Orthopedic Spine 2026 MCQs: Board Review Questions & Answers (Part 1)

Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Orthopedic Spine 2026 MCQs: Board Review Questions & Answers (Part 1). Top-rated Orthopedic Spine 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Spine 2026 MCQs: Board Review Questions & Answers (Part 1)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figures 1a and 1b show the sagittal T2- and T1-weighted MRI scans of a 25-year-old intravenous drug abuser who has low back pain that is increasing in intensity. Laboratory studies show a WBC count of 10,000/mm3 and an erythrocyte sedimentation rate of 80 mm/h. Blood culture is negative. Initial management consist of
Explanation
Question 2
A 27-year-old man sustained a gunshot wound to the lumbar spine and undergoes an exploratory laparotomy. An injury to the cecum is identified and treated. Management should now include
Explanation
Question 3
A 68-year-old man reports a 1-year history of debilitating neck pain without neurologic symptoms. History reveals a C5-6 anterior diskectomy and bone grafting 10 years ago that provided good relief of arm and neck pain. Radiographs show evidence of fibrous union at C5-6, spondylotic disk narrowing at C4-5 and C6-7, and a fixed 2-mm subluxation at C3-4. Examination reveals cervical stiffness and discomfort at the extremes of movement. His neurologic examination is normal. Treatment should now consist of
Explanation
Question 4
Which of the following is considered the lowest level that a standard thoracolumbosacral orthosis (TLSO) can immobilize?
Explanation
Question 5
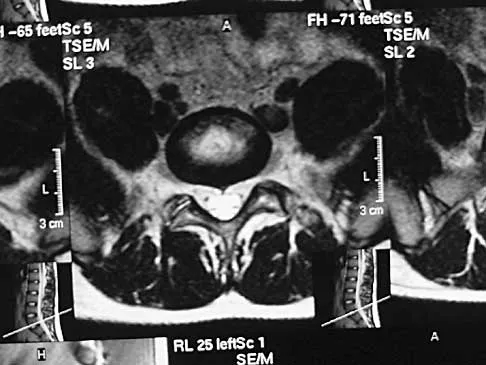
A 65-year-old man with ankylosing spondylitis has neck pain after falling back over his lawnmower, striking his thoracic spine, and forcing his neck into extension. Examination reveals subtle weakness of the intrinsics and finger flexors at approximately 4+/5. Initial management consists of immobilization in a rigid collar, and placing his head in the anatomic position. Radiographs reveal a subtle extension fracture of the lower cervical spine. Approximately 6 hours after the injury, he reports increasing paresthesias in his upper and lower extremities, and examination now shows his intrinsics are 2/5, finger flexors are 3/5, and his triceps are now weak at 4/5 on manual motor testing. In addition, his lower extremities now show weakness in both dorsal and plantar flexion of the ankle in the range of 4/5. Repeat radiographs appear unchanged. An MRI scan is shown in Figure 2. Management should now consist of
Explanation
Question 6
Figures 3a and 3b show the MRI scans of a patient with neck pain. What is the most likely diagnosis?
Explanation
Question 7
A Trendelenburg gait is most likely to be seen in association with
Explanation
Question 8
An otherwise healthy 70-year-old man has back and bilateral leg pain in an L5 distribution that is aggravated by standing more than 10 minutes or walking more than 100 feet. He has to sit to get relief. Neurologic and pulse examinations are normal. A radiograph and MRI scan are shown in Figures 4a and 4b. Treatment should consist of
Explanation
Question 9
Figures 5a and 5b show the radiograph and MRI scan of a patient who has severe mechanical neck pain but no neurologic problems. Biopsy and work-up show the lesion to be a solitary plasmacytoma. Treatment should consist of
Explanation
Question 10
A 71-year-old woman undergoes a posterior lumbar decompression and fusion from L4-S1. Thirty-six hours after the procedure, she reports severe right-sided chest pain and shortness of breath. Doppler ultrasound reveals a clot proximal to the knee within the femoral vein. A large pulmonary embolus is confirmed by CT angiography. The next most appropriate step in management should consist of
Explanation
Question 11
Figure 6 shows the lateral radiograph of a 22-year-old woman who has painful Scheuermanns's kyphosis in the middle and lower thoracic spine. When planning surgical correction using instrumentation, the distal aspect of the instrumentation should ideally extend to the
Explanation
Question 12
Figure 7 shows the radiograph of a 64-year-old man who has neck pain and weakness of the upper and lower extremities following a motor vehicle accident. Examination reveals 3/5 quadriceps and 4/5 hip flexors but no ankle dorsiflexion or plantar flexion. His intrinsics are 1/5, with finger flexors of 3/5. He is awake, alert, and cooperative. Management should consist of
Explanation
Question 13
What is the recommended insertion torque for halo pins in adults?
Explanation
Question 14
A 55-year-old woman with a history of untreated idiopathic scoliosis has had neurogenic claudication for the past several months. MRI reveals spinal stenosis at L2-L3, L3-L4, and L4-L5. Radiographs show a 45-degree lumbar curve from T10 to L4, with a degenerative spondylolisthesis at L4-L5. Laminectomy at the stenotic levels and stabilization of the deformity are planned. Which of the following is NOT considered an absolute indication for extending the fusion to the sacrum, rather than stopping at L5?
Explanation
Question 15
Which of the following findings is considered a contraindication for posterior decompression (with or without fusion) for myelopathy?
Explanation
Question 16
A patient reports progessive bilateral hand clumsiness and ataxia. Examination reveals a positive Hoffmann's sign and intrinsic atrophy. MRI reveals multilevel cervical spondylosis, and lateral flexion and extension radiographs show cervical kyphosis in the neutral position, with restoration of lordosis on extension. Which of the following procedures is most likely to result in poor long-term results?
Explanation
Question 17
A 45-year-old man seen in the emergency department reports a 1-week history of worsening low back pain and a progressive neurologic deficit in the S1 distribution. Examination reveals 2/5 strength in the gastrocnemius. Laboratory studies show a WBC count of 13,500/mm3 and an erythrocyte sedimentation rate of 74 mm/h. Radiographs of the lumbosacral spine show narrowing of the L5-S1 disk space, with irregularity of the end plates. A sagittal T2-weighted MRI scan is shown in Figure 8. Definitive management should consist of
Explanation
Question 18
In a retroperitoneal approach to the lumbar spine, what structure runs along the medial aspect of the psoas and along the lateral border of the spine?
Explanation
Question 19
What is the most likely primary cause of decreased success rates of bony fusion in smokers undergoing lumbar arthrodesis?
Explanation
Question 20
Flexion-distraction injuries of the thoracolumbar spine are most frequently associated with injury to what organ system?
Explanation
Question 21
What is the most common adverse postoperative complication of laminoplasty for multilevel cervical spondylotic myelopathy?
Explanation
Question 22
The thickest bone in the occiput is located
Explanation
Question 23
A patient who underwent an L5-S1 diskectomy 18 months ago has persistent pain in the left leg. Figures 9a and 9b show postoperative axial T1-weighted MRI scans at the L5-S1 level without and with gadolinium. What is the most likely diagnosis?
Explanation
Question 24
Which of the following factors is most closely associated with early postoperative migration of "stand-alone" lumbar interbody fusion cages?
Explanation
Question 25
If a laminectomy for spinal stenosis is performed, which of the following is an indication for concomitant arthrodesis at that level?
Explanation
Question 26
A 45-year-old man presents with acute right anterior thigh pain and weakness in knee extension following a lifting injury. Physical examination reveals a diminished right patellar reflex and a positive femoral nerve stretch test. MRI of the lumbar spine reveals a large, far lateral (extraforaminal) disc herniation at the L4-L5 level on the right. Which of the following nerve roots is most likely being compressed?
Explanation
Question 27
A 62-year-old man with a 30-year history of ankylosing spondylitis presents to the emergency department with severe back pain after a mechanical fall from standing height. Neurologic examination is unremarkable. Radiographs and CT scans reveal a transverse fracture through the T10-T11 disc space extending through the fused posterior elements.
What is the most appropriate management for this patient?

Explanation
Question 28
A 58-year-old woman with a history of metastatic renal cell carcinoma presents with progressive back pain and mild bilateral lower extremity weakness (motor strength 4/5). MRI demonstrates an isolated L2 vertebral body metastasis with significant epidural extension and spinal cord compression. The patient has a life expectancy of greater than 12 months. What is the most appropriate treatment paradigm?
Explanation
Question 29
A 75-year-old woman sustains a Type II odontoid fracture after a fall. She is neurologically intact. Nonoperative management with a rigid cervical collar is being considered. Which of the following factors is most strongly associated with an increased rate of nonunion in this scenario?
Explanation
Question 30
An 11-year-old girl is evaluated for scoliosis. She is premenarchal. Radiographs demonstrate a right thoracic curve with a Cobb angle of 32 degrees. Her Risser stage is 0. What is the most appropriate recommendation?
Explanation
Question 31
A 16-year-old male gymnast has a 9-month history of localized lower back pain that worsens with extension. He has no radicular symptoms and his neurologic examination is normal. He has failed a comprehensive regimen of rest, NSAIDs, physical therapy, and a trial of bracing. Radiographs reveal a Grade 1 isthmic spondylolisthesis at L5-S1. What is the most appropriate surgical intervention?
Explanation
Question 32
A 65-year-old man presents with deteriorating handwriting, frequent dropping of objects, and a broad-based, unsteady gait. Physical examination reveals an inverted brachioradialis reflex. This highly specific finding is indicative of pathology at which of the following spinal levels?
Explanation
Question 33
A 54-year-old man with poorly controlled diabetes mellitus presents with severe, unrelenting mid-back pain, fevers, and new-onset bilateral leg weakness that has progressed over the last 12 hours. MRI with contrast reveals a large, dorsally located epidural collection from T6 to T9 with significant cord compression. What is the most appropriate next step in management?
Explanation
Question 34
An 8-year-old boy with Down syndrome is brought in by his parents for medical clearance to participate in gymnastics. He is completely asymptomatic and his neurologic exam is normal. Flexion-extension radiographs of the cervical spine demonstrate an atlantodens interval (ADI) of 7 mm. What is the most appropriate recommendation?
Explanation
Question 35
A 40-year-old man presents to the emergency department with acute onset of bilateral lower extremity weakness, perineal numbness, and sexual impotence following a heavy lifting incident. Examination reveals symmetrical 3/5 weakness in bilateral hip flexors, knee extensors, and ankle dorsiflexors. Deep tendon reflexes at the knees and ankles are hyperactive (3+). Anal sphincter tone is absent. Which of the following is the most likely diagnosis?
Explanation
Question 36
A 65-year-old female presents with progressive low back pain and difficulty standing upright. She has to bend her knees to look straight ahead. Radiographic analysis reveals a pelvic incidence (PI) of 60 degrees, a lumbar lordosis (LL) of 25 degrees, and a sagittal vertical axis (SVA) of +12 cm. She has failed all conservative management. What is the most critical radiographic goal of her surgical correction?
Explanation
Question 37
A 70-year-old male with progressive gait clumsiness and hand dexterity issues undergoes a C3-C6 cervical laminectomy and instrumented fusion. On postoperative day 2, he reports isolated profound bilateral deltoid and biceps weakness (Medical Research Council grade 2/5). Sensation and lower extremity function remain completely unchanged. Which of the following is the most likely etiology of this patient's new neurologic deficit?
Explanation
Question 38
A 35-year-old construction worker falls from a 15-foot scaffolding, sustaining severe middle back pain. Neurological examination is intact bilaterally (ASIA E). A CT scan of the thoracic spine demonstrates a T12 burst fracture with 40% loss of anterior vertebral body height, 15 degrees of focal kyphosis, and a vertical splitting fracture of the lamina. An MRI reveals fluid signal and disruption of the posterior ligamentous complex (PLC). Based on the Thoracolumbar Injury Classification and Severity (TLICS) score, what is the most appropriate management?
Explanation
Question 39
A 58-year-old male with a history of renal cell carcinoma presents with acute-onset bilateral lower extremity weakness (3/5 hip flexion, 4/5 knee extension), saddle anesthesia, and urinary retention. MRI reveals an extensive T8 metastatic lesion with high-grade epidural spinal cord compression (ESCC). What is the most appropriate next step in management?
Explanation
Question 40
A 14-year-old female gymnast presents with a 6-month history of mechanical low back pain. Radiographs demonstrate a Grade II L5-S1 spondylolisthesis. Advanced imaging confirms bilateral pars interarticularis defects at L5. She has failed 6 months of physical therapy, bracing, and NSAIDs. Her pain restricts her activities of daily living and sports. What is the most appropriate surgical treatment?
Explanation
Question 41
An 82-year-old male falls from a standing height. He has severe neck pain but a normal neurologic examination. CT scan reveals a Type II odontoid fracture with 2 mm of posterior displacement. Comorbidities include severe COPD, diabetes mellitus, and severe osteoporosis. Which of the following treatments provides the best balance of safety and efficacy for this specific patient?
Explanation
Question 42
A 45-year-old male with a long-standing history of ankylosing spondylitis presents to the emergency department after a low-speed motor vehicle collision. He complains of new-onset neck pain. Neurologic examination is unremarkable. Standard AP, lateral, and open-mouth odontoid plain radiographs are negative for fracture or dislocation. What is the most appropriate next step in the management of this patient?
Explanation
Question 43
A 52-year-old female presents with right-sided neck pain radiating down her arm. On examination, she has profound weakness in elbow extension and wrist flexion on the right side. She also exhibits diminished pinprick sensation over her middle finger and an absent triceps reflex. Which cervical nerve root is most likely compressed?
Explanation
Question 44
A 60-year-old diabetic patient presents with acute worsening back pain, low-grade fevers, and progressive bilateral lower extremity weakness over the last 48 hours. ESR and CRP are markedly elevated. MRI with contrast shows L3-L4 discitis/osteomyelitis with an associated anterior epidural abscess causing severe thecal sac compression. Blood cultures are pending. Examination reveals 3/5 strength in hip flexion and knee extension bilaterally. What is the most appropriate immediate management?
Explanation
Question 45
A 72-year-old male presents with bilateral leg pain and cramping that worsens with walking. The pain reliably improves when he sits down or leans over a shopping cart. To distinguish between neurogenic claudication and vascular claudication, the physician performs a stationary bicycle test (van Gelderen bicycle test). Which of the following findings during the test is most characteristic of neurogenic claudication?
Explanation
Question 46
A 65-year-old woman presents with severe low back pain and leaning forward when walking. Standing lateral radiographs show a Pelvic Incidence (PI) of 60 degrees, Pelvic Tilt (PT) of 35 degrees, and Lumbar Lordosis (LL) of 20 degrees. Her Sagittal Vertical Axis (SVA) is +12 cm. What is the goal of surgical correction for this patient based on the SRS-Schwab classification?
Explanation
Question 47
A 78-year-old man presents with neck pain after a ground-level fall. CT scan reveals a Type II odontoid fracture with 3 mm of posterior displacement. He is neurologically intact. He has a history of severe COPD, congestive heart failure, and coronary artery disease. What is the most appropriate management?
Explanation
Question 48
A 55-year-old male with diabetes presents with a 2-week history of worsening severe midthoracic back pain, low-grade fevers, and new-onset bilateral lower extremity weakness (motor strength 3/5). MRI with gadolinium reveals a posterior epidural fluid collection with rim enhancement at T7-T9 causing severe spinal cord compression. What is the most appropriate next step in management?
Explanation
Question 49
A 62-year-old man of East Asian descent presents with progressive clumsiness in his hands and an unsteady, broad-based gait. Examination shows a positive Hoffmann's sign bilaterally. Cervical spine CT demonstrates continuous ossification of the posterior longitudinal ligament (OPLL) from C3 to C6, causing severe canal stenosis. The K-line on a neutral lateral radiograph is plotted, and the OPLL mass anteriorly crosses the K-line (K-line negative). Which of the following is true regarding this finding?
Explanation
Question 50
A 22-year-old restrained driver is involved in a high-speed motor vehicle collision. He complains of severe back pain. CT scans of the thoracolumbar spine show a transverse fracture through the L1 spinous process, pedicles, and posterior vertebral body, with widening of the posterior elements. There is no translation. What associated intra-abdominal injury is most likely to be present?
Explanation
Question 51
A 50-year-old man with a long-standing history of ankylosing spondylitis presents to the emergency department after a low-speed rear-end motor vehicle collision. He reports new-onset neck pain but no neurologic deficits. Initial plain radiographs of the cervical spine are reported as 'normal'. What is the most appropriate next step in management?
Explanation
Question 52
A 16-year-old female gymnast presents with a 6-month history of low back pain and left leg pain that worsens with activity. Examination reveals hamstring tightness and an L5 step-off. Radiographs show a grade II L5-S1 isthmic spondylolisthesis. She is scheduled for L5-S1 decompression and instrumented fusion. During reduction of the L5 vertebra, which nerve root is at highest risk for iatrogenic injury?
Explanation
Question 53
A 45-year-old man presents with acute onset severe low back pain, bilateral lower extremity radicular pain, and numbness in his perineal region. He reports difficulty urinating for the past 12 hours. Bladder scan reveals a post-void residual (PVR) of 450 mL. An MRI of the lumbar spine shows a massive L4-L5 central disc herniation. What is the most significant prognostic factor for recovery of bladder function following surgical decompression?
Explanation
Question 54
A 35-year-old male undergoes an anterior lumbar interbody fusion (ALIF) at L5-S1 for degenerative disc disease. Postoperatively, he notes normal erectile function but reports a lack of seminal emission during orgasm. This complication is most likely due to injury of which of the following structures?
Explanation
Question 55
A 60-year-old woman with a history of breast cancer presents with progressive mechanical back pain. Standing radiographs and MRI reveal a lytic metastatic lesion at T10 involving the vertebral body and left pedicle. The lesion occupies 60% of the vertebral body height. She has kyphosis of 15 degrees at this level, and pain is reproducible with loading and relieved by lying down. According to the Spinal Instability Neoplastic Score (SINS), which of the following features contributes most to classifying this lesion as unstable?
Explanation
Question 56
A 65-year-old man presents with a 6-month history of progressive difficulty buttoning his shirts and an unsteady gait. On examination, he demonstrates bilateral positive Hoffmann signs, an inverted brachioradialis reflex, and lower extremity hyperreflexia.
The lateral cervical radiograph demonstrates a fixed 15-degree cervical kyphosis centered at C4-C6. MRI reveals severe central canal stenosis with anterior cord compression and T2 hyperintensity at C4-C5 and C5-C6. Which of the following is the most appropriate surgical intervention?

Explanation
Question 57
A 55-year-old diabetic man presents to the emergency department with severe midthoracic back pain, a fever of 39.0°C (102.2°F), and rapidly progressive paraparesis over the last 24 hours. A STAT thoracic spine MRI with contrast demonstrates a large dorsal epidural abscess spanning from T8 to T10, causing severe spinal cord compression. There is no evidence of anterior column instability, discitis, or osteomyelitis. What is the most appropriate immediate management?
Explanation
Question 58
A 30-year-old man presents to the trauma bay after falling 10 feet from a ladder. He complains of moderate low back pain. He is neurologically intact with 5/5 strength in all myotomes and normal bowel/bladder function.
A CT scan shows an L2 burst fracture with 20% loss of anterior vertebral body height, 10 degrees of regional kyphosis, 30% canal compromise, and an intact posterior osseous-ligamentous complex. What is the recommended treatment?

Explanation
Question 59
An 82-year-old woman with a history of severe osteoporosis and multiple medical comorbidities presents after a low-speed motor vehicle collision. She reports severe upper neck pain. She is neurologically intact.
A cervical CT scan reveals a Type II odontoid fracture with 3 mm of posterior displacement. What is the most appropriate initial management for this patient?

Explanation
Question 60
A 45-year-old man with known ankylosing spondylitis presents to the emergency department after a seemingly minor mechanical fall from standing height. He complains of severe, localized, and new-onset mid-back pain. Anteroposterior and lateral thoracic spine radiographs demonstrate extensive syndesmophyte formation but are otherwise read as 'unremarkable' by the radiologist. His neurologic examination is perfectly normal. What is the most appropriate next step in management?
Explanation
Question 61
A 60-year-old woman presents with a 4-month history of right-sided neck and arm pain radiating into her middle finger, consistent with a C7 radiculopathy. Five years ago, she underwent a C5-C6 anterior cervical diskectomy and fusion (ACDF). Radiographs show a solid fusion at C5-C6 and new, severe disc space narrowing and foraminal osteophytosis at C6-C7.
She has failed 6 months of comprehensive non-operative management. What is the most appropriate surgical option?
Explanation
Question 62
A 14-year-old female gymnast presents with persistent lower back pain that has prevented her from participating in sports for the past 8 months. She has undergone extensive physical therapy, bracing, and activity modification without relief. Radiographs reveal a Grade II isthmic spondylolisthesis at L5-S1 with 35% translation. Her neurologic examination is intact. What is the recommended surgical procedure for this patient?
Explanation
Question 63
A 40-year-old man is transported to the trauma center after a high-speed motorcycle collision. On physical examination, he has dense bilateral loss of motor function, as well as loss of pain and temperature sensation below the T10 dermatomal level. However, his proprioception, vibratory sense, and fine touch sensation remain intact in his lower extremities. Which of the following spinal cord injury syndromes does this presentation most accurately describe?
Explanation
Question 64
A 68-year-old woman presents with progressively worsening lower back pain and an inability to stand completely upright. She notes that she must consciously bend her knees to maintain a forward gaze. Standing full-length scoliosis radiographs reveal a Pelvic Incidence (PI) of 60 degrees, a Lumbar Lordosis (LL) of 20 degrees, and a Sagittal Vertical Axis (SVA) of +12 cm. What is the primary radiographic goal in the surgical correction of her adult spinal deformity?
Explanation
Question 65
A 72-year-old man presents with a 2-year history of worsening bilateral buttock and posterior thigh pain when walking. His symptoms are consistently relieved by sitting down or leaning forward over a shopping cart. Bilateral lower extremity pulses are palpable and bounding, and his neurologic exam is unremarkable. An MRI reveals severe central canal stenosis at L3-L4 and L4-L5 secondary to significant ligamentum flavum hypertrophy and facet arthropathy. Flexion-extension radiographs show no evidence of spondylolisthesis or dynamic instability. After failing 6 months of physical therapy and epidural steroid injections, what is the most appropriate surgical management?
Explanation
Question 66
A 32-year-old man is evaluated in the emergency department after a shallow water diving accident. He is awake, alert, and fully cooperative. Neurologic examination demonstrates 0/5 strength in the bilateral triceps, finger flexors, and hand intrinsics, but 5/5 strength in the deltoids and biceps. Sensation is decreased in the C7, C8, and T1 dermatomes bilaterally. Lateral radiographs reveal a bilateral C6-C7 facet dislocation. Which of the following is the most appropriate initial management?
Explanation
Question 67
A 62-year-old woman presents with severe, unrelenting mid-back pain and progressive lower extremity weakness. She has a history of renal cell carcinoma. Imaging reveals a solitary lytic lesion at T12 with severe collapse of the vertebral body and bony retropulsion causing severe spinal cord compression. Oncology determines her expected survival is greater than 12 months. Which of the following treatment strategies is most appropriate?
Explanation
Question 68
A 68-year-old woman with a prior L3-S1 fusion presents with severe back pain, a stooped posture, and an inability to stand up straight. Standing full-length radiographs show a pelvic incidence (PI) of 60 degrees, lumbar lordosis (LL) of 20 degrees, pelvic tilt (PT) of 35 degrees, and a sagittal vertical axis (SVA) of +12 cm. Revision corrective spinal osteotomy is planned. To optimize sagittal balance, what is the minimum lumbar lordosis (LL) that should be targeted during the reconstruction?
Explanation
Question 69
A 14-year-old girl presents with severe low back pain and significant hamstring tightness. She stands with a characteristic 'pelvic waddle' gait. Lateral radiographs demonstrate a Grade 4 dysplastic isthmic spondylolisthesis at L5-S1 with a high slip angle. Nonoperative management has failed. Surgical planning includes an L4-to-pelvis posterior instrumented fusion with partial reduction of the L5 vertebral body. Which nerve root is at the highest risk of injury during the reduction maneuver?
Explanation
Question 70
A 55-year-old Asian man presents with an 8-month history of progressive clumsy hands, gait instability, and hyperreflexia. A positive Hoffman's sign is present bilaterally. CT of the cervical spine shows continuous ossification of the posterior longitudinal ligament (OPLL) from C3 to C6. The sagittal MRI shows cervical kyphosis, and the ossified mass crosses the K-line (K-line negative). Which surgical approach is most appropriate to halt the progression of his myelopathy?
Explanation
Question 71
A 65-year-old woman is evaluated for neurogenic claudication secondary to a symptomatic Grade 1 degenerative spondylolisthesis at L4-L5. She is deciding between operative and nonoperative management. Based on the 8-year long-term results of the Spine Patient Outcomes Research Trial (SPORT) for degenerative spondylolisthesis, what should she be counseled regarding her treatment options?
Explanation
Question 72
A 28-year-old male is intubated following a high-speed motor vehicle collision. A lateral cervical spine radiograph reveals a basion-dental interval (BDI) of 14 mm and a basion-posterior axial line interval (BBAI) of 15 mm. A subsequent MRI demonstrates complete disruption of the tectorial membrane and alar ligaments. What is the definitive management for this injury?
Explanation
Question 73
A 72-year-old woman undergoes a T10 to pelvis posterior instrumented fusion for adult spinal deformity. Six months later, she returns with localized mechanical back pain at the thoracolumbar junction. Radiographs demonstrate an abnormal kyphotic angulation measuring 18 degrees between the upper instrumented vertebra (UIV) and the UIV+2 (compared to 4 degrees postoperatively). She is neurologically intact. Which of the following is the most significant modifiable surgical risk factor for this specific complication?
Explanation
Question 74
A 54-year-old man with uncontrolled diabetes presents with severe mid-back pain, fevers, and acute lower extremity weakness evolving over 24 hours. His temperature is 38.8°C. ESR is 95 mm/hr and CRP is 120 mg/L. Gadolinium-enhanced MRI reveals a T8-T9 discitis/osteomyelitis with a large ventral epidural abscess causing severe anterior compression of the thoracic spinal cord. What is the most appropriate initial surgical approach?
Explanation
Question 75
A 42-year-old man presents with an acute onset of severe bilateral sciatica, saddle anesthesia, and urinary retention. Post-void residual volume is 600 mL. MRI demonstrates a massive central disc herniation at L4-L5 completely obliterating the thecal sac. Symptoms began 12 hours ago, and urgent surgical decompression is planned. What is the predominant pathophysiological mechanism causing nerve root injury in this syndrome?
Explanation
Question 76
A 55-year-old man presents with progressive clumsiness in his hands and difficulty walking. He has a positive Hoffman's sign and hyperreflexia in the lower extremities. MRI shows multilevel cervical stenosis from C3 to C6. He has neutral sagittal alignment but prominent retrovertebral osteophytes. He undergoes a multilevel posterior cervical laminectomy and fusion. What is the most common postoperative neurologic complication specific to this posterior approach?
Explanation
Question 77
A 35-year-old construction worker falls from a height of 15 feet and sustains a T12 burst fracture. On examination, he is neurologically intact with 5/5 motor strength and normal bowel/bladder function. Upright radiographs show 25 degrees of local kyphosis, and CT shows 40% canal compromise. An MRI reveals that the posterior ligamentous complex (PLC) is completely intact. What is the most appropriate management?
Explanation
Question 78
A 65-year-old woman presents with severe low back pain and an inability to stand up straight, reporting progressive fatigue when walking. Radiographs reveal a degenerative lumbar scoliosis with marked sagittal imbalance. Her measured pelvic incidence (PI) is 65 degrees. For an optimal postoperative functional outcome in sagittal alignment, her lumbar lordosis (LL) should be surgically restored to approximately:
Explanation
Question 79
A 15-year-old male gymnast presents with a 3-week history of worsening low back pain that is significantly exacerbated by extension activities. Plain radiographs, including oblique views, show no definitive fracture lines. An MRI of the lumbar spine without contrast reveals increased T2/STIR signal (marrow edema) in the L5 pars interarticularis bilaterally, without a visible fracture gap on T1-weighted sequences. What is the most appropriate initial management?
Explanation
Question 80
An 82-year-old woman with a medical history of severe severe chronic obstructive pulmonary disease and recent myocardial infarction falls from standing height. She complains of isolated neck pain. A CT scan of the cervical spine reveals a Type II odontoid fracture with 2 mm of posterior displacement. She is neurologically intact. What is the most appropriate definitive management?
Explanation
Question 81
A 45-year-old man underwent an L4-L5 posterior lumbar interbody fusion (PLIF) 10 days ago for degenerative spondylolisthesis. He now presents to the emergency department with worsening incisional back pain, fever to 38.8°C, and new purulent drainage from the wound. Laboratory tests reveal a CRP of 150 mg/L and an ESR of 85 mm/h. MRI with gadolinium demonstrates an enhancing fluid collection deep to the fascia, adjacent to the spinal instrumentation. What is the next best step in management?
Explanation
Question 82
A 42-year-old man with a 15-year history of ankylosing spondylitis presents to the trauma bay after a minor, low-speed motor vehicle collision. He complains of moderate lower neck pain. Neurological examination is unremarkable. Standard anteroposterior, lateral, and open-mouth odontoid radiographs are obtained and read as normal. What is the most appropriate next step in his evaluation?
Explanation
Question 83
A 60-year-old man with an established history of metastatic prostate cancer presents with rapidly progressive bilateral lower extremity weakness, sensory deficits, and urinary retention over the last 48 hours. MRI reveals an anterior metastatic lesion at T8 causing severe anterior spinal cord compression. He has a Karnofsky Performance Status of 80 and an expected survival of greater than 6 months. What is the most appropriate initial surgical management?
Explanation
Question 84
A 40-year-old construction worker presents with a 2-year history of debilitating low back pain and bilateral L5 radiculopathy that has failed comprehensive conservative management. Upright radiographs demonstrate a Grade II L5-S1 isthmic spondylolisthesis. MRI confirms bilateral severe L5 foraminal stenosis. What is the most appropriate surgical treatment?
Explanation
Question 85
A 6-year-old girl is brought to the clinic by her parents. She is holding her head tilted to the right and rotated to the left. Her parents report this deformity occurred suddenly following a mild upper respiratory tract infection 2 weeks ago. She has tenderness over the upper cervical spine. An open-mouth odontoid view and dynamic CT scan confirm atlantoaxial rotatory subluxation (AARS) Fielding Type I. What is the initial treatment of choice?
Explanation
Question 86
A 24-year-old male arrives at the trauma bay after a high-speed motor vehicle collision. He has 0/5 strength in his lower extremities, 0/5 in wrist flexion and finger extension, but 3/5 in bilateral elbow flexion. He is awake, alert, and fully cooperative. Lateral cervical radiographs demonstrate a bilateral C5-C6 facet dislocation. What is the most appropriate next step in his management?
Explanation
Question 87
A 65-year-old male with long-standing ankylosing spondylitis presents to the emergency department after a ground-level fall. He complains of severe neck pain. He is neurologically intact. Initial plain radiographs of the cervical spine are obscured by the shoulders but read by the resident as showing no acute fracture.
What is the most appropriate next step in his management?
Explanation
Question 88
A 62-year-old female presents with severe low back pain and difficulty standing upright. She constantly leans forward to walk. Standing full-length scoliosis radiographs show a pelvic incidence (PI) of 65 degrees, lumbar lordosis (LL) of 30 degrees, and a sagittal vertical axis (SVA) of +12 cm. If surgical intervention is planned, which of the following sagittal alignment goals is most critical to achieve optimal clinical outcomes and reduce the risk of adjacent segment disease?
Explanation
Question 89
An 82-year-old male with a history of severe COPD and ischemic heart disease presents with neck pain after a low-speed motor vehicle collision. CT scan demonstrates a Type II odontoid fracture with 2 mm of posterior displacement. He is neurologically intact. Which of the following is the most appropriate initial management for this patient?
Explanation
Question 90
A 65-year-old female presents with a 2-year history of bilateral lower extremity heaviness and cramping that worsens with walking and improves when leaning over a shopping cart. She has failed 6 months of conservative management. MRI reveals severe L4-L5 spinal stenosis with a stable Grade I degenerative spondylolisthesis. According to the Spine Patient Outcomes Research Trial (SPORT), which of the following statements is true regarding her treatment options?
Explanation
Question 91
A 58-year-old male presents with deteriorating handwriting, difficulty buttoning his shirts, and frequent tripping over the last six months. On physical examination, flicking the nail of his middle finger results in reflexive flexion of the thumb and index finger. This specific clinical sign indicates pathology in which of the following anatomic locations?
Explanation
Question 92
A 54-year-old male with a history of intravenous drug use presents with severe mid-back pain, fevers, and new-onset lower extremity weakness (motor strength 3/5 bilaterally). His temperature is 38.9°C (102.0°F), ESR is 110 mm/hr, and CRP is 85 mg/L. MRI of the thoracic spine with gadolinium shows a posterior epidural fluid collection at T6-T8 compressing the spinal cord.
What is the most appropriate next step in management?
Explanation
Question 93
A 60-year-old male undergoes a multi-level posterior cervical laminectomy and instrumented fusion (C3-C7) for severe cervical spondylotic myelopathy. On postoperative day 2, he is noted to have new profound weakness in right shoulder abduction and external rotation (strength 1/5). His grip strength, wrist extension, and lower extremity strength remain intact. What is the most likely etiology of this new deficit?
Explanation
Question 94
A 15-year-old boy is brought by his parents for evaluation of a 'hunchback' posture. He reports mild achy pain in the mid-back after playing sports. Standing lateral radiographs demonstrate a thoracic kyphosis of 65 degrees. According to Sorensen's criteria, which of the following radiographic findings is required to confirm the diagnosis of Scheuermann's disease?
Explanation
Question 95
A 42-year-old male presents to the emergency department with severe lower back pain and bilateral sciatica. He reports new-onset perineal numbness and difficulty initiating urination for the past 12 hours. On physical examination, he has decreased perianal sensation and decreased rectal tone.
The urinary retention seen in this syndrome is primarily due to dysfunction of which of the following nerve roots?

Explanation
Question 96
An 84-year-old man is brought to the emergency department after a ground-level fall. He complains of severe neck pain but denies any numbness, tingling, or weakness in his extremities. His medical history is significant for severe chronic obstructive pulmonary disease (COPD), coronary artery disease with a previous myocardial infarction, and poorly controlled diabetes mellitus. Neurological examination is completely intact. A CT scan of the cervical spine reveals a Type II odontoid fracture with 2 mm of posterior displacement. What is the most appropriate management for this patient?
Explanation
Question 97
A 62-year-old man presents with progressive hand clumsiness, difficulty walking, and frequent tripping over the past 8 months. Physical examination demonstrates hyperreflexia in the bilateral lower extremities, a positive Hoffmann sign bilaterally, and an inverted brachioradialis reflex. Imaging shows multi-level cervical spondylosis from C3 to C6. A sagittal MRI reveals severe spinal cord compression from large anterior diskosteophyte complexes. Standing lateral radiographs demonstrate a rigid 15-degree kyphotic deformity of the cervical spine from C3 to C6. Which of the following surgical approaches is most appropriate?
Explanation
Question 98
A 65-year-old woman is being evaluated for progressive low back pain and an inability to stand up straight, which severely limits her daily activities. Standing full-length lateral spinopelvic radiographs are obtained to plan a multi-level corrective spinal fusion. Measurement of her spinopelvic parameters demonstrates a pelvic incidence (PI) of 60 degrees. To achieve optimal sagittal balance postoperatively and minimize the risk of adjacent segment disease, what is the ideal target for her lumbar lordosis (LL)?
Explanation
Question 99
A 45-year-old man undergoes an anterior cervical discectomy and fusion (ACDF) at C5-C6 through a right-sided, transverse cervical approach. On postoperative day 1, he is noted to have severe hoarseness and coughing when attempting to drink thin liquids. Laryngoscopy confirms unilateral vocal cord paralysis. The injured structure responsible for this complication typically courses in which of the following anatomic locations?
Explanation
Question 100
A 55-year-old woman undergoes a posterior C3-C7 laminectomy and instrumented fusion for severe cervical spondylotic myelopathy. Postoperatively, she awakens with improved bilateral lower extremity function and intact sensation globally. However, on postoperative day 3, she develops acute, isolated right-sided weakness in shoulder abduction and elbow flexion (Medical Research Council grade 2/5). Sensation in the upper extremities remains intact. What is the most appropriate next step in management?
Explanation
None
