collapse. Similarly, untreated, end-stage adult-acquired flatfoot deformity (Stage IV posterior tibial tendon dysfunction) resulting in rigid, severe valgus malalignment with tibiotalar joint involvement is an excellent candidate for this rigid, fixed-angle reconstruction. The blade plate is particularly advantageous in these scenarios because it does not require an intact talus for fixation.
Patient compliance is perhaps the most critical non-surgical indication. The patient must possess the cognitive capacity and social support to commit to a grueling 5 to 8 months of strict non-weight-bearing. They must fully comprehend that complications are frequent, and that hardware failure, infection, or nonunion may ultimately necessitate a salvage amputation. A highly effective method for gauging patient compliance is assessing their adherence to protocols during the preoperative immobilization phase in a total contact cast (TCC) or CROW boot.
Differential Diagnosis and Infection Exclusion
Before embarking on a major reconstructive arthrodesis, the surgeon must definitively rule out deep space infection, a task that is notoriously difficult in the diabetic foot. The clinical presentation of an acute Stage 0 or Stage I Charcot joint—erythema, profound edema, and calor—is virtually indistinguishable from acute cellulitis or osteomyelitis. Misdiagnosing an infection as an acute Charcot event and subsequently implanting massive internal hardware will result in a catastrophic, limb-losing complication. Monitoring systemic clinical and laboratory markers of infection (CRP, ESR, WBC count) is important, though often blunted in the diabetic patient with chronic renal insufficiency.
The physical examination is critical in this differentiation. The Brodsky test is a simple, highly effective clinical tool: if a suspected Charcot extremity is elevated above the level of the patient’s heart for 10 to 15 minutes, the erythema and edema will significantly dissipate due to the reduction of dependent venous pooling and autonomic hyperemia. Conversely, an infected extremity will remain persistently erythematous and engorged despite elevation. Furthermore, if the skin envelope is entirely intact without any history of recent ulceration or penetrating trauma, deep infection is highly unlikely, pointing toward a neuroarthropathic etiology.
When the diagnosis remains equivocal, particularly in the presence of a chronic, clean ulceration, advanced diagnostics are mandatory. Magnetic Resonance Imaging (MRI) can be helpful but is often confounded by the intense bone marrow edema present in both Charcot and osteomyelitis. A tagged white blood cell (WBC) scan combined with a sulfur colloid marrow scan offers higher specificity. However, the absolute gold standard for differentiating Charcot neuroarthropathy from osteomyelitis is a fluoroscopically guided, large-bore needle bone biopsy of the talus or calcaneus, sent for both histopathology and deep aerobic/anaerobic cultures.
| Indications for Blade Plate Arthrodesis | Absolute Contraindications |
|---|---|
| Non-braceable Charcot hindfoot deformity | Active, untreated deep space abscess or osteomyelitis |
| Talar fragmentation, resorption, or severe AVN | Severe peripheral vascular disease (TcPO2 < 45 mmHg) |
| Chronic ulceration secondary to bony prominence | Active, unmanaged smoking or nicotine use |
| Failed prior tibiotalocalcaneal (TTC) fusion | Profound medical instability (e.g., severe heart failure) |
| Post-traumatic simultaneous ankle/subtalar arthritis | Demonstrated inability to comply with NWB protocols |
| Salvage alternative to below-knee amputation (BKA) | Inadequate soft tissue envelope for lateral closure |

Pre-Operative Planning, Templating, and Patient Positioning
Clinical and Radiographic Evaluation
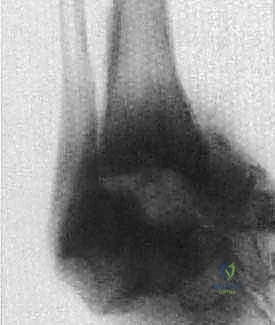
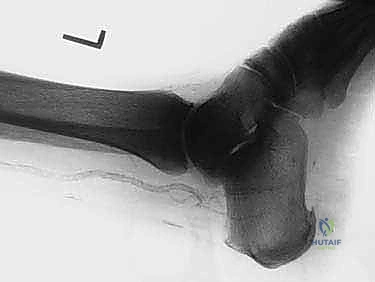
Comprehensive preoperative planning begins with a meticulous radiographic evaluation. Weight-bearing anteroposterior (AP), lateral, and mortise views of the ankle, along with AP, lateral, and axial views of the foot, are mandatory. These images allow the surgeon to assess the degree of talar collapse, the magnitude of the varus or valgus deformity, and the presence of calcified vessels. In the setting of severe deformity, standard radiographs may be difficult to interpret due to overlapping osseous structures and profound subluxation. Therefore, a multi-planar computed tomography (CT) scan is highly recommended to accurately assess the remaining bone stock of the calcaneus and distal tibia, map out cystic lesions, and plan the trajectory of the blade plate.
Templating is a critical step that should not be bypassed. Using digital or acetate templates on the lateral radiograph, the surgeon must determine the appropriate blade length, plate length, and the optimal entry point on the posterior calcaneal tuberosity. The goal is to ensure the blade captures the maximum volume of dense trabecular bone in the calcaneus without breaching the plantar or medial cortices. Additionally, the templating process helps estimate the amount of tibial shortening that will occur following talectomy and joint preparation, allowing the surgeon to counsel the patient regarding postoperative limb length discrepancy and the potential need for a shoe lift.
Medical clearance is an absolute prerequisite, requiring a multidisciplinary approach involving the patient’s internist, diabetologist, and potentially a cardiologist. The emphasis must be placed on strict perioperative glycemic control. Hemoglobin A1c levels should ideally be optimized below 7.5%, as elevated perioperative glucose levels are directly correlated with impaired leukocyte function, diminished collagen cross-linking, and exponential increases in surgical site infections. Nutritional status must also be evaluated; a serum albumin level below 3.5 g/dL or prealbumin below 15 mg/dL indicates malnutrition and significantly impairs wound healing and bone consolidation.
Medical Optimization and Soft Tissue Management
The management of the soft tissue envelope begins weeks, if not months, prior to the operative date. If the patient presents with a chronic ulceration, typically at the tip of the medial or lateral malleolus, a trial of nonoperative CROW bracing or aggressive total contact casting (TCC) is warranted. Ideally, wound healing should be completely accomplished and maintained prior to surgical intervention. If the ulcer is clean and granulating but fails to close due to the underlying biomechanical pressure, surgery may proceed, provided there is absolute certainty that no underlying osteomyelitis exists.
In the immediate preoperative period, the extremity should be maintained in a well-padded, non-weight-bearing splint or cast to minimize edema. The skin must be meticulously inspected for any signs of tinea pedis, maceration, or nascent breakdown, particularly in the web spaces and around the heel. Any dermatological issues must be aggressively treated with topical antifungals or barrier creams to ensure the surgical field is pristine.
On the day of surgery, the skin is prepared with a tincture of iodine and alcohol solution. It is critical to note that standard Betadine paint can leave a residue that prevents adhesive drapes (such as Tegaderm) from sticking securely to the skin. This is particularly problematic as the surgeon must effectively mark the curvilinear incision and isolate any existing, clean ulcerations from the primary surgical field. Ulcers are thoroughly debrided of any fibrinous slough, irrigated, and then tightly sealed beneath a sterile Tegaderm dressing to prevent cross-contamination during the extensive reconstructive procedure.
Patient Positioning and Operating Room Setup
Proper patient positioning is critical for obtaining adequate exposure and ensuring unimpeded fluoroscopic imaging throughout the case. The patient is placed in the lateral decubitus position with the operative extremity facing upward. A radiolucent bean bag is utilized to secure the torso, and all bony prominences (axilla, greater trochanter, peroneal nerve of the down leg) are meticulously padded to prevent positioning neuropathies. The operative table should be perfectly leveled to allow the surgeon to accurately judge the rotational and sagittal alignment of the limb during the reconstruction.
The extremity is prepped and draped freely above the knee to allow for assessment of the mechanical axis of the entire lower limb. The surgeon must ensure that the anterior superior iliac spine (ASIS) and the patella can be easily palpated through the sterile drapes; these landmarks
Clinical & Radiographic Imaging Archive