Orthopedic Spine 2026 MCQs: Board Review Questions & Answers (Part 3)

Key Takeaway
We review everything you need to understand about Orthopedic Spine 2026 MCQs: Board Review Questions & Answers (Part 3). Top-rated Orthopedic Spine 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Spine 2026 MCQs: Board Review Questions & Answers (Part 3)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figure 16 shows the radiograph of a 56-year-old man who has neck pain after a rollover accident on his lawnmower. The injury appears to be isolated, and he is neurologically intact. Management of the fracture should consist of
Explanation
Question 2
Degenerative spondylolisthesis of the cervical spine is most commonly seen at which of the following levels?
Explanation
Question 3
Thoracic disk herniations are most frequently found in what area of the spine?
Explanation
Question 4
In a patient who has had low back pain for less than 2 weeks, which of the following findings is an indication for continued observation and symptomatic treatment rather than more aggressive evaluation and/or treatment?
Explanation
Question 5
Radiographs of an 80-year-old woman with back pain reveal a compression fracture. Which of the following imaging studies best evaluates the acuity of the fracture?
Explanation
Question 6
A 24-year-old professional football player underwent surgery for a symptomatic cervical disk herniation with radiculopathy 9 months ago. A current radiograph is shown in Figure 17. He has normal neurologic findings, no pain, and full range of motion. A CT scan shows a solid fusion. When can he expect to return to play?
Explanation
Question 7
When treating thoracic disk herniations, which of the following surgical approaches has the highest reported rate of neurologic complications?
Explanation
Question 8
When harvesting iliac crest bone graft during a posterior spinal decompression and fusion, injury to what structure can result in painful neuromas or numbness over the skin of the buttocks?
Explanation
Question 9
A 42 year-old-woman who underwent surgery for lumbar scoliosis 2 years ago now has fixed sagittal plane imbalance and severe back pain. Which of the following is considered a contraindication to isolated pedicle subtraction osteotomy for the treatment of iatrogenic flatback syndrome in this patient?
Explanation
Question 10
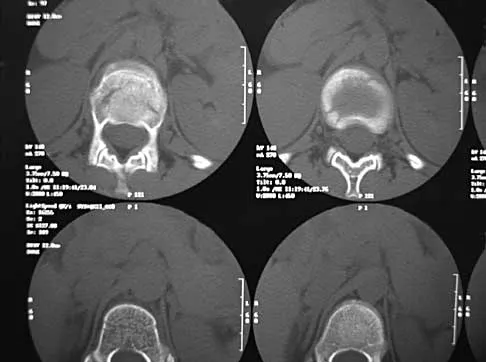
A 42-year-old man sustained a burst fracture at L2 in a motor vehicle accident. Examination reveals that he is neurologically intact. Figure 18 shows a cross-sectional CT scan through the fracture. If the fracture is managed nonsurgically for the next 2 years, the retained fragments can be expected to
Explanation
Question 11
A 50-year-old man reports the onset of back pain and incapacitating pain radiating down his left leg posterolaterally and into the first dorsal web space of his foot 1 day after doing some yard work. He denies any history of trauma. Examination reveals ipsilateral extensor hallucis longus weakness. MRI scans are shown in Figures 19a through 19c. What nerve root is affected?
Explanation
Question 12
Which of the following pharmacologic agents is most likely to adversely affect the success rate of bony union after lumbar arthrodesis?
Explanation
Question 13
A 69-year-old woman is seen in the emergency department with a bilateral C5-6 facet dislocation and complete quadriplegia after falling down a flight of stairs. After initial evaluation and treatment by the trauma service, she is moved to the intensive care unit. Examination reveals a blood pressure of 90/50 mm/Hg, a pulse rate of 50/min, a respiration rate of 12/min, and urine output of 1 mL/kg/h. Her hemodynamic status should be addressed by
Explanation
Question 14
What region of the spine is most susceptible to changes in the vascular supply to the spinal cord during an anterior approach?
Explanation
Question 15
What is the most common presenting sign or symptom in an adult with lumbar pyogenic infection?
Explanation
Question 16
The natural history of cervical spondylolytic myelopathy is best described as
Explanation
Question 17
Figures 20a and 20b show lateral and AP radiographs of a 49-year-old man who sustained a gunshot wound through the left shoulder. He reports neck pain and examination reveals weakness in all four extremities. What is the priority of evaluation?
Explanation
Question 18
A 35-year-old woman undergoes an L4-5 anterior fusion via a left retroperitoneal approach. Postoperative examination reveals that her right foot is cool and pale. Her neurologic examination is normal, and her pedal pulses are asymmetric. What is the most likely reason for the right foot finding?
Explanation
Question 19
What type of thoracolumbar spinal injury is associated with an increased risk of neurologic deterioration following admission to the hospital?
Explanation
Question 20
A 30-year-old man has had a 3-day history of severe, incapacitating lower back pain without radiation. He reports improvement with rest. He denies any history of trauma, has no constitutional symptoms, and his neurologic examination is normal. What is the best course of action?
Explanation
Question 21
Which of the following patient factors is associated with recurrent radicular pain following lumbar diskectomy for sciatica?
Explanation
Question 22
Figure 21 shows the tomogram of a 26-year-old woman who sustained an axial load injury to her neck in a fall off a horse. What ligament is injured?
Explanation
Question 23
Based on the findings shown in Figures 22a and 22b, corrective surgery to obtain maximal safe correction and optimal instrumentation fixation should be performed at which of the following locations?
Explanation
Question 24
A 65-year-old woman has significant neck pain after falling and striking her head. A radiograph and sagittal CT scan are shown in Figures 23a and 23b. What is the most likely diagnosis?
Explanation
Question 25
Immediately after undergoing lumbar instrumentation, a patient reports severe right leg pain and has 4+/5 weakness. Figure 24 shows an axial CT scan of L5. Exploratory surgery will most likely reveal
Explanation
Question 26
A 65-year-old woman presents with progressive low back pain and an inability to stand up straight. Standing full-length spine radiographs reveal a pelvic incidence (PI) of 60°, lumbar lordosis (LL) of 20°, pelvic tilt (PT) of 35°, and sagittal vertical axis (SVA) of +12 cm. What is the minimum recommended degree of lumbar lordosis restoration required to optimize her post-operative clinical outcome?
Explanation
Question 27
A 65-year-old man presents with progressive gait imbalance and loss of fine motor skills. Examination reveals hyperreflexia and a positive Babinski sign. MRI of the cervical spine demonstrates multi-level stenosis from C3 to C6 due to ossification of the posterior longitudinal ligament (OPLL). A line drawn from the mid-point of the spinal canal at C2 to the mid-point at C7 (K-line) on a neutral sagittal image shows that the OPLL mass crosses anterior to posterior over this line (K-line negative). Which of the following surgical approaches is most strongly indicated?
Explanation
Question 28
A 35-year-old male falls from a 15-foot ladder and sustains an L1 burst fracture. His neurological examination is completely normal (ASIA E). A CT scan shows 45% canal compromise and 20 degrees of local kyphosis. An MRI confirms an intact posterior ligamentous complex (PLC). According to the Thoracolumbar Injury Classification and Severity Score (TLICS), what is the most appropriate management?
Explanation
Question 29
A 55-year-old diabetic male presents with 2 weeks of worsening mid-back pain, low-grade fevers, and new-onset lower extremity weakness (motor strength 3/5 bilaterally). He also reports urinary retention. An MRI reveals a large ventral epidural abscess at T6-T8 with severe spinal cord compression. Broad-spectrum intravenous antibiotics are initiated. What is the next best step in management?
Explanation
Question 30
A 70-year-old man with a known history of severe ankylosing spondylitis presents to the emergency department after a minor low-speed motor vehicle collision. He reports new-onset severe neck pain but has no neurological deficits. Initial plain radiographs of the cervical spine are obscured by cervicothoracic kyphosis and osteopenia, making them difficult to interpret. What is the most appropriate next step in management?
Explanation
Question 31
A 14-year-old female gymnast complains of persistent mechanical low back pain for 6 months. Radiographs demonstrate a Grade II L5-S1 isthmic spondylolisthesis. Non-operative management, including bracing, physical therapy, and activity modification, has failed. She is now scheduled for an in situ posterolateral L5-S1 fusion. Which of the following slip parameters is most associated with a high risk of progression and nonunion?
Explanation
Question 32
An 80-year-old woman presents with acute, severe localized midthoracic back pain following a minor lifting incident 1 week ago. Neurologic exam is completely normal. Radiographs demonstrate an acute T8 osteoporotic compression fracture with a 20% loss of anterior height. What is the recommended initial management?
Explanation
Question 33
A 60-year-old woman with a 20-year history of severe rheumatoid arthritis presents with neck pain and occipital headaches. Lateral cervical spine radiographs in flexion and extension show an anterior atlantodens interval (ADI) of 8 mm. Which of the following is the most critical radiographic parameter to measure to determine the risk of impending neurologic injury?
Explanation
Question 34
During a routine L4-L5 lumbar microdiscectomy for a herniated disc, an incidental durotomy is encountered. A primary water-tight repair is successfully performed with 4-0 Nurolon. A Valsalva maneuver confirms no further cerebrospinal fluid (CSF) leak. What is the most appropriate post-operative management strategy regarding patient mobilization?
Explanation
Question 35
Which of the following is considered the strongest risk factor for nonunion of a Type II odontoid fracture treated non-operatively with rigid cervical immobilization?
Explanation
Question 36
Figure 1 shows the lateral radiograph of a 30-year-old man who sustained a whiplash-type injury in a motor vehicle collision. He presents with neck pain and weakness in wrist extension, but normal triceps strength. The imaging demonstrates a unilateral facet dislocation at C6-C7. Which nerve root is most likely affected, and what is the typical biomechanical mechanism of this injury?

Explanation
Question 37
A 65-year-old woman presents with severe mechanical back pain and an inability to stand upright. Standing full-length spine radiographs reveal a pelvic incidence (PI) of 60 degrees and a sacral slope (SS) of 20 degrees. What is her pelvic tilt (PT), and what is the optimal target for her postoperative lumbar lordosis (LL) to restore sagittal balance?
Explanation
Question 38
A 55-year-old diabetic male presents with 2 weeks of worsening back pain, fevers, and recent onset of bilateral lower extremity weakness (3/5) and urinary retention. MRI (Figure 2) shows an extensive ventral epidural abscess from L2 to L4 causing severe canal stenosis. What is the most appropriate next step in management?

Explanation
Question 39
A 62-year-old man of East Asian descent presents with clumsiness in his hands, fine motor difficulty, and a wide-based gait. Lateral radiograph and CT (Figure 3) demonstrate continuous linear ossification along the posterior aspect of the C3-C6 vertebral bodies, with a local kyphotic angle of 18 degrees. Which of the following is the most likely diagnosis, and what surgical approach is generally favored given his alignment?

Explanation
Question 40
An 82-year-old woman sustains a ground-level fall and complains of severe neck pain. CT scan (Figure 4) reveals a Type II odontoid fracture with 2 mm of posterior displacement. She is neurologically intact. Which of the following treatments has the highest risk of morbidity and mortality in this specific patient demographic?

Explanation
Question 41
A 58-year-old female presents with severe neurogenic claudication secondary to L4-L5 degenerative spondylolisthesis. Preoperative dynamic radiographs show 4 mm of translation on flexion-extension. Based on the Spine Patient Outcomes Research Trial (SPORT) study on degenerative spondylolisthesis, how do the outcomes of surgical management compare to nonoperative management at the 4-year follow-up?
Explanation
Question 42
A 40-year-old male falls from a height of 10 feet. Neurological examination is completely normal (Grade E). CT of the spine (Figure 5) shows an L1 burst fracture with 40% loss of anterior body height, 20 degrees of kyphosis, and 30% canal compromise. MRI demonstrates an intact posterior ligamentous complex (PLC). Using the Thoracolumbar Injury Classification and Severity (TLICS) score, what is this patient's score and the recommended management?

Explanation
Question 43
A 60-year-old woman with a history of renal cell carcinoma presents with progressive back pain. MRI shows a metastatic lesion in the T8 vertebral body with high-grade epidural spinal cord compression. She has 4/5 strength in her lower extremities. Her overall life expectancy is estimated to be greater than 1 year. According to the NOMS (Neurologic, Oncologic, Mechanical, Systemic) framework, what is the most appropriate management for this radioresistant tumor?
Explanation
Question 44
A 13-year-old premenarchal female presents with a right thoracic curve. She has not had her first menstrual period and is Risser stage 0. Standing PA radiograph shows a Cobb angle of 35 degrees. According to the Bracing in Adolescent Idiopathic Scoliosis Trial (BRAIST), what is the most appropriate management for this patient?
Explanation
Question 45
A 68-year-old male complains of bilateral calf, thigh, and buttock pain that worsens with ambulation. Which of the following clinical features is most indicative of neurogenic claudication (secondary to lumbar spinal stenosis) rather than vascular claudication?
Explanation
Question 46
A 60-year-old man with a long-standing history of ankylosing spondylitis sustains a cervical spine fracture after a ground-level fall. Upon presentation, he complains of severe neck pain but remains neurologically intact. Radiographs and a CT scan reveal a displaced fracture extending through the C5-C6 disc space and the posterior elements. What is the most appropriate definitive management for this patient?
Explanation
Question 47
A 65-year-old man presents with chronic back pain and bilateral leg heaviness that worsens with walking and is relieved by leaning forward. MRI demonstrates severe L4-L5 spinal stenosis without spondylolisthesis. He is scheduled for an L4-L5 decompressive laminectomy. Which of the following intraoperative factors is the most significant risk factor for the development of postoperative iatrogenic spondylolisthesis requiring secondary fusion?
Explanation
Question 48
A 35-year-old man falls from a height of 15 feet and sustains a T12 thoracolumbar burst fracture. Imaging reveals a 40% loss of anterior vertebral body height, 20% retropulsion of bone into the spinal canal, and an intact posterior ligamentous complex (PLC). Physical examination confirms he is completely neurologically intact. What is the most appropriate management?

Explanation
Question 49
A 24-year-old man is involved in a high-speed motor vehicle collision. A CT scan of the cervical spine reveals a traumatic spondylolisthesis of the axis (Hangman's fracture). According to the Levine and Edwards classification, which of the following radiographic findings distinguishes a Type II Hangman's fracture from a Type I fracture?
Explanation
Question 50
During an anterior cervical discectomy and fusion (ACDF), meticulous dissection is required to avoid injury to the recurrent laryngeal nerve (RLN). Which of the following statements most accurately describes the anatomical characteristics and surgical implications of the RLN?

Explanation
Question 51
A 68-year-old woman presents with severe low back pain and a progressive forward-leaning posture. Standing full-length spinal radiographs reveal a pelvic incidence (PI) of 60 degrees, a pelvic tilt (PT) of 35 degrees, and a lumbar lordosis (LL) of 25 degrees. To optimally correct her sagittal imbalance during surgical reconstruction, what is the primary realignment goal regarding these spinopelvic parameters?
Explanation
Question 52
Which of the following radiographic parameters is considered the gold standard for quantifying global sagittal alignment on a standing 36-inch lateral radiograph?

Explanation
Question 53
A 54-year-old man with a history of intravenous drug use presents with severe midthoracic back pain, subjective fevers, and progressive lower extremity weakness over 48 hours. Physical examination reveals 3/5 motor strength in both legs, diminished sensation below T10, and a palpable distended bladder. MRI demonstrates a large dorsal epidural abscess spanning T8-T11 with severe cord compression. What is the most appropriate next step in management?
Explanation
Question 54
A 14-year-old female gymnast presents with a 1-year history of unrelenting low back pain exacerbated by extension maneuvers. Radiographs demonstrate a Grade II isthmic spondylolisthesis at L5-S1. She has failed 6 months of comprehensive conservative management, including Boston bracing, physical therapy, and strict activity modification. Which of the following is the most appropriate surgical intervention?

Explanation
Question 55
A 65-year-old man with known preexisting cervical spondylosis presents to the emergency department after sustaining a hyperextension injury to his neck in a rear-end motor vehicle collision. He exhibits significant weakness and a burning sensation in his upper extremities, but retains 4/5 strength in his lower extremities. His bowel and bladder functions are intact. Which of the following best explains the anatomical basis for this specific neurologic deficit?
Explanation
Question 56
An 82-year-old man presents with neck pain after a low-energy fall from a standing height. Neurologic examination is normal. Radiographs and CT scan demonstrate a Type II odontoid fracture with 2 mm of posterior displacement. In considering non-operative management options, which of the following immobilization methods is associated with the highest rate of morbidity and mortality in this age group?
Explanation
Question 57
A 45-year-old man presents with an acute onset of severe right leg pain. Physical examination reveals weakness in the right extensor hallucis longus (EHL) muscle (3/5 strength) and decreased pinprick sensation over the dorsal aspect of the first web space of the right foot. His patellar and Achilles reflexes are symmetric and intact. Which of the following disc herniations is the most likely cause of this patient's clinical presentation?
Explanation
Question 58
In the preoperative planning for a 62-year-old woman undergoing corrective surgery for adult degenerative scoliosis and sagittal imbalance, analyzing spino-pelvic parameters is critical. To minimize the risk of mechanical failure, proximal junctional kyphosis, and adjacent segment disease, the postoperative lumbar lordosis (LL) should ideally be matched to the patient's pelvic incidence (PI) within what range?
Explanation
Question 59
A 66-year-old man presents with progressive clumsiness in his hands, difficulty buttoning his shirt, and a wide-based gait. Physical examination demonstrates a positive Hoffmann sign bilaterally. An MRI of the cervical spine is performed to evaluate for cervical spondylotic myelopathy. Which of the following specific MRI findings is associated with the poorest prognosis for neurologic recovery following surgical decompression?
Explanation
Question 60
A 22-year-old restrained passenger is involved in a high-speed motor vehicle collision. He reports severe back pain.
Figure 6 shows a lateral radiograph of the thoracolumbar spine revealing a flexion-distraction injury (Chance fracture) at L2. What is the most commonly associated concomitant injury with this specific fracture pattern?
Explanation
Question 61
A 60-year-old man with a long-standing history of Ankylosing Spondylitis is brought to the emergency department after a minor fall at home. He complains of new-onset lower cervical neck pain. Neurologic examination is unremarkable. Standard orthogonal plain radiographs of the cervical spine are interpreted by the on-call radiologist as showing 'no acute fracture, typical bamboo spine changes'. What is the most appropriate next step in management?
Explanation
Question 62
A 12-year-old premenarchal girl presents with an asymmetric Adam's forward bending test. Standing scoliosis radiographs reveal a right thoracic curve measuring 32 degrees with an apex at T8. Her Risser stage is 0, and the tri-radiate cartilages are open. What is the most appropriate management for this patient?
Explanation
Question 63
A 35-year-old woman presents to the emergency department with acute onset severe lower back pain, bilateral lower extremity sciatica, perineal numbness, and urinary retention. Bladder ultrasound reveals a post-void residual of 500 mL. MRI confirms a massive L4-L5 central disc herniation causing severe cauda equina compression. According to current literature, surgical decompression should ideally be performed within what time frame from the onset of autonomic symptoms to maximize the probability of bladder function recovery?
Explanation
Question 64
A 68-year-old woman with advanced rheumatoid arthritis is being evaluated preoperatively before a total knee arthroplasty. She denies any radicular pain, weakness, or changes in bowel/bladder function. Flexion-extension radiographs of the cervical spine reveal atlantoaxial instability. Which of the following radiographic findings represents an absolute indication for prophylactic posterior C1-C2 fusion prior to her elective knee surgery?
Explanation
Question 65
A 60-year-old man presents with progressive cervical myelopathy secondary to multi-level Ossification of the Posterior Longitudinal Ligament (OPLL). When determining the surgical approach (anterior vs. posterior), the 'K-line' is evaluated on the lateral cervical radiograph. Which of the following scenarios is considered a definitive contraindication to performing a stand-alone posterior cervical laminoplasty for this patient?
Explanation
Question 66
Figure 22 shows the imaging of an 82-year-old man who fell from a standing height and presents with severe neck pain. He is neurologically intact. If this injury is treated nonoperatively, which of the following factors is most strongly associated with the development of a nonunion?

Explanation
Question 67
A 65-year-old man presents with progressive hand clumsiness, difficulty buttoning his shirts, and frequent tripping. On examination, flicking the volar aspect of the distal phalanx of his middle finger results in reflexive flexion of his ipsilateral thumb and index finger. This physical examination finding indicates compression of which of the following structures?
Explanation
Question 68
A 35-year-old woman is involved in a motor vehicle collision and sustains a burst fracture of L1. Her neurological examination demonstrates full strength and normal sensation in her bilateral lower extremities (ASIA E). An MRI is obtained which definitively demonstrates disruption of the posterior ligamentous complex (PLC). Based on the Thoracolumbar Injury Classification and Severity (TLICS) score, what is the most appropriate management?
Explanation
Question 69
Figure 4 demonstrates the standing full-length spine radiograph of a 68-year-old woman presenting with severe lower back pain, forward stooping, and early satiety. When planning corrective surgery for adult spinal deformity, which of the following represents the optimal goal for the relationship between Pelvic Incidence (PI) and Lumbar Lordosis (LL)?
Explanation
Question 70
Figure 11 shows a lateral radiograph of a 14-year-old female gymnast with chronic, mechanical low back pain. Radiographs reveal a Grade II isthmic spondylolisthesis at L5-S1. She has failed 6 months of physical therapy, activity modification, and bracing. Which of the following is the most appropriate surgical treatment?

Explanation
Question 71
Figure 15 shows the cervical spine radiograph of a 52-year-old man with a long history of ankylosing spondylitis who presents with neck pain after a minor fall. He is neurologically intact on presentation. Which of the following statements is true regarding this patient's condition?

Explanation
Question 72
In evaluating a patient with metastatic disease to the thoracic spine, the Spinal Instability Neoplastic Score (SINS) is utilized to guide referral for surgical stabilization. Which of the following radiographic or clinical findings contributes the highest number of points to the SINS score?
Explanation
Question 73
Figure 8 demonstrates the sagittal CT scan of a 55-year-old man of Japanese descent who presents with progressive gait instability, hyperreflexia, and a positive Hoffman sign. He is diagnosed with Ossification of the Posterior Longitudinal Ligament (OPLL). If a posterior approach (e.g., laminoplasty) is chosen for definitive management, which of the following factors provides the primary anatomic rationale for this surgical selection?

Explanation
Question 74
A 70-year-old man with known severe cervical spondylosis presents after a hyperextension injury to his neck resulting from a fall down stairs. On examination, he has profound weakness in his upper extremities, particularly the intrinsic muscles of the hands, but is able to ambulate with minimal assistance. He reports patchy sensory loss in his arms and has urinary retention. Which of the following best describes the pathophysiologic mechanism of this specific neurologic deficit?
Explanation
Question 75
Figure 13 shows the axial MRI of a 42-year-old man presenting with severe bilateral leg pain, saddle anesthesia, and acute urinary retention. He is taken for emergent surgical decompression. Which of the following factors is most strongly associated with a poor prognosis for the return of normal bladder function?

Explanation
Question 76
A 60-year-old Asian man presents with progressive clumsiness in his hands, broad-based gait, and bilateral hyperreflexia. A lateral radiograph and sagittal CT of the cervical spine demonstrate continuous ossification of the posterior longitudinal ligament (OPLL) from C3 to C6. The cervical spine has maintained a lordotic alignment, and the K-line is positive. What is the most appropriate surgical intervention?
Explanation
Question 77
Figure 10 shows the imaging of a 35-year-old woman who fell from a height of 10 feet. She has severe midline back pain but is neurologically entirely intact. CT and MRI of the thoracolumbar spine show an L1 burst fracture with 15 degrees of local kyphosis and 30% canal compromise. The posterior ligamentous complex (PLC) is intact on MRI STIR sequences. Based on the Thoracolumbar Injury Classification and Severity (TLICS) score, what is the most appropriate management?

Explanation
Question 78
A 65-year-old woman with a history of hypertension and diabetes presents with 1 year of neurogenic claudication and lower back pain. Imaging confirms an L4-L5 grade I degenerative spondylolisthesis with severe central canal stenosis. She has failed 6 months of structured physical therapy, NSAIDs, and epidural steroid injections. According to the Spine Patient Outcomes Research Trial (SPORT) for degenerative spondylolisthesis, what outcome is expected if she chooses surgical intervention compared to continued non-operative management?
Explanation
Question 79
A 25-year-old man presents to the trauma bay after a shallow water diving accident. An open-mouth odontoid radiograph demonstrates a lateral mass displacement of C1 on C2 totaling 8 mm. Subsequent MRI confirms a mid-substance rupture of the transverse atlantal ligament (TAL). He is neurologically intact. What is the most appropriate definitive management?
Explanation
Question 80
Figure 6 relates to a 62-year-old man with a known history of advanced ankylosing spondylitis who presents with new-onset, severe neck pain following a minor ground-level fall. He is neurologically intact. Initial lateral cervical spine radiographs in the emergency department are read as "normal with extensive bridging syndesmophytes." What is the most appropriate next step in his management?
Explanation
Question 81
An 85-year-old woman with severe chronic obstructive pulmonary disease, congestive heart failure, and osteoporosis sustains a Type II odontoid fracture with 3 mm of posterior displacement after a mechanical fall. She complains of neck pain but has no neurological deficits. What is the most appropriate initial management for this patient?
Explanation
Question 82
A 30-year-old man sustains a traumatic spondylolisthesis of the axis (Hangman's fracture) following a high-speed motor vehicle collision. Lateral radiographs demonstrate significant angulation at the C2-C3 interspace with minimal translation. When longitudinal cervical traction is applied in the emergency department, the C2-C3 angulation paradoxically increases. Based on the Levine and Edwards classification, what is the most appropriate definitive management for this specific injury pattern?
Explanation
Question 83
A 52-year-old man with a history of intravenous drug use presents with 2 weeks of worsening lower back pain and low-grade fever. Neurological examination reveals full 5/5 strength in all lower extremity muscle groups, normal reflexes, intact sensation, and normal rectal tone. Laboratory studies show a WBC of 14,000/µL, ESR of 85 mm/hr, and CRP of 120 mg/L. MRI with contrast reveals an epidural abscess from L3 to L5 causing moderate thecal sac compression. Blood cultures return positive for methicillin-sensitive Staphylococcus aureus (MSSA). What is the most appropriate initial management?
Explanation
Question 84
A 68-year-old man underwent an L3-L5 posterior spinal decompression and instrumented fusion 3 years ago. He now presents with severe low back pain and radiculopathy corresponding to the L2-L3 level. Radiographs reveal progressive stenosis and listhesis at L2-L3. Which of the following factors has been most significantly correlated with an increased risk of developing adjacent segment disease (ASD) following a lumbar fusion?
Explanation
Question 85
A 45-year-old woman is evaluated in the emergency department for severe low back pain, bilateral lower extremity radicular pain, saddle anesthesia, and new-onset acute urinary retention. She notes the urinary retention began approximately 12 hours ago. MRI reveals a massive extruded disc herniation at L4-L5 severely compressing the cauda equina. Regarding surgical intervention for Cauda Equina Syndrome with urinary retention (CES-R), which of the following statements most accurately reflects current evidence on timing and outcomes?
Explanation
Question 86
A 78-year-old male with severe osteoporosis presents to the emergency department after a ground-level fall, reporting severe upper neck pain. He is neurologically intact. Imaging confirms a Type II odontoid fracture. If nonoperative management with a rigid cervical collar is chosen, which of the following radiographic findings is the most significant predictor of subsequent nonunion?
Explanation
Question 87
A 60-year-old male with a history of intravenous drug use presents with 48 hours of progressive bilateral lower extremity weakness, sensory loss below the umbilicus, and severe midthoracic back pain. His temperature is 38.8°C (101.8°F). MRI with contrast reveals a large, peripherally enhancing posterior epidural collection extending from T4 to T8 with severe spinal cord compression. Which of the following is the most appropriate management?
Explanation
Question 88
A 35-year-old male falls 10 feet from a ladder and sustains an L1 burst fracture. He is neurologically intact. MRI demonstrates an intact posterior ligamentous complex (PLC). Based on the Thoracolumbar Injury Classification and Severity (TLICS) score, what is his total score and the generally recommended treatment?
Explanation
Question 89
A 58-year-old male presents with progressively worsening manual dexterity, broad-based gait, and hyperreflexia in the lower extremities. MRI of the cervical spine demonstrates severe central canal stenosis at C4-C5 and C5-C6 with spinal cord signal changes. Which of the following MRI signal characteristics is associated with the poorest prognosis for neurologic recovery following surgical decompression?
Explanation
Question 90
A 16-year-old female gymnast complains of 6 months of persistent lower back pain that is worsened with spinal extension. She has failed physical therapy and bracing. Upright lateral radiographs demonstrate a Grade I isthmic spondylolisthesis at L5-S1. What is the most appropriate surgical intervention?
Explanation
Question 91
A 68-year-old male with a 30-year history of ankylosing spondylitis sustains a low-energy fall and presents with severe lower cervical pain. He is initially neurologically intact. CT imaging confirms a displaced, transdiscal extension-type fracture at C6-C7. Within hours of admission, he develops progressive quadriplegia. What is the most likely cause of his delayed neurologic deterioration?
Explanation
Question 92
A 65-year-old female presents with severe mechanical lower back pain, early satiety, and a flexed posture. Radiographs reveal a severe degenerative flatback deformity. Her measured pelvic incidence (PI) is 58 degrees. To achieve optimal spinopelvic alignment and clinical outcomes postoperatively, what should her target lumbar lordosis (LL) ideally be?
Explanation
Question 93
A 45-year-old male presents with acute onset of severe right anterior thigh pain and weakness in knee extension. Examination reveals an absent right patellar reflex and sensory diminished over the medial aspect of the right lower leg. MRI of the lumbar spine reveals a far lateral (extraforaminal) disc herniation at the L4-L5 level on the right. Which nerve root is most likely compressed?
Explanation
Question 94
A 55-year-old female with long-standing, poorly controlled rheumatoid arthritis complains of occipital headache and "electric shock" sensations radiating down her arms when she flexes her neck. Flexion-extension radiographs demonstrate atlantoaxial subluxation. Which of the following radiographic measurements indicates the highest risk for impending neurologic deficit and serves as a strong indication for surgical stabilization?
Explanation
Question 95
A 42-year-old male presents to the emergency department with severe lower back pain and bilateral radicular leg pain. He reports the onset of urinary incontinence starting 8 hours ago. Examination reveals complete perineal anesthesia (saddle anesthesia) and absent anal sphincter tone. MRI confirms a massive L4-L5 central disc extrusion. Following emergent decompression, which of the following is the most reliable predictor of poor postoperative bladder function recovery?
Explanation
Question 96
Figure 24 shows the lateral radiograph of an 84-year-old man who sustained a ground-level fall. He complains of high neck pain but is neurologically intact. CT scan confirms a Type II odontoid fracture with 1 mm of posterior displacement. If non-operative management is selected for this patient, which of the following orthoses is associated with the highest mortality rate in this specific demographic?
Explanation
Question 97
A 65-year-old woman presents with progressive low back pain and difficulty standing upright. Standing full-length lateral spine radiographs reveal a Pelvic Incidence (PI) of 60 degrees and a Pelvic Tilt (PT) of 35 degrees. What is her Sacral Slope (SS), and what does this PT value indicate about her compensatory mechanism?
Explanation
Question 98
Figure 17 shows imaging of a 55-year-old man of East Asian descent presenting with progressive clumsiness in his hands and a wide-based gait. Imaging demonstrates Ossification of the Posterior Longitudinal Ligament (OPLL) from C3 to C6 with a K-line that is negative. Which of the following is the most appropriate surgical strategy?
Explanation
Question 99
A 35-year-old construction worker falls from a height of 15 feet. Neurological examination reveals 3/5 strength in ankle dorsiflexion and EHL bilaterally, with intact bowel and bladder function. CT scan of the thoracolumbar spine demonstrates an L1 burst fracture. MRI reveals complete disruption of the posterior interspinous ligaments and ligamentum flavum. According to the Thoracolumbar Injury Classification and Severity (TLICS) score, what is his total score and the recommended treatment?
Explanation
Question 100
Figure 6 shows the sagittal T2-weighted MRI of a 60-year-old diabetic patient presenting with severe back pain, fever, and progressive bilateral leg weakness over the past 24 hours. Laboratory studies show an ESR of 85 mm/hr and CRP of 120 mg/L. MRI confirms a ventral epidural abscess at L2-L4. Blood cultures are drawn in the emergency department. What is the most appropriate next step in management?
Explanation
None
