Orthopedic Spine 2026 MCQs: Board Review Questions & Answers (Part 4)

Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Orthopedic Spine 2026 MCQs: Board Review Questions & Answers (Part 4). Top-rated Orthopedic Spine 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Spine 2026 MCQs: Board Review Questions & Answers (Part 4)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figures 29a and 29b show the AP and lateral radiographs of a 30-year-old man who has increasingly worse back pain and stiffness. Examination shows painful, limited spinal range of motion. There is no neurologic deficit. What laboratory study would be most helpful in confirming the diagnosis?
Explanation
Question 2
A 29-year-old man undergoes surgery for a grade I isthmic spondylolisthesis at L5. Following surgery, what type of brace will best immobilize the L5-S1 motion segment?
Explanation
Question 3
When examining a patient with marked hyperreflexia, which of the following findings best suggests that the condition is not caused by a cerivcal spine pathology?
Explanation
Question 4
The artery of Adamkiewicz (arteria radicularis, arteria magna) is most commonly found on the
Explanation
Question 5
A 62-year-old man with a long history of ankylosing spondylitis has neck pain after lightly bumping his head on the wall. Examination reveals neck pain with any attempted motion; the neurologic examination is normal. Plain radiographs show extensive ankylosis of the cervical spine and kyphosis but no fracture. What is the next most appropriate step in management?
Explanation
Question 6
A young man sustains a lumbar strain in an on-the-job motor vehicle accident. Both he and his treating physician feel that he is capable of limited duty with appropriate restrictions shortly after the injury. What term best describes his work status?
Explanation
Question 7
Based on the findings seen at C5-6 in Figure 30, the most likely deficit for this patient will be weakness of the
Explanation
Question 8
A 40-year-old woman with no history of back problems has a symptomatic L4-5 disk herniation with an L5 radiculopathy that has failed to respond to 12 weeks of nonsurgical management. In the preoperative discussion, the surgeon advises the patient that the chance of recurrence of the herniation after successful diskectomy is what percent?
Explanation
Question 9
In the normal adult, the distance between the basion and the tip of the dens with the head in neutral position is how many millimeters?
Explanation
Question 10
The postoperative neurologic prognosis of a patient who has a tumor that is compressing the spinal cord and causing a neurologic deficit depends primarily on the
Explanation
Question 11
An otherwise healthy 32-year-old man who underwent an uneventful L5-S1 lumbar microdiskectomy 6 weeks ago now reports increasing and severe back pain that awakens him from sleep. Examination reveals a benign-appearing wound, and the neurologic examination is normal. Laboratory studies show an erythrocyte sedimentation rate (ESR) of 90 mm/h and a WBC of 9,000/mm3. Plain radiographs are normal. What is the next most appropriate step in management?
Explanation
Question 12
An 81-year-old man with severe low back pain reports right extensor hallucis longus and anterior tibialis weakness and difficulty urinating over the past 24 hours. He has a temperature of 101 degrees F (38.3 degrees C). MRI scans are shown in Figures 31a and 31b. Management should consist of
Explanation
Question 13
A 25-year-old man has chronic back pain that has been slowly worsening. He has no constitutional symptoms, and he denies any previous medical problems. Examination shows a tall lean build with no objective neurologic findings or skin lesions. Figure 32 shows a T2-weighted sagittal MRI scan. What is the most likely diagnosis?
Explanation
Question 14
Which of the following factors has the most effect on the pullout strength of lumbar transpedicular screw fixation?
Explanation
Question 15
Examination of a 34-year-old man who has had left leg pain for the past 6 weeks reveals minimal weakness of the left extensor hallucis longus and normal ankle jerk and patellar reflexes. Figure 33 shows an axial MRI scan of the L4-5 disk. Based on these findings, the MRI scan results are consistent with compression of the
Explanation
Question 16
A 20-year-old college athlete is seen for follow-up after sustaining an injury at football practice 2 days ago. He reports that he tackled a player and felt neck pain and numbness in both arms. The numbness resolved within seconds, but his neck remains painful and stiff. He denies any history of neck pain or injury. Examination reveals limited neck motion. The neurologic examination and radiographs are normal. MRI scans of the cervical spine are shown in Figure 34. During counseling, the patient, his family, and his coach should be informed that he has an acute cervical disk herniation and cannot play
Explanation
Question 17
An Asian 45-year-old man has bilateral upper extremity dysfunction. Figure 35a shows a T2-weighted sagittal MRI scan of the cervical spine, and Figure 35b shows a T2-weighted axial MRI scan at the level of the C3 vertebral body. What is the most likely pathologic process?
Explanation
Question 18
A 36-year-old man has a moderate-sized left paracentral L5-S1 disk herniation with compression of the S1 nerve. Examination will most likely reveal sensory changes at what location?
Explanation
Question 19
In a patient with a C5-6 herniation, the most likely sensory deficit will be in the
Explanation
Question 20
A 78-year-old woman has had activity-limiting cervical pain and occipital headaches for the past 4 years. Management consisting of injections, analgesics, and part-time collar wear has provided temporary relief. Examination reveals that her neck pain seems to be primarily located immediately below the skull and is aggravated by long periods of sitting and rotation of her head. Plain radiographs are shown in Figures 36a through 36c. What is the best course of action?
Explanation
Question 21
Contraindications to cervical laminectomy as a treatment for cervical spondylotic myelopathy include which of the following findings?
Explanation
Question 22
What arterial vessel is most prone to injury during posterior iliac crest bone graft harvest?
Explanation
Question 23
A 30-year-old man who underwent an anterior lumbar diskectomy and fusion at L4-5 and L5-S1 through an anterior retroperitoneal approach 1 month ago now reports he is unable to obtain and maintain an erection. The most likely cause of this condition is
Explanation
Question 24
Which of the following statements about injury of the anterior vascular structures during lumbar disk surgery is true?
Explanation
Question 25
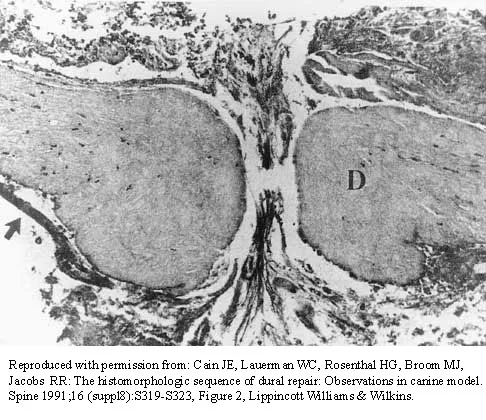
The photomicrograph in Figure 37 shows a repaired dural tear 4 days after surgery. The material interposed between the dural edges (D) is composed of
Explanation
Question 26
A patient with signs of myelopathy exhibits a hyperactive jaw jerk reflex on physical examination. Which of the following best describes the most likely anatomic location of the primary pathology?
Explanation
Question 27
A 60-year-old woman with long-standing rheumatoid arthritis presents with progressive neck pain and subjective hand clumsiness. Flexion-extension radiographs reveal an atlantodental interval (ADI) of 11 mm. What is the most appropriate management?
Explanation
Question 28
A 24-year-old man is involved in a motor vehicle accident and sustains a traumatic spondylolisthesis of the axis (Hangman's fracture). Imaging shows severe angulation with minimal translation, and flexion-extension views demonstrate an opening of the posterior C2-C3 disc space (Type IIA). Which of the following treatments is strictly contraindicated?
Explanation
Question 29
A 45-year-old man presents with sharp radicular pain radiating down the posterior aspect of his right leg to the lateral border of his foot. On examination, he exhibits an absent Achilles reflex and weakness in plantar flexion. Which nerve root is most likely compressed?
Explanation
Question 30
A 65-year-old man with underlying cervical spondylosis falls forward and strikes his chin, sustaining a hyperextension injury. He immediately develops profound weakness in his upper extremities with relatively preserved motor function in his lower extremities. What is the most likely diagnosis?
Explanation
Question 31
A 55-year-old man with a long-standing history of ankylosing spondylitis sustains a minor ground-level fall. He complains of severe lower cervical neck pain, but initial plain radiographs in the emergency department are read as normal. What is the next best step in management?
Explanation
Question 32
A 60-year-old man undergoes a C3-C6 posterior cervical laminectomy and fusion for cervical spondylotic myelopathy. On postoperative day 2, he develops profound new weakness in right shoulder abduction and elbow flexion, but has no new sensory deficits or leg symptoms. What is the most likely etiology?
Explanation
Question 33
A 15-year-old female gymnast presents with chronic, insidious-onset low back pain that significantly worsens with spinal extension. Her neurologic examination is normal. Plain radiographs show a bilateral radiolucent line across the pars interarticularis of L5. What is the most appropriate initial management?
Explanation
Question 34
A 35-year-old woman is involved in a high-speed collision. CT of the thoracolumbar spine demonstrates an L1 burst fracture with a fracture of the posterior elements.
Her neurologic examination is normal. The TLICS score is calculated as 5 (Morphology=2; PLC=3; Neuro=0). What is the recommended management?

Explanation
Question 35
In the surgical evaluation and reconstruction of adult degenerative scoliosis, achieving proper sagittal balance is highly correlated with improved clinical outcomes. Which of the following spinopelvic parameters is the primary target?
Explanation
Question 36
A 22-year-old man is a restrained backseat passenger (lap belt only) in a motor vehicle collision. He sustains a flexion-distraction injury to his lumbar spine (Chance fracture). Which associated injury must be most actively excluded during his trauma workup?
Explanation
Question 37
A 62-year-old man with poorly controlled diabetes presents with severe, unrelenting back pain and low-grade fevers. MRI with contrast reveals increased T2 signal in the L3-L4 intervertebral disc and adjacent vertebral endplates with enhancement. What is the most common causative organism?
Explanation
Question 38
A 16-year-old boy presents with progressive rounding of his upper back and mild pain after prolonged sitting. Lateral radiographs show a rigid thoracic kyphosis of 55 degrees. Which of the following radiographic findings definitively meets the Sorensen criteria for Scheuermann's disease?
Explanation
Question 39
A 40-year-old man presents to the emergency department with severe low back pain, bilateral leg weakness, and numbness in his perineal region. He reports he has not urinated in 14 hours. A bedside bladder ultrasound shows a post-void residual (PVR) volume of 600 mL. What is the most appropriate next step?
Explanation
Question 40
A 75-year-old woman sustains a Type II odontoid fracture after a ground-level fall. Which of the following factors is most strongly associated with a high rate of nonunion if managed nonoperatively with a halo vest?
Explanation
Question 41
A 68-year-old man complains of bilateral calf and thigh pain that occurs after walking two blocks. The pain is rapidly relieved when he leans forward on a shopping cart or sits down. Standing perfectly upright exacerbates the pain. His pedal pulses are strongly palpable. What is the most likely diagnosis?
Explanation
Question 42
A 30-year-old woman is brought to the trauma bay after a rollover motor vehicle collision. She is fully awake, alert, and neurologically intact. Cervical spine CT demonstrates a left-sided unilateral facet dislocation at C5-C6. What is the most appropriate next step in management?
Explanation
Question 43
A 45-year-old man presents with right arm pain radiating to the lateral forearm and thumb. He has weakness in wrist extension and a diminished brachioradialis reflex. Which of the following nerve roots is most likely affected?
Explanation
Question 44
A 25-year-old man is involved in a motor vehicle collision. Imaging reveals a fracture through the pars interarticularis of C2 bilaterally with 2 mm of displacement and no angulation. According to the Levine and Edwards classification, what is the most appropriate management?
Explanation
Question 45
A 70-year-old man with a history of cervical spondylosis falls forward, striking his chin. He presents with profound motor weakness in his upper extremities but is able to move his lower extremities against gravity. He has variable sensory loss and urinary retention. Which of the following is the most likely diagnosis?
Explanation
Question 46
A 15-year-old male gymnast complains of worsening lower back pain exacerbated by extension. Oblique radiographs demonstrate a 'collar on the Scotty dog' appearance. Which of the following is the most appropriate initial management?
Explanation
Question 47
A 55-year-old man with long-standing ankylosing spondylitis presents to the emergency department after a minor ground-level fall. He complains of severe lower neck pain. Neurological examination is intact. Initial plain radiographs of the cervical spine are difficult to interpret due to patient positioning and underlying deformity. What is the most appropriate next step in management?
Explanation
Question 48
A 60-year-old woman with a history of multiple myeloma presents with progressively worsening back pain and new-onset lower extremity weakness. MRI demonstrates a T8 vertebral body metastatic lesion with epidural spinal cord compression. She has no mechanical instability. According to the NOMS framework, what is the best initial treatment?
Explanation
Question 49
A 42-year-old man presents to the emergency department with severe lower back pain, bilateral sciatica, saddle anesthesia, and urinary incontinence. Which of the following is the most critical next step?
Explanation
Question 50
Which of the following radiographic criteria is definitively diagnostic for Diffuse Idiopathic Skeletal Hyperostosis (DISH)?
Explanation
Question 51
During the physical examination of a patient with suspected cervical myelopathy, you perform a rapid flicking of the distal phalanx of the middle finger, which elicits an involuntary flexion of the thumb and index finger. What is the name of this clinical sign?
Explanation
Question 52
A 75-year-old woman presents with a displaced Type II odontoid fracture after a fall. What is the major disadvantage of utilizing a halo vest orthosis in this specific patient population compared to a rigid cervical collar?
Explanation
Question 53
A 65-year-old man presents with neurogenic claudication characterized by bilateral leg pain and heaviness that worsens with walking and improves when leaning forward over a shopping cart. What is the primary anatomical structure responsible for dorsal central canal narrowing in degenerative lumbar spinal stenosis?
Explanation
Question 54
A patient suffers a penetrating knife injury to the right side of the spinal cord at the T10 level. Which of the following neurological deficits is expected below the level of the injury?
Explanation
Question 55
A 60-year-old woman with a 20-year history of rheumatoid arthritis presents for preoperative evaluation before a total knee arthroplasty. Flexion-extension radiographs of the cervical spine reveal an anterior atlantodental interval (ADI) of 6 mm. What is the most appropriate next step?
Explanation
Question 56
Which of the following surgical approaches is generally contraindicated for the treatment of a central, calcified thoracic disc herniation causing myelopathy?
Explanation
Question 57
A 22-year-old woman is involved in a high-speed motor vehicle collision while wearing a lap belt. She sustains a flexion-distraction injury (Chance fracture) of L1. What concomitant injury must be heavily suspected and evaluated for?
Explanation
Question 58
A 55-year-old woman presents with neurogenic claudication and lower back pain. Radiographs reveal a grade 1 degenerative spondylolisthesis at L4-L5. She has failed six months of physical therapy and injections. Which of the following is the most appropriate surgical intervention based on major clinical trials?
Explanation
Question 59
A 65-year-old man presents with acute bilateral leg pain, urinary retention, and saddle anesthesia. Post-void residual (PVR) ultrasound is 400 mL. Which of the following urodynamic findings is most consistent with the underlying pathophysiology of this syndrome?
Explanation
Question 60
A 45-year-old man presents with severe radicular leg pain. MRI demonstrates a far-lateral disc herniation at the L4-L5 level. Which of the following physical examination findings is most likely to be present?
Explanation
Question 61
A 72-year-old woman sustains a hyperextension injury to her cervical spine. She presents with significant weakness in her upper extremities, but her lower extremities have 4/5 motor strength. Which function is typically the last to recover in this specific spinal cord syndrome?
Explanation
Question 62
A 24-year-old male is involved in a high-speed motor vehicle collision. On presentation, his blood pressure is 80/50 mmHg and heart rate is 50 bpm. His extremities are warm and well-perfused. Which of the following is the primary pathophysiological mechanism for his vital sign abnormalities?
Explanation
Question 63
A
14-year-old girl is evaluated for scoliosis. Radiographs reveal a right thoracic curve of 42 degrees. Her Risser stage is 0 and she is premenarchal. What is the most appropriate next step in management?

Explanation
Question 64
A 55-year-old man presents with progressive gait difficulty and hand clumsiness. Examination reveals hyperreflexia, a positive Hoffman's sign, and difficulty buttoning his shirt. Which of the following tests best differentiates cervical myelopathy from a central nervous system pathology above the foramen magnum?
Explanation
Question 65
During a posterior approach for a TLIF at L4-L5, a pedicle screw is being placed into the right L4 vertebra. A medial breach of the pedicle wall occurs. Which neural structure is at greatest risk of iatrogenic injury?
Explanation
Question 66
An 82-year-old man presents with neck pain following a ground-level fall. CT scan reveals a Type II odontoid fracture with 2 mm of displacement. He has a history of severe COPD, congestive heart failure, and diabetes. What is the most appropriate definitive management?
Explanation
Question 67
A
35-year-old man is diagnosed with an unstable T12 thoracolumbar burst fracture with MRI-confirmed posterior ligamentous complex (PLC) disruption. He is neurologically intact. Based on the Thoracolumbar Injury Classification and Severity (TLICS) score, what is his point value and the recommended treatment?

Explanation
Question 68
In a patient with adolescent idiopathic scoliosis, which of the following best describes the structural relationship between the apical vertebra and the rib hump?
Explanation
Question 69
A 16-year-old male gymnast complains of chronic lower back pain. Radiographs show a grade I spondylolisthesis at L5-S1. What radiographic spinopelvic parameter is most strongly correlated with the risk of progression in isthmic spondylolisthesis?
Explanation
Question 70
A 50-year-old man presents with severe neck pain radiating down his right arm. Neurologic examination reveals weakness in triceps extension and wrist flexion, along with a diminished triceps reflex. He also has numbness over his middle finger. Which of the following nerve roots is most likely compressed?
Explanation
Question 71
A 78-year-old man with severe chronic obstructive pulmonary disease and congestive heart failure sustains a displaced Type II odontoid fracture after a low-energy fall. He is deemed a high-risk surgical candidate. What is the most appropriate initial management?
Explanation
Question 72
A 60-year-old diabetic male presents with worsening back pain, fever, and progressive lower extremity weakness. MRI demonstrates a large ventral epidural abscess spanning L2 to L4 with cord compression. What is the most appropriate definitive surgical management?
Explanation
Question 73
A 14-year-old gymnast presents with persistent lower back pain exacerbated by extension. Radiographs confirm a Grade 1 isthmic spondylolisthesis at L5-S1. If this patient were to develop a radicular neurologic deficit, which nerve root is most commonly affected?
Explanation
Question 74
A 65-year-old woman is planning to undergo corrective surgery for a symptomatic adult spinal deformity. Her preoperative radiographs demonstrate a pelvic incidence (PI) of 60 degrees. To achieve optimal spino-pelvic alignment and minimize adjacent segment disease, the target postoperative lumbar lordosis (LL) should be within how many degrees of her PI?
Explanation
Question 75
A 45-year-old man with ankylosing spondylitis presents after a minor motor vehicle collision. A non-contrast CT shows a highly displaced fracture through the C5-C6 disc space extending through the posterior elements.
Which of the following is the most significant acute risk associated with patient positioning and transport?

Explanation
Question 76
A 58-year-old female with breast cancer presents with back pain. MRI shows a lytic metastasis at T8. According to the Spinal Instability Neoplastic Score (SINS), which of the following clinical or radiographic features contributes most strongly to a higher score (indicating instability)?
Explanation
Question 77
A 70-year-old man with severe cervical spondylosis falls and strikes his chin. He develops bilateral upper extremity weakness that is far worse than his lower extremity weakness. Which spinal tract is predominantly responsible for this disproportionate motor deficit?
Explanation
Question 78
A 62-year-old male presents with severe myelopathy. Imaging reveals dense ossification along the posterior margin of the C3-C6 vertebral bodies, consistent with OPLL.
If an anterior surgical approach (corpectomy) is selected, what is the most common and feared intraoperative complication specific to this pathology?

Explanation
Question 79
A 68-year-old man reports bilateral calf pain after walking two blocks. The pain is rapidly relieved when he leans forward on a shopping cart. Which of the following findings most reliably differentiates this neurogenic claudication from vascular claudication?
Explanation
Question 80
A 24-year-old man presents after a high-speed motor vehicle collision. Radiographs demonstrate a Type II traumatic spondylolisthesis of the axis (Hangman's fracture).
What is the classic mechanism of injury for the initial pars interarticularis fracture in this scenario?
Explanation
Question 81
A 35-year-old construction worker sustains an L1 fracture with 50% canal compromise and 25 degrees of kyphosis after a fall. Neurologic exam is normal. According to the Thoracolumbar Injury Classification and Severity (TLICS) score, how many points are assigned specifically for the burst morphology of this fracture?
Explanation
Question 82
A 42-year-old woman presents with sudden onset severe low back pain, bilateral sciatica, perineal numbness, and difficulty initiating micturition (post-void residual is 350 mL). MRI confirms a massive L4-L5 central disc herniation. What is the most appropriate management?
Explanation
Question 83
A 15-year-old boy presents with a progressive thoracic kyphosis of 55 degrees. Imaging is evaluated for Scheuermann's kyphosis.
To meet the classic Sorensen criteria, what is the minimum degree of anterior wedging required in each of three consecutive vertebrae?
Explanation
Question 84
A 48-year-old woman undergoes a right-sided C5-C6 anterior cervical discectomy and fusion (ACDF). Postoperatively, she exhibits significant hoarseness and a weak voice. Laryngoscopy confirms unilateral vocal cord paralysis. Injury to which of the following structures is responsible?
Explanation
Question 85
A 65-year-old man presents with progressive gait clumsiness and deteriorating hand dexterity. Examination reveals a positive Hoffman's sign bilaterally and hyperreflexia in the lower extremities, but diminished biceps reflexes bilaterally. What is the most likely location of the primary pathology?
Explanation
Question 86
An 82-year-old woman falls and presents with neck pain. The radiograph shows a displaced Type II odontoid fracture. She has significant medical comorbidities (Charlson Comorbidity Index of 6) and no neurologic deficit. What is the most appropriate initial management?
Explanation
Question 87
A 54-year-old intravenous drug user presents with severe lower back pain, a low-grade fever, and new-onset urinary retention. What is the most sensitive imaging modality and expected elevated laboratory marker to confirm the suspected diagnosis?
Explanation
Question 88
A 12-year-old premenarchal female presents with a right thoracic curve measuring 48 degrees on a standing PA radiograph. She is Risser 0 and has a Sanders skeletal maturity stage of 2. What is the most appropriate management?
Explanation
Question 89
A 68-year-old man complains of bilateral calf pain and heaviness that occurs after walking two blocks. Which of the following historical factors is most specific for neurogenic claudication rather than vascular claudication?
Explanation
Question 90
A 15-year-old male gymnast presents with mechanical low back pain. Radiographs reveal a Grade 1 slip at L5-S1. What is the anatomic location of the defect causing this specific type of spondylolisthesis?
Explanation
Question 91
A 60-year-old diabetic male undergoes a lumbar microdiscectomy. Three weeks later, he presents with severe, unremitting back pain and elevated inflammatory markers. An MRI shows fluid in the disc space with endplate enhancement. What is the most likely causative organism?
Explanation
Question 92
A 72-year-old man with known cervical spondylosis sustains a hyperextension injury in a motor vehicle accident. He presents with 2/5 motor strength in his upper extremities and 4/5 motor strength in his lower extremities. What spinal cord injury syndrome does this represent?
Explanation
Question 93
When evaluating an adult patient for spinal deformity correction, achieving spinopelvic harmony is a primary goal. To minimize the risk of adjacent segment disease and mechanical failure, the lumbar lordosis (LL) should ideally be matched to within 10 degrees of which specific pelvic parameter?
Explanation
Question 94
A 45-year-old man presents to the emergency department with acute urinary retention, saddle anesthesia, and bilateral lower extremity weakness following a heavy lifting event. What is the most consistent early clinical finding in cauda equina syndrome?
Explanation
Question 95
A 34-year-old man is involved in a high-speed MVC. Imaging shows a bilateral pars interarticularis fracture of C2 with >3 mm of translation and severe angulation. This represents a Levine-Edwards Type II fracture. What is the primary mechanism of injury for this fracture pattern?
Explanation
Question 96
A 50-year-old woman presents with numbness in her right ring and small fingers, along with weakness in hand grip. Which of the following physical examination findings would best differentiate a C8 radiculopathy from cubital tunnel syndrome?
Explanation
Question 97
A 22-year-old man was wearing a lap belt during a head-on collision. Radiographs demonstrate a flexion-distraction injury (Chance fracture) through the L2 vertebral body and posterior elements. Which of the following concomitant injuries must be carefully ruled out?
Explanation
Question 98
A 78-year-old woman with a history of severe osteoporosis presents with acute-onset, severe mid-back pain after coughing. MRI confirms an acute T11 compression fracture without posterior wall involvement or neurologic deficit. She has failed 6 weeks of aggressive conservative management including bracing and analgesics. What is the most appropriate next step?
Explanation
Question 99
A 42-year-old man develops acute, severe anterior thigh pain and weakness in knee extension. MRI of the lumbar spine reveals a far-lateral (extraforaminal) disc herniation at the L4-L5 level. Which nerve root is most likely compressed?
Explanation
Question 100
A 65-year-old woman with long-standing rheumatoid arthritis presents with neck pain and mild myelopathic signs. Flexion-extension radiographs demonstrate an atlantodens interval (ADI) of 11 mm. What is the most critical radiographic parameter to assess the true space available for the spinal cord?
Explanation
None
