AAOS & ABOS Orthopedic Spine MCQs (Part 3): Cervical Myelopathy, Lumbar Stenosis | 2026 Board Prep

Key Takeaway
This high-yield question set for AAOS/ABOS/OITE exams, Part 3, focuses on critical Orthopedic Spine topics. Questions cover cervical myelopathy diagnosis and surgical indications, lumbar spinal stenosis pathophysiology and treatment options, and complex adult spinal deformity classification and management strategies. Master these key areas for 2026 board success.
AAOS & ABOS Orthopedic Spine MCQs (Part 3): Cervical Myelopathy, Lumbar Stenosis | 2026 Board Prep
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 58-year-old woman with rheumatoid arthritis has progressive neck pain, upper extremity and lower extremity weakness, and difficulty with fine motor movements. Examination reveals hyperreflexia with mild to moderate objective weakness but the patient has no difficulty with ambulation for short distances. What is the most important preoperative imaging finding that predicts full neurologic recovery with surgical stabilization?
Explanation
Question 2
Figures 20a through 20d show the radiographs and MRI scans of a 59-year-old woman who has had symptoms consistent with progressive neurogenic claudication and back pain for the past 9 months. In the last 6 months, nonsurgical management consisting of nonsteroidal anti-inflammatory drugs, physical therapy, and a series of epidural steroid injections have been used; however the injections, while beneficial, have provided only temporary relief of her symptoms. What is the most appropriate management at this time?
Explanation
Question 3
A 29-year-old man reports a 2-week history of severe neck pain after being struck sharply on the back of the head and neck while moving a refrigerator down a flight of stairs. Initial evaluation in the emergency department revealed no obvious fracture and he was discharged in a soft collar. Neurologic examination is within normal limits, and radiographs taken in the office are shown in Figures 21a through 21c. Subsequent MRI scans show intra-substance rupture of the transverse atlantal ligament. What is the most appropriate treatment option at this time?
Explanation
Question 4
Figure 22 reveals what anatomic variant of the lumbar spine?
Explanation
Question 5
Posterior lumbar spine arthrodesis may be associated with adjacent segment degeneration cephalad or caudad to the fusion segment. Which of the following is the predicted rate of symptomatic degeneration at an adjacent segment warranting either decompression and/or arthrodesis at mid-range follow-up (5-10 years) after lumbar fusion?
Explanation
Question 6
A 24-year-old man who was involved in a high speed motor vehicle accident is transferred for definitive care after having been diagnosed with an acute spinal cord injury from a fracture-dislocation at C6-7. He has a complete C6 neurologic level and it is now approximately 10 hours from his injury. What is the most appropriate pharmacologic treatment at this time?
Explanation
Question 7
Figures 23a and 23b show the MRI scans of a 50-year-old woman who has increasing gait disturbance. She reports three falls in the past week. Examination reveals hyperreflexia, motor weakness in the biceps and triceps, and a positive Hoffman's sign. What is the most appropriate treatment plan?
Explanation
Question 8
What structure (arrow) is shown in Figure 24?
Explanation
Question 9
The best patient-related outcomes, following the surgical treatment of cauda equina syndrome secondary to a large L5-S1 disk herniation, are most closely related to which of the following?
Explanation
Question 10
A 45-year-old man undergoes an anterior cervical diskectomy and fusion at C5-6 and C6-7 with instrumentation. During the first postoperative visit at 1 week, the patient reports difficulty swallowing and mild anterior cervical tightness. The anterior wound is benign and the patient denies any dyspnea or shortness of breath. A postoperative radiograph is seen in Figure 25. What is the most appropriate management at this time?
Explanation
Question 11
Steroids are thought to prevent neurologic deterioration after traumatic spinal cord injury by which of the following mechanisms?
Explanation
Question 12
Which of the following mechanisms of inhibition has been linked to cigarette smoking and lumbar spinal fusion?
Explanation
Question 13
Which of the following is considered the most effective means of identifying an evolving motor tract injury during cervical spine surgery?
Explanation
Question 14
A previously healthy 29-year-old man reports a 2-day history of severe atraumatic lower back pain. He denies any bowel or bladder difficulties and no constitutional signs. Examination is consistent with mechanical back pain. No focal neurologic deficits or pathologic reflexes are noted. What is the most appropriate management?
Explanation
Question 15
Sacral fractures are most likely to be associated with neurologic deficits when they involve what portion of the sacrum?
Explanation
Question 16
Which of the following is associated with the use of bisphosphonates in the setting of metastatic breast cancer to the spine?
Explanation
Question 17
A 67-year-old retired steelworker was involved in a motor vehicle accident and sustained a midcervical spinal cord injury. Radiographs and MRI scans reveal severe cervical stenosis and spondylosis without fractures or dislocations. Neurologic examination reveals an ASIA C spinal cord impairment with greater motor involvement of the upper extremities than the lower extremities. What is the probability that the patient eventually will become ambulatory?
Explanation
Question 18
A 20-year-old man involved in a motor vehicle accident is brought to the emergency department with a C6-7 unilateral facet dislocation. His neurologic examination reveals a focal left-sided C7 nerve root palsy. He is awake and cooperative with questioning and has no other obvious traumatic injuries. What is the most appropriate treatment at this time?
Explanation
Question 19
A 66-year-old man reports a 2-week history of worsening low back and leg pain. He reports that his pain is aggravated by lying down and relieved by standing and walking. He notes that he has been losing weight recently and that his pain has been awakening him during the night. His medical history is significant for hypertension, coronary artery disease, and prostate cancer. His physical examination is essentially unremarkable. Lumbar radiographs are within normal limits. What is the most appropriate management for this patient?
Explanation
Question 20
Which of the following increases radiation exposure to patients and personnel during surgery?
Explanation
Question 21
A 78-year-old woman undergoes her third lumbar decompression and fusion from L3 to L5 without complication. On the morning of postoperative day 3, examination reveals painless, flaccid weakness of both lower extremities. She also has an absent bulbocavernous reflex and a mild saddle paresthesia. MRI scans of the lumbar spine are shown in Figures 26a and 26b. What is the most appropriate management at this time?
Explanation
Question 22
Figures 27a through 27c show the radiographs and CT scan of a 27-year-old man who sustained a low-velocity gunshot wound to the neck. He is quadriplegic (ASIA A), hemodynamically stable, and does not have drainage from his wound. After initial resuscitation and stabilization, the cervical spine and spinal cord injuries are best managed by
Explanation
Question 23
Which of the following is a true statement regarding thoracic disk herniations?
Explanation
Question 24
A sentinel event is defined as an unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof. What is the most common sentinel event related to spine surgery?
Explanation
Question 25
What structure is most at risk with anterior penetration of C1 lateral mass screws?
Explanation
Question 26
A 65-year-old man presents with progressive hand clumsiness and gait instability over 1 year. Exam shows a positive Hoffmann sign and hyperreflexia. Preoperative MRI shows T2 hyperintensity and T1 hypointensity in the spinal cord at C4-C5. What is the prognostic significance of these MRI findings?
Explanation
Question 27
A 70-year-old woman undergoes C3-C6 laminectomy and instrumented fusion for cervical spondylotic myelopathy. On postoperative day 2, she develops profound right deltoid and biceps weakness (1/5) with no new sensory deficits. Her lower extremity myelopathic symptoms have improved. What is the most widely accepted pathomechanism for this specific postoperative complication?
Explanation
Question 28
A 62-year-old female presents with severe neurogenic claudication. Standing lateral radiographs demonstrate a grade 1 degenerative spondylolisthesis at L4-L5 with 4 mm of dynamic translation on flexion-extension views. MRI confirms severe central canal stenosis. According to standard board guidelines, what surgical intervention provides the most durable long-term outcome for this patient?
Explanation
Question 29
During the neurologic examination of a patient with suspected cervical myelopathy, tapping the distal brachioradialis tendon results in reflexive finger flexion but an absent normal elbow flexion response. This clinical sign indicates primary pathology at which spinal level?
Explanation
Question 30
A 68-year-old man reports bilateral leg cramping that worsens after walking 2 blocks. The pain is rapidly relieved when he leans forward over a shopping cart but is not relieved simply by standing still upright. He has 2+ palpable pedal pulses. Hypertrophy of which of the following anatomic structures is most likely the primary contributor to his pathology?
Explanation
Question 31
A 55-year-old woman presents with progressive cervical myelopathy.
Radiographs reveal severe multi-level cervical spondylosis from C3 to C6 with a rigid, focal kyphotic deformity of 15 degrees. What is the most appropriate surgical approach?
Explanation
Question 32
A 72-year-old male presents with worsening gait instability, hand clumsiness, and frequent falls. He reports an "electric shock-like" sensation radiating down his spine when he bends his neck forward. What is the name of this clinical sign?
Explanation
Question 33
In a patient with lumbar spinal stenosis, hypertrophy of the superior articular process most commonly compresses which neurologic structure within the lateral recess?
Explanation
Question 34
A 60-year-old Asian male presents with progressive cervical myelopathy. Imaging demonstrates continuous multi-level ossification of the posterior longitudinal ligament (OPLL) from C3-C6. Cervical lordosis is preserved, and the K-line is positive. Which procedure provides adequate decompression while minimizing the risk of a dural tear?
Explanation
Question 35
A 64-year-old woman is undergoing an L3-L5 laminectomy for severe lumbar stenosis. During decompression, an incidental 1.5 cm dural tear occurs with visible CSF egress. What is the most appropriate management?
Explanation
Question 36
A 67-year-old man with known cervical spondylosis presents to the ER after a minor hyperextension injury. He is unable to move his arms but retains functional, albeit weak, motor function in his legs. Perianal sensation is intact. What is the most likely diagnosis?
Explanation
Question 37
Which of the following best describes the natural history of untreated cervical spondylotic myelopathy?
Explanation
Question 38
A 58-year-old man presents with bilateral hand numbness, difficulty buttoning his shirt, and severe neurogenic claudication. Examination shows brisk knee reflexes, absent ankle reflexes, and a positive Hoffmann sign. What is the most appropriate treatment strategy for this presentation of "tandem stenosis"?
Explanation
Question 39
A 68-year-old man presents with progressive gait instability and hand clumsiness over the past 6 months. Physical examination reveals an absent brachioradialis reflex with a hyperactive reflex response causing spontaneous flexion of the fingers. This specific examination finding is due to a compressive lesion at which of the following spinal levels?
Explanation
Question 40
A 72-year-old woman complains of bilateral posterior leg pain that worsens with walking and improves when she rests or leans forward on a shopping cart. Which of the following diagnostic tests best differentiates neurogenic claudication from vascular claudication?
Explanation
Question 41
When counseling a 65-year-old man newly diagnosed with mild cervical spondylotic myelopathy (mJOA score of 16), what is the most accurate description of the natural history of this condition if left untreated?
Explanation
Question 42
A 64-year-old woman with persistent neurogenic claudication has failed 6 months of nonoperative management. Dynamic radiographs and MRI demonstrate a mobile grade I degenerative spondylolisthesis at L4-L5 with severe central canal stenosis. What is the most appropriate surgical treatment?
Explanation
Question 43
A 55-year-old man of East Asian descent presents with progressive cervical myelopathy. Imaging reveals multilevel Ossification of the Posterior Longitudinal Ligament (OPLL). The OPLL mass extends anteriorly, crossing a line connecting the midpoints of the spinal canal at C2 and C7 (K-line negative). What is the most appropriate surgical approach?
Explanation
Question 44
A 64-year-old male presents with progressive clumsiness in his hands and a broad-based gait. Examination shows a positive Hoffmann's sign and bilateral hyperreflexia. MRI of the cervical spine demonstrates multi-level spondylosis with ventral cord compression. Which of the following MRI findings is the strongest predictor of poor neurologic recovery following surgical decompression?
Explanation
Question 45
A 68-year-old female presents with severe neurogenic claudication and an L4-L5 grade I degenerative spondylolisthesis. She has failed 6 months of conservative management. According to the Spine Patient Outcomes Research Trial (SPORT), what is the expected long-term outcome if she chooses surgical decompression and fusion compared to continued nonoperative treatment?
Explanation
Question 46
A 55-year-old male of East Asian descent presents with progressive myelopathy. Imaging reveals continuous Ossification of the Posterior Longitudinal Ligament (OPLL) from C3 to C6. The OPLL mass is noted to cross the K-line on a neutral sagittal radiograph. What is the most appropriate surgical strategy?
Explanation
Question 47
A 72-year-old man complains of bilateral leg pain and fatigue that begins after walking two blocks. The pain is relieved by sitting or leaning over a shopping cart. During a stationary bicycle test, he is able to pedal for 30 minutes without leg pain while leaning forward. Which of the following is the most likely diagnosis?
Explanation
Question 48
During the physical examination of a 60-year-old patient with suspected cervical myelopathy, you tap the brachioradialis tendon near the styloid process of the radius. This elicits spontaneous flexion of the digits without flexion of the elbow. This reflex is most indicative of pathology at which spinal level?
Explanation
Question 49
A 70-year-old woman with multilevel lumbar spinal stenosis presents with an increasingly forward-leaning posture. Radiographs show a marked loss of lumbar lordosis. Which of the following spinopelvic compensatory mechanisms is she most likely utilizing to maintain global sagittal balance?
Explanation
Question 50
A 65-year-old male undergoes a C3-C6 posterior laminectomy and fusion for cervical spondylotic myelopathy. On postoperative day 2, he develops profound weakness in bilateral deltoid and biceps muscles (1/5 strength) but maintains full strength in his hands. What is the most likely etiology of this complication?
Explanation
Question 51
A 65-year-old man presents with mild, non-progressive numbness in his hands and hyperreflexia but normal gait. His mJOA score is 16. What is the most likely natural history of his condition if managed nonoperatively?
Explanation
Question 52
A 55-year-old woman is planning to undergo a posterior cervical laminectomy and fusion for multilevel cervical spondylotic myelopathy. Which of the following preoperative factors is the strongest predictor of a poor functional recovery following surgery?
Explanation
Question 53
A 72-year-old man reports a 1-year history of bilateral buttock and calf pain that occurs after walking two blocks. He notes the pain is relieved when he leans forward on a shopping cart or sits down. His pedal pulses are palpable. Which of the following physical examination findings is most characteristic of his underlying pathology?
Explanation
Question 54
A 68-year-old woman has severe neurogenic claudication and L4-L5 degenerative spondylolisthesis. Flexion-extension radiographs show 4 mm of dynamic translation. She has failed 6 months of nonoperative management. What is the most appropriate surgical treatment?
Explanation
Question 55
Three days after undergoing a C3-C6 posterior laminectomy and fusion for cervical myelopathy, a 62-year-old man develops profound weakness in his bilateral deltoid and biceps muscles. He has no sensory changes, and his lower extremity strength is normal. What is the most likely etiology of this complication?
Explanation
Question 56
A 70-year-old man presents with neurogenic claudication. Sagittal and axial MRI scans demonstrate severe central canal stenosis at L3-L4 and L4-L5.
Which of the following anatomical structures is the primary contributor to dorsal compression of the thecal sac in this condition?
Explanation
Question 57
A 59-year-old man presents with deteriorating handwriting and difficulty buttoning his shirts. On examination, brisk tapping of the distal phalanx of the long finger elicits flexion of the thumb interphalangeal joint. What is this clinical sign, and what does it indicate?
Explanation
Question 58
During an L3-L5 laminectomy for severe spinal stenosis in a 74-year-old woman, an incidental 4-mm dural tear occurs ventrally during removal of hypertrophic ligamentum flavum. Cerebrospinal fluid is noted to be leaking. The tear is inaccessible for direct primary suture repair. What is the most appropriate next step in management?
Explanation
Question 59
A 64-year-old man has severe cervical spondylotic myelopathy due to continuous ossification of the posterior longitudinal ligament (OPLL) from C3 to C6. He has a neutral cervical alignment. Which of the following is the most appropriate surgical approach to decompress the spinal cord?
Explanation
Question 60
A 72-year-old woman with lumbar spinal stenosis reports mild, intermittent neurogenic claudication that does not limit her daily activities. Which of the following is the most appropriate initial management strategy?
Explanation
Question 61
Which of the following characteristics best differentiates degenerative spondylolisthesis from isthmic spondylolisthesis in the lumbar spine?
Explanation
Question 62
In a patient with progressive cervical spondylotic myelopathy, an MRI of the cervical spine reveals focal hyperintensity on T2-weighted images and hypointensity on T1-weighted images within the spinal cord at C4-C5. What does this specific pattern of MRI signal change indicate?
Explanation
Question 63
A 65-year-old woman underwent an L4-S1 posterior decompression and instrumented fusion 5 years ago. She now presents with new-onset L3 radiculopathy and neurogenic claudication. Radiographs reveal a new spondylolisthesis at L3-L4. What is the most significant biomechanical risk factor for this condition?
Explanation
Question 64
A 65-year-old man presents with progressive gait instability, hand clumsiness, and hyperreflexia. Imaging demonstrates multilevel cervical spondylosis from C3-C6 with focal kyphosis of 15 degrees and cord compression. Which of the following surgical approaches is most appropriate?
Explanation
Question 65
A 55-year-old woman with cervical spondylotic myelopathy undergoes a posterior cervical laminectomy and fusion from C3-C6. On postoperative day 2, she develops profound weakness in right shoulder abduction and elbow flexion, with a normal sensory exam and unchanged lower extremity function. What is the most likely etiology of this complication?
Explanation
Question 66
Which of the following MRI findings in a patient with severe cervical spondylotic myelopathy portends the poorest prognosis for neurologic recovery following surgical decompression?
Explanation
Question 67
A 62-year-old man complains of bilaterally radiating leg pain, heaviness, and numbness that worsens after walking two blocks. He notes immediate relief when he leans over his shopping cart at the grocery store. On physical examination, which of the following findings is most reliable for differentiating his condition from peripheral vascular claudication?
Explanation
Question 68
A 72-year-old woman presents with severe neurogenic claudication. Radiographs demonstrate an L4-L5 degenerative spondylolisthesis (Grade 1). MRI confirms severe central canal stenosis. Dynamic flexion-extension radiographs show 4 mm of translation. According to the Spine Patient Outcomes Research Trial (SPORT), what is the expected outcome if she chooses surgical intervention compared to nonoperative management?
Explanation
Question 69
You are evaluating a 68-year-old man with progressive bilateral hand numbness and clumsiness. He demonstrates a positive finger escape sign. During the exam, you briskly flick the distal phalanx of his middle finger downward, resulting in reflexive flexion of his thumb and index finger. What is the name of this clinical sign?
Explanation
Question 70
A 65-year-old man presents with progressive gait instability and loss of fine motor skills. Examination demonstrates a positive Hoffman sign, hyperreflexia, and intrinsic hand muscle atrophy. Lateral radiographs reveal a flexible kyphotic deformity of the cervical spine. MRI demonstrates multi-level cervical stenosis (C3-C6) with spinal cord compression anteriorly. What is the most appropriate surgical intervention?
Explanation
Question 71
A 68-year-old woman presents with severe neurogenic claudication and low back pain. Radiographs reveal a grade 1 degenerative spondylolisthesis at L4-L5 that increases to grade 2 on dynamic flexion views. MRI confirms severe central canal stenosis at L4-L5. She has failed 6 months of comprehensive nonoperative management. What is the most appropriate surgical treatment?
Explanation
Question 72
A 55-year-old man is newly diagnosed with cervical spondylotic myelopathy. Which of the following MRI findings is the most reliable independent predictor of poor neurologic recovery following surgical decompression?
Explanation
Question 73
A 72-year-old man complains of bilateral leg pain that worsens significantly with walking. Which of the following historical factors or examination findings is most specific for neurogenic claudication secondary to lumbar spinal stenosis, as opposed to vascular claudication?
Explanation
Question 74
Three days following a C3-C6 posterior cervical laminectomy and fusion for cervical myelopathy, a 60-year-old patient develops isolated, profound weakness in unilateral shoulder abduction and elbow flexion. Sensation is completely intact, and his preoperative myelopathic symptoms have improved. What is the most likely etiology?
Explanation
Question 75
A 50-year-old man of East Asian descent presents with progressive hand clumsiness and broad-based gait. CT demonstrates a continuous, dense bony mass along the posterior aspect of the C3 to C6 vertebral bodies. MRI shows significant anterior spinal cord compression, but sagittal alignment is lordotic. What is the most appropriate surgical option?
Explanation
Question 76
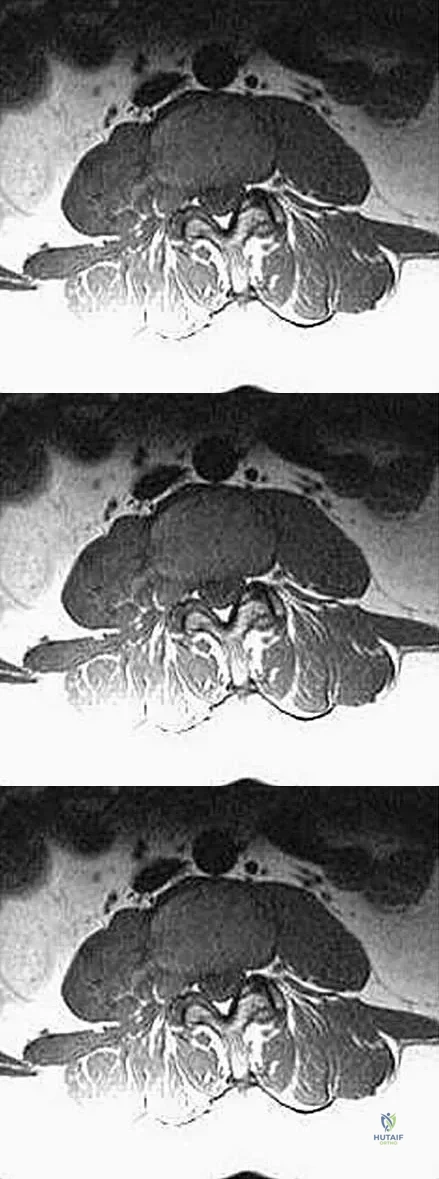
Look at the provided image:
A 67-year-old male presents with progressive lower extremity weakness and neurogenic claudication exacerbated by prolonged standing. Based on standard surgical principles for degenerative lumbar spinal stenosis, if this patient fails non-operative management, what is the primary surgical objective?
Explanation
Question 77
In the pathophysiology of central degenerative lumbar spinal stenosis, which anatomical structure primarily contributes to the narrowing of the central spinal canal from a posterior direction?
Explanation
Question 78
A 70-year-old woman with suspected cervical spondylotic myelopathy is asked to open and close her hands rapidly. She demonstrates spontaneous abduction of her small finger during the exam. What does the abduction of the small finger represent?
Explanation
Question 79
During an L4-L5 laminectomy for severe lumbar spinal stenosis, a 4-mm incidental dural tear occurs dorsally. Cerebrospinal fluid leakage is noted, and the tear is primarily repaired watertight with 4-0 Nurolon sutures. What is the most appropriate next step in management?
Explanation
Question 80
When comparing minimally invasive (MIS) tubular decompression (e.g., unilateral laminotomy for bilateral decompression) to traditional open laminectomy for lumbar spinal stenosis, the MIS approach has been most consistently shown in the literature to result in which of the following?
Explanation
None
