Orthopedic Spine 2026 MCQs: Board Review Questions & Answers (Part 3)

Key Takeaway
Your ultimate guide to Orthopedic Spine 2026 MCQs: Board Review Questions & Answers (Part 3) starts here. Top-rated Orthopedic Spine 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Spine 2026 MCQs: Board Review Questions & Answers (Part 3)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
What is the most common complication of halo vest immobilization in adults?
Explanation
Question 2
What is the most common neurologic complication following an anterior cervical diskectomy and fusion?
Explanation
Question 3
An otherwise healthy 45-year-old woman reports the onset of severe right leg pain. Figure 20a shows an axial MRI scan of the L4-5 level, and Figure 20b shows a sagittal view with the arrow at the L4-5 level. What nerve root is the most likely source of her pain?
Explanation
Question 4
Which of the following forms of nonsurgical management is considered best for acute low back pain without radiculopathy?
Explanation
Question 5
A type 2A hangman's fracture, which has the potential to overdistract with traction, has which of the following hallmark findings?
Explanation
Question 6
Figures 21a and 21b show the radiographs of a 22-year-old man who was shot through the abdomen the previous evening. An exploratory laparotomy performed at the time of admission revealed a colon injury. Current examination reveals no neurologic deficits. Management for the spinal injury should include
Explanation
Question 7
Stability at the atlanto-occipital joint is provided mainly by
Explanation
Question 8
Which of the following are considered characteristic features of degeneration of a disk?
Explanation
Question 9
What spinal nerves in the cauda equina are primarily responsible for innervation of the bladder?
Explanation
Question 10
Figures 22a and 22b show the radiograph and sagittal MRI scan of the upper cervical spine of a 62-year-old woman who has had a long history of rheumatoid arthritis. Following hospitalization and skeletal traction, her symptoms improve significantly, her neurologic examination returns to normal, and repeat radiographs show a normal occiput and C1-C2 relationship. Treatment should now include
Explanation
Question 11
What is the prognosis for ambulation, from best to worst, for patients with an incomplete spinal cord injury?
Explanation
Question 12
A skeletally mature 15-year-old girl who was thrown from the car in a rollover accident sustained the injuries shown in Figures 23a through 23d. Examination reveals no neurologic deficit, but the patient has moderate posterior spinal tenderness at the level of the injury. What is the most appropriate treatment?
Explanation
Question 13
The MRI scan shown in Figure 24 reveals a right-sided herniated nucleus pulposus at L4-5 in a patient with pain in the right leg. Administration of a caudal epidural steroid injection provides immediate relief. Over the next week he notes generalized weakness of the lower extremities and has one episode of urinary incontinence. What is the next most appropriate step in management?
Explanation
Question 14
At the L4-5 level, what is the location of the S2-5 nerve roots in relationship to the L5 and S1 nerve roots?
Explanation
Question 15
A comparison of dural tears repaired with suture alone and those treated by suture with fibrin glue supplementation will reveal which of the following findings?
Explanation
Question 16
A 19-year-old woman reports lower back pain following a motor vehicle accident. Radiographs obtained immediately after the accident and a bone scan obtained 4 weeks later are shown in Figures 25a through 25c. The patient asks questions regarding the cause, genetics, and natural history of her condition. She should be informed that the condition was
Explanation
Question 17
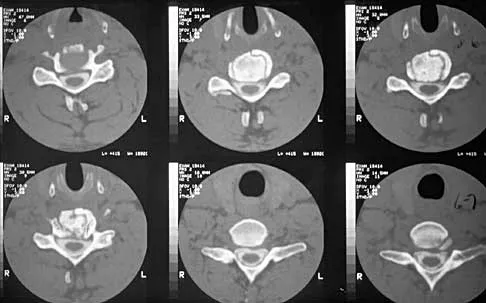
A patient underwent an anterior cervical diskectomy and interbody fusion for a C5-6 herniated nucleus pulposus and left C6 radiculopathy 8 months ago. He now reports new onset of severe neck pain and left C6 radicular pain, with wrist extension weakness. The radiograph and CT scan shown in Figures 26a and 26b reveal pseudarthrosis at C5-6. The next step in management should consist of
Explanation
Question 18
A 44-year-old farmer involved in a rollover accident on his tractor sustained an L1 burst fracture with a 20% loss of anterior vertebral body height, 30% canal compromise, and 15 degrees of kyphosis. He remains neurologically intact. The preferred initial course of action should consist of
Explanation
Question 19
A 40-year-old carpenter has a 3-month history of right arm pain and neck pain that now leaves him unable to work. Examination reveals a positive Spurling test, weakness of the biceps, and a mildly positive Hoffman's sign on the right side. Electromyography and nerve conduction velocity studies show a right C6 deficit. Figures 27a through 27c show MRI scans that reveal two-level spondylotic disease at C5-6 and C6-7, a large herniated nucleus pulposus at C5-6, and a prominent ridge and hard disk at C6-7. Nonsurgical management fails to provide relief, so the patient elects surgical intervention. Which of the following surgical options would give the best long-term results?
Explanation
Question 20
A patient with rheumatoid arthritis has an unstable pseudarthrosis after undergoing C1-2 posterior fusion. No neurologic deficits are noted, and repair with posterior transarticular fixation screws and a posterior wiring technique at C1-2 is planned. Which of the following preoperative studies offers the best visualization?
Explanation
Question 21
An elderly patient falls and sustains an extension injury to the neck that results in upper extremity weakness, spared perianal sensation, and lower extremity spasticity. These findings best describe what syndrome?
Explanation
Question 22
In the treatment of thoracic disk herniations, what approach is associated with the highest risk of iatrogenic paraplegia?
Explanation
Question 23
Which of the following factors is the strongest predictor of vertebral fracture in postmenopausal women?
Explanation
Question 24
A 23-year-old man sustains a unilateral jumped facet with an isolated cervical root injury in a motor vehicle accident. Acute reduction results in some initial improvement of his motor weakness. Over the next 48 hours, examination reveals ipsilateral loss of pain and temperature sensation in his face, limbs, and trunk, as well as nystagmus, tinnitus, and diplopia. What is the most likely etiology for these changes?
Explanation
Question 25
A 60-year-old woman with a history of breast cancer has progressive paraparesis. The MRI scan is shown in Figure 28. What form of management is most likely to restore or maintain ambulation?
Explanation
Question 26
A 65-year-old man undergoes a C3-C6 posterior laminectomy and instrumented fusion for severe cervical spondylotic myelopathy. On postoperative day 2, he develops profound weakness in his bilateral deltoid and biceps muscles (0/5 strength). His sensation is intact, and his myelopathic symptoms in the lower extremities have improved. What is the most appropriate initial management?
Explanation
Question 27
When evaluating a 68-year-old female for adult spinal deformity, which of the following postoperative spinopelvic parameters is most closely correlated with achieving a satisfactory health-related quality of life (HRQOL) score?
Explanation
Question 28
An 82-year-old man with long-standing, advanced ankylosing spondylitis presents after a ground-level fall. He complains of severe neck pain but is neurologically intact. Computed tomography demonstrates a displaced extension-distraction fracture traversing the C6-C7 disc space and posterior elements. What is the recommended definitive management?
Explanation
Question 29
An 80-year-old man sustains a Type II odontoid fracture after a ground-level fall. He has a history of severe COPD and coronary artery disease, but his neurologic examination is completely normal. Which of the following treatment modalities has the highest associated mortality rate in this specific patient population?
Explanation
Question 30
A 24-year-old woman is involved in a high-speed motor vehicle collision while wearing only a lap belt.
Radiographs and CT scans reveal a transverse fracture through the L2 vertebral body, pedicles, and spinous process (Chance fracture). Which of the following associated injuries is most critical to rule out?

Explanation
Question 31
A 70-year-old man with pre-existing cervical spondylosis trips and falls forward, striking his forehead. He presents with profound weakness in his upper extremities, particularly affecting his intrinsic hand muscles, but retains the ability to ambulate with only mild lower extremity weakness. What is the pathophysiological mechanism of his neurologic deficit?
Explanation
Question 32
A 65-year-old woman with a 20-year history of rheumatoid arthritis undergoes routine cervical spine flexion-extension radiographs. She is completely asymptomatic. Which of the following radiographic measurements represents an absolute indication for prophylactic surgical stabilization?
Explanation
Question 33
Recombinant human bone morphogenetic protein-2 (rhBMP-2) is sometimes utilized off-label in anterior cervical diskectomy and fusion (ACDF). Which of the following is the most significant, life-threatening complication associated with its use in the anterior cervical spine?
Explanation
Question 34
A 55-year-old diabetic male presents with severe mid-back pain, fevers, and rapidly progressive lower extremity paraparesis. MRI reveals a T8-T10 ventral epidural abscess causing severe anterior spinal cord compression, accompanied by T9-T10 discitis. What is the most appropriate surgical approach?
Explanation
Question 35
A 60-year-old man with metastatic renal cell carcinoma presents with mechanical back pain. MRI shows a solitary L2 vertebral metastasis with early epidural extension, but the epidural space is largely patent and there is no spinal cord compression. He is neurologically intact. According to the NOMS framework, how should this lesion best be managed?
Explanation
Question 36
A 45-year-old male presents with right arm pain radiating down the posterior aspect of his forearm into his middle finger. Examination reveals weakness in triceps extension and an absent triceps reflex. A Spurling maneuver reproduces his symptoms. Compression of which cervical nerve root is most likely responsible?
Explanation
Question 37
A 68-year-old man complains of bilateral calf pain and heaviness that worsens with walking. He states the pain is reliably relieved when he leans forward on a shopping cart at the grocery store. Which of the following activities or findings is most specific for differentiating his neurogenic claudication from vascular claudication?
Explanation
Question 38
A 14-year-old competitive gymnast presents with persistent lower back pain unresponsive to 6 months of physical therapy and bracing. Radiographs demonstrate a Grade II L5-S1 isthmic spondylolisthesis. She is neurologically intact. Surgical intervention is planned. Which of the following procedures is considered the most appropriate standard of care?
Explanation
Question 39
A 30-year-old man involved in a high-speed collision sustains a traumatic spondylolisthesis of the axis (Hangman's fracture). Imaging demonstrates a fracture through the bilateral pars interarticularis with 15 degrees of angulation and 4 mm of translation (Levine-Edwards Type II). What is the classic mechanism of this specific injury pattern?
Explanation
Question 40
A 25-year-old male falls from a ladder.
CT imaging shows a T12 burst fracture with 30% canal compromise. MRI confirms that the posterior ligamentous complex (PLC) is fully intact. The patient has normal motor and sensory exams in his lower extremities. What is his Thoracolumbar Injury Classification and Severity (TLICS) score, and what is the recommended treatment?
Explanation
Question 41
A 65-year-old man presents with bilateral leg pain when walking. He notes the pain is relieved when pushing a shopping cart but worsens when walking down a hill. Pulse examination is normal. Which of the following is the most likely diagnosis?
Explanation
Question 42
A 60-year-old man presents with hand clumsiness and frequent falls. On physical exam, tapping the distal brachioradialis tendon results in spontaneous finger flexion without elbow flexion. This reflex finding localizes the primary pathology to which spinal cord level?
Explanation
Question 43
In a patient with longstanding rheumatoid arthritis, which of the following radiographic findings is the strongest indication for operative intervention to prevent irreversible neurologic damage?
Explanation
Question 44
An 82-year-old frail female sustains a minimally displaced Type II odontoid fracture after a mechanical fall. What is the most appropriate initial management, considering her age and comorbidities?
Explanation
Question 45
A 45-year-old man presents with severe lower back pain, bilateral sciatica, and perineal numbness. Which of the following objective findings is most sensitive for diagnosing early urinary dysfunction associated with cauda equina syndrome?
Explanation
Question 46
A 12-year-old girl is diagnosed with adolescent idiopathic scoliosis. She is premenarcheal with a Risser stage of 0. Standing radiographs reveal a right thoracic curve of 35 degrees. What is the most appropriate next step in management?
Explanation
Question 47
A 50-year-old woman presents with progressive myelopathy due to a large, calcified, central disc herniation at T8-T9. What is the most appropriate surgical approach for decompression?
Explanation
Question 48
A 35-year-old man is involved in a motor vehicle accident and sustains a traumatic spondylolisthesis of C2 (Hangman's fracture). Imaging shows a fracture through the pars interarticularis with 4 mm of translation. This injury is best described by which of the following mechanisms?
Explanation
Question 49
A 25-year-old man wearing a lap seatbelt without a shoulder harness is involved in a high-speed collision. He sustains a flexion-distraction injury of the L1 vertebra (Chance fracture). What concomitant injury must be aggressively evaluated?
Explanation
Question 50
A 65-year-old Asian male presents with progressive hand clumsiness and gait imbalance. Imaging shows multilevel Ossification of the Posterior Longitudinal Ligament (OPLL) with a K-line negative cervical spine. Which of the following procedures is generally considered CONTRAINDICATED as a standalone procedure for this patient?
Explanation
Question 51
A 68-year-old woman undergoes corrective surgery for flatback syndrome. To achieve optimal sagittal balance and minimize compensatory mechanisms, her postoperative lumbar lordosis (LL) should be matched to within 10 degrees of which of the following spinopelvic parameters?
Explanation
Question 52
Following a C3-C7 posterior cervical laminectomy and fusion for severe cervical spondylotic myelopathy, a patient develops isolated, unilateral deltoid and biceps weakness on postoperative day 3. Sensation remains intact. What is the most likely etiology of this new deficit?
Explanation
Question 53
An 82-year-old man sustains a Type II odontoid fracture after a ground-level fall. He has severe medical comorbidities, including heart failure and severe chronic obstructive pulmonary disease. What is the most appropriate initial management strategy?
Explanation
Question 54
A 45-year-old man presents with severe right anterior thigh pain and new-onset weakness in knee extension. MRI reveals a far lateral (extraforaminal) disc herniation at the L3-L4 level. Which nerve root is most likely compressed by this lesion?
Explanation
Question 55
A 65-year-old male presents with neurogenic claudication. Radiographs demonstrate a degenerative Grade 1 spondylolisthesis at L4-L5 with 4 mm of dynamic translation on flexion-extension views. He has failed 6 months of non-operative management. What is the most appropriate surgical treatment?
Explanation
Question 56
A 24-year-old male is involved in a motor vehicle collision.
CT of the cervical spine shows a Type II odontoid fracture with 7 mm of posterior displacement. The patient is neurologically intact. What is the most appropriate definitive management?

Explanation
Question 57
A 45-year-old female presents with progressive clumsiness in her hands and wide-based gait. Exam reveals positive Hoffmann's signs bilaterally. MRI reveals severe cervical cord compression at C4-C6 with T2 signal changes in the spinal cord. Upright radiographs demonstrate a 15-degree fixed cervical kyphosis. What is the most appropriate surgical approach?
Explanation
Question 58
A 68-year-old man presents with bilateral leg pain and fatigue that worsens with walking. Which of the following historical findings is most specific for differentiating neurogenic claudication from vascular claudication?
Explanation
Question 59
A 55-year-old woman with a 20-year history of rheumatoid arthritis presents with progressive hand clumsiness and hyperreflexia. Radiographs reveal atlantoaxial instability. Which of the following radiographic measurements is the strongest predictor of postoperative neurologic recovery?
Explanation
Question 60
A 74-year-old man falls and sustains a Type II odontoid fracture. Which of the following factors most significantly increases his risk of fracture nonunion with conservative halo vest management?
Explanation
Question 61
A 45-year-old man presents with severe left anterior thigh pain and trace quadriceps weakness. An MRI demonstrates a far lateral (extraforaminal) disc herniation at the L3-L4 level. Which nerve root is most likely compressed?
Explanation
Question 62
A 62-year-old man with ankylosing spondylitis presents to the ER after a ground-level fall. He has severe neck pain but intact neurology. A CT scan reveals a transverse fracture through the C5-C6 disc space. He is admitted and placed in a hard collar. Several hours later, he develops progressive bilateral upper and lower extremity weakness. What is the most likely cause?
Explanation
Question 63
A 13-year-old premenarchal girl (Risser 0) is diagnosed with adolescent idiopathic scoliosis. Her right thoracic curve measures 34 degrees. What is the most appropriate next step in management?
Explanation
Question 64
During a posterior spinal fusion for scoliosis, neuromonitoring demonstrates a sudden, sustained loss of motor evoked potentials (MEPs) in both lower extremities, while somatosensory evoked potentials (SSEPs) remain intact. What is the most likely pathophysiologic cause?
Explanation
Question 65
A 28-year-old man sustains a flexion-distraction (Chance) fracture of L2 during a high-speed motor vehicle collision. Which of the following injuries is most highly associated with this specific fracture pattern?
Explanation
Question 66
A 52-year-old man presents with right arm pain and numbness radiating to his thumb and index finger. Examination reveals weakness in wrist extension and a diminished brachioradialis reflex. Which cervical disc level is most likely affected?
Explanation
Question 67
A 16-year-old boy presents with progressive mid-back pain. Lateral radiographs show anterior wedging of 7 degrees in four consecutive thoracic vertebrae and irregular vertebral endplates with Schmorl's nodes. Which of the following is the most likely diagnosis?
Explanation
Question 68
A 68-year-old man with a history of diffuse idiopathic skeletal hyperostosis (DISH) presents with progressive solid food dysphagia. What is the most likely pathophysiologic mechanism for his symptom?
Explanation
Question 69
A 32-year-old male construction worker has a symptomatic Grade II isthmic spondylolisthesis at L5-S1. He complains of severe bilateral leg pain. Which nerve root is most likely being compressed, and at what anatomical location?
Explanation
Question 70
A 58-year-old woman with a history of renal cell carcinoma presents with progressive paraparesis. MRI reveals a large metastatic lesion in the T8 vertebral body causing significant epidural spinal cord compression. What is the most appropriate management strategy?
Explanation
Question 71
A 71-year-old man undergoes a multilevel posterior cervical laminectomy and instrumented fusion for severe cervical spondylotic myelopathy. On postoperative day 2, he develops isolated profound weakness in right shoulder abduction and elbow flexion, with no sensory deficits or leg symptoms. What is the most likely diagnosis?
Explanation
Question 72
A 45-year-old male intravenous drug user presents with intractable back pain, fevers, and acute urinary retention. MRI reveals an L3-L4 epidural abscess with significant canal compromise. What is the most appropriate next step in management?
Explanation
Question 73
During a routine physical exam of a 60-year-old man with neck pain, tapping the distal brachioradialis tendon results in reflexive flexion of the ipsilateral fingers without elbow flexion. What does this specific finding suggest?
Explanation
Question 74
A 24-year-old unrestrained passenger in an MVC sustains a traumatic spondylolisthesis of C2 (Hangman's fracture). Radiographs show a fracture through the pars interarticularis with severe angulation but minimal translation. Flexion-extension views demonstrate severe instability in flexion. This is classified as a Type IIA fracture. Which of the following treatments is absolutely contraindicated?
Explanation
Question 75
A 48-year-old woman undergoes a straightforward L4-L5 microdiscectomy. During the procedure, a small incidental durotomy is primarily repaired with a watertight suture. On postoperative day 1, she complains of a severe headache that worsens when she sits up and resolves when she lies flat. What is the best initial management?
Explanation
Question 76
A 6-year-old child with progressive bilateral cavovarus foot deformities is noted to have a small sacral dimple and an asymmetric gait. MRI of the lumbar spine reveals the conus medullaris terminating at the L4 level and a thickened filum terminale. What is the most appropriate surgical treatment?
Explanation
Question 77
A 65-year-old man undergoes an L2-L5 posterior laminectomy and instrumented fusion. Three weeks postoperatively, he presents with worsening back pain, fever, and a purulent draining sinus tract from his incision. His hardware appears well-fixed on radiographs. What is the most appropriate surgical management?
Explanation
Question 78
A 45-year-old male presents with severe right-sided leg pain and weakness in knee extension. MRI of the lumbar spine reveals a far-lateral (extraforaminal) disc herniation at the L4-L5 level. Which nerve root is most likely compressed in this scenario?
Explanation
Question 79
A 60-year-old male undergoes a C3-C6 cervical laminoplasty for multi-level ossification of the posterior longitudinal ligament (OPLL). On postoperative day three, he develops new-onset, profound weakness in shoulder abduction and elbow flexion, with no sensory deficits. What is the most likely diagnosis?
Explanation
Question 80
A 55-year-old female with long-standing rheumatoid arthritis presents with progressive neck pain and myelopathic symptoms. Which of the following radiographic measurements is the strongest indication for surgical stabilization to prevent irreversible neurologic deficit?
Explanation
Question 81
A 62-year-old male presents with rapidly progressive paraparesis. Imaging reveals a solitary, large osteolytic metastatic lesion in the L2 vertebral body with severe epidural spinal cord compression. Biopsy confirms renal cell carcinoma. What is the most appropriate surgical management strategy?
Explanation
Question 82
In the preoperative planning for adult spinal deformity correction, achieving a harmonious sagittal profile is a primary goal. Which of the following formulas correctly describes the relationship between the pelvic parameters?
Explanation
Question 83
A 13-year-old premenarcheal female presents with a right thoracic prominence. Radiographs reveal an adolescent idiopathic scoliosis (AIS) curve of 32 degrees. Her Risser stage is 1. What is the most appropriate management?
Explanation
Question 84
A 40-year-old male presents to the emergency department with severe lower back pain, bilateral sciatica, and perineal numbness. Which of the following objective findings is most sensitive for diagnosing early cauda equina syndrome?
Explanation
Question 85
A 55-year-old male with known Ankylosing Spondylitis presents to the emergency room with acute neck pain after a low-speed motor vehicle collision. A review of the initial lateral cervical radiograph is shown.
What is the most appropriate next step in management?
Explanation
Question 86
The use of recombinant human bone morphogenetic protein-2 (rhBMP-2) in anterior cervical diskectomy and fusion (ACDF) has been associated with which of the following significant postoperative complications?
Explanation
Question 87
During a posterior lumbar spinal fusion, the surgeon prepares to insert a pedicle screw at the L4 level. What is the correct anatomical starting point for a traditional straightforward trajectory L4 pedicle screw?
Explanation
Question 88
A 35-year-old male falls from a roof. Review the provided imaging.
When calculating the Thoracolumbar Injury Classification and Severity (TLICS) score to determine the need for operative stabilization, which MRI finding is given the most weight?
Explanation
Question 89
A 65-year-old diabetic male develops severe, unremitting low back pain and fever. MRI confirms pyogenic spondylodiscitis at L3-L4. What is the most common route of pathogen transmission leading to this condition in an adult?
Explanation
Question 90
An 82-year-old female sustains a Type II odontoid fracture after a fall from standing. Which of the following is a recognized risk factor for nonunion if this fracture is treated non-operatively with a rigid cervical collar?
Explanation
Question 91
A 68-year-old female presents with neurogenic claudication. Radiographs reveal an L4-L5 degenerative spondylolisthesis. Anatomically, what is the primary restraint that typically prevents anterior translation of L4 on L5, and becomes compromised in this condition?
Explanation
Question 92
A 22-year-old male is involved in a high-speed motorcycle accident resulting in a complete spinal cord injury at the T6 level. He initially presents in a state of spinal shock. What clinical finding definitively marks the end of the spinal shock phase?
Explanation
Question 93
A 48-year-old male presents with shooting pain down his right arm, associated with weakness in wrist extension. The brachioradialis reflex is diminished. Review the MRI shown.
Based on the physical exam, which specific physical examination finding further supports the affected nerve root?
Explanation
Question 94
A 35-year-old man presents after a motor vehicle collision with severe neck pain and right-sided C6 radiculopathy. CT imaging demonstrates a right unilateral C5-C6 facet dislocation. MRI reveals a large, extruded disc herniation posterior to the C5-C6 interspace, severely compressing the thecal sac. What is the most appropriate next step in management?
Explanation
Question 95
A 68-year-old woman undergoes posterior spinal instrumentation and fusion from the lower thoracic spine to the pelvis for adult degenerative scoliosis. Postoperatively, she is at risk for developing proximal junctional kyphosis (PJK). Which of the following factors is most strongly associated with an increased risk of PJK?
Explanation
Question 96
A 62-year-old man presents with progressive hand clumsiness and an unsteady gait. Physical examination reveals lower extremity hyperreflexia, a positive Hoffmann sign bilaterally, and a positive inverted brachioradialis reflex. When the brachioradialis tendon is tapped, there is a diminished radial reflex but spontaneous, brisk flexion of the fingers. At which of the following cervical intervertebral levels is the spinal cord compression most likely located?
Explanation
None
