ABOS Part I & AAOS OITE Orthopedic Review: Hand Surgery, Masses, & Pediatric Elbow Fractures | Part 22220
Key Takeaway
This ABOS Part I Orthopedic Review module offers 32 advanced multiple-choice questions mirroring ABOS Part I and AAOS OITE exams. It covers critical topics in hand surgery, including lumbrical plus deformity and benign hand masses, alongside pediatric lateral condyle fractures, their diagnosis, and management, providing a comprehensive study resource.
ABOS Part I & AAOS OITE Orthopedic Review: Hand Surgery, Masses, & Pediatric Elbow Fractures | Part 22220
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 32-year-old carpenter presents with progressive difficulty making a full fist with his right ring finger, particularly when attempting to grasp small objects. He reports a history of a 'Jersey finger' injury to the same digit 6 months prior, which was surgically repaired. On examination, when he attempts to actively flex his ring finger, his metacarpophalangeal (MCP) joint flexes, but his proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints paradoxically extend. Passive range of motion of the PIP and DIP joints is full. Based on the epidemiology and pathophysiology described in the case, which of the following is the MOST likely underlying mechanism for this patient's current deformity?
Explanation
Correct Answer: C
Explanation:
The patient's presentation of a 'Jersey finger' injury (avulsion of the FDP insertion) followed by paradoxical IP extension during attempted active flexion is a classic description of a lumbrical plus deformity. The case explicitly states that 'Avulsion of the FDP insertion (e.g., "Jersey Finger")' is a common scenario where 'the lumbrical muscle, which originates from the FDP, becomes functionally unopposed distally. Attempted FDP activation then primarily pulls on the lumbrical, leading to its paradoxical action.'
- Option A (Over-tensioning of the FDS tendon): While over-tensioning of flexor tendons can cause lumbrical plus, the case specifically mentions FDP repairs or grafts, or FDS to FDP transfers. An FDS plus deformity would typically involve isolated PIP flexion with inability to fully extend the PIP, not paradoxical IP extension.
- Option B (Adhesions between FDP and flexor sheath): Adhesions would restrict FDP glide and lead to a general loss of flexion, but not the paradoxical IP extension characteristic of lumbrical plus. The FDP would simply be unable to pull the distal phalanx.
- Option D (Rupture of the central slip): A central slip rupture results in a boutonnière deformity (PIP flexion, DIP hyperextension), which is a fixed deformity of the extensor mechanism, not a dynamic paradoxical extension during attempted flexion.
- Option E (Spasticity of interosseous muscles): While spasticity can contribute to intrinsic overactivity, the specific history of a 'Jersey finger' repair points more directly to the FDP-lumbrical imbalance. Interosseous muscle spasticity would typically cause a more generalized intrinsic contracture, not necessarily the specific lumbrical plus phenomenon.
Question 2
A 28-year-old concert pianist develops a lumbrical plus deformity in her left index finger following a flexor tendon repair. She is concerned about the impact on her career. A thorough understanding of the lumbrical muscles is crucial for her surgeon. Which of the following statements accurately describes the anatomical and functional characteristics of the lumbrical muscles?
Explanation
Correct Answer: C
Explanation:
The case provides a detailed description of lumbrical anatomy and action:
- Option C (Correct): The case states: 'The first and second lumbricals typically originate from the FDP tendons of the index and middle fingers, respectively, and are unipennate. The third and fourth lumbricals are bipennate, originating from adjacent FDP tendons... The first and second lumbricals are innervated by the median nerve. The third and fourth lumbricals are innervated by the ulnar nerve.' This option accurately combines these facts.
- Option A (Incorrect): Not all lumbricals are bipennate (1st and 2nd are unipennate), and they are not solely innervated by the median nerve (3rd and 4th by ulnar nerve).
- Option B (Incorrect): Lumbricals originate from the radial side of the FDP tendons, not FDS tendons. They insert into the radial lateral band of the extensor apparatus and the base of the proximal phalanx, not directly into the central slip.
- Option D (Incorrect): The primary actions of the lumbricals are 'Flexion of the Metacarpophalangeal (MCP) joints' and 'Extension of the Interphalangeal (IP) joints' (the "intrinsic plus" position), not the reverse.
- Option E (Incorrect): Lumbricals pass volar to the deep transverse metacarpal ligament, then extend dorsally to insert into the lateral bands.
Question 3
A 55-year-old patient presents with a lumbrical plus deformity of the middle finger following a complex flexor tendon reconstruction. The surgeon explains that the deformity results from a disruption of normal force transmission. Which of the following statements best describes the biomechanical pathophysiology of this condition?
Explanation
Correct Answer: C
Explanation:
The case provides a clear explanation of the biomechanics of lumbrical plus deformity:
- Option C (Correct): The case states: 'When the FDP tendon is abnormally taut... The primary FDP muscle belly contracts, but the excessive tension on the tendon restricts its distal excursion... Instead of transmitting force primarily to the distal phalanx, the contracting FDP tendon pulls predominantly on the origin of the lumbrical muscle. This effectively shortens the lumbrical and intensifies its pull... The now over-active lumbrical... flexes the MCP joint while simultaneously extending the PIP and DIP joints through its connection to the lateral bands and terminal tendon.' This perfectly matches the description.
- Option A (Incorrect): An over-lengthened FDP would result in weakness of DIP flexion, not paradoxical IP extension. The problem is FDP tightness, not looseness.
- Option B (Incorrect): The lumbrical muscle is overactive, not paralyzed, in lumbrical plus deformity.
- Option D (Incorrect): Adhesions of the EDC tendon would primarily affect MCP and PIP extension, not cause paradoxical IP extension during attempted flexion.
- Option E (Incorrect): Rupture of the deep transverse metacarpal ligament would lead to splaying of the fingers and potentially subluxation of the MCP joints, but it does not directly explain the paradoxical IP extension characteristic of lumbrical plus. The lumbrical passes volar to this ligament.
Question 4
A 40-year-old patient presents with a lumbrical plus deformity of the ring finger, significantly impacting her ability to perform daily tasks. After a trial of hand therapy, the deformity persists. The surgeon is considering surgical intervention. According to the case, which of the following is an absolute contraindication to surgical intervention for this condition?
Explanation
Correct Answer: D
Explanation:
The case outlines both indications and contraindications for surgical intervention. Under 'Contraindications for Surgical Intervention', it explicitly states: 'Any active infection in the surgical field is an absolute contraindication to elective hand surgery until adequately treated.'
- Option A (Mild, intermittent pain): This falls under non-operative management criteria ('Mild to moderate pain managed with NSAIDs, activity modification, splinting') and is not an absolute contraindication.
- Option B (Patient's desire for non-invasive approach): While patient preference is a factor, it's listed as a reason for non-operative management, not an absolute contraindication. The question asks for an absolute contraindication.
- Option C (Dynamic deformity that improves with active-assistive exercises): This describes a mild deformity that is likely to respond to conservative management and would typically not warrant surgery, but it is not an absolute contraindication if surgery were otherwise indicated.
- Option E (Unrealistic patient expectations): This is listed as a contraindication, but it is generally considered a relative contraindication that can be addressed through thorough patient education, rather than an absolute one that completely precludes surgery.
Question 5
A 60-year-old patient is scheduled for surgical correction of a lumbrical plus deformity in the small finger. During pre-operative planning, the surgeon emphasizes the importance of a detailed history and physical examination. Which of the following findings on physical examination is considered the hallmark of lumbrical plus deformity?
Explanation
Correct Answer: C
Explanation:
The case consistently highlights the defining clinical feature of lumbrical plus deformity:
- Option C (Correct): The 'Introduction & Epidemiology' section defines the condition as 'paradoxical extension of the interphalangeal (IP) joints during attempted active flexion of the involved digit.' The 'Physical Examination' section further reinforces this: 'The hallmark lumbrical plus deformity will manifest as MCP flexion with paradoxical PIP and DIP extension.'
- Option A (Fixed flexion contracture of the PIP joint with hyperextension of the DIP joint): This describes a boutonnière deformity, which is a fixed extensor mechanism issue, not the dynamic paradoxical extension of lumbrical plus.
- Option B (Inability to actively extend the MCP joint while maintaining IP joint flexion): This describes a loss of intrinsic function (e.g., intrinsic minus hand), which is the opposite of the lumbrical plus deformity where the lumbricals are overactive.
- Option D (Isolated inability to flex the DIP joint): This would indicate a complete FDP rupture or avulsion without the lumbrical plus component, or a severe adhesion of the FDP distal to the lumbrical origin, but not the paradoxical IP extension.
- Option E (Pain and swelling localized to the A1 pulley region): This is characteristic of trigger finger, not lumbrical plus deformity.
Question 6
A 48-year-old patient is undergoing surgical correction for a lumbrical plus deformity of the middle finger. The surgeon has made a Brunner zig-zag incision and meticulously protected the digital neurovascular bundles. After exposing the flexor sheath, the next critical step is to identify the lumbrical muscle. Which of the following accurately describes the typical anatomical location and appearance of the lumbrical muscle in relation to the flexor tendons?
Explanation
Correct Answer: B
Explanation:
The 'Detailed Surgical Approach / Technique' section provides specific guidance on identifying the lumbrical:
- Option B (Correct): The case states: 'Identify the lumbrical muscle. It typically originates from the radial side of the FDP tendon in the palm, distal to the carpometacarpal joint line, and runs distally along the radial side of the FDP tendon. It appears as a reddish-brown, often fusiform, muscle belly transitioning into a thin tendon that inserts into the extensor mechanism.' This option precisely matches the description.
- Option A (Incorrect): Lumbricals originate from the FDP, not FDS, and from the radial side, not ulnar. They are muscular proximally, not purely tendinous.
- Option C (Incorrect): Lumbricals are part of the intrinsic muscles, originating from the FDP, not the central slip. They run volar to the deep transverse metacarpal ligament, then dorsally to the extensor mechanism, not volar to the flexor tendons throughout.
- Option D (Incorrect): Lumbricals are not deep to the FDP tendon; they originate from its radial side. Their insertion is into the extensor mechanism, not the A2 pulley.
- Option E (Incorrect): Lumbricals do not originate from the flexor retinaculum; that is the origin for some thenar and hypothenar muscles. Their insertion is into the extensor mechanism, not directly into the base of the middle phalanx (that's the central slip).
Question 7
A 35-year-old patient undergoes a lumbrical tenotomy for a lumbrical plus deformity of the ring finger. During the immediate post-operative period (Day 0-7), the hand therapist applies a dorsal blocking splint. Which of the following positions is typically maintained by this splint, and what is its primary purpose?
Explanation
Correct Answer: B
Explanation:
The 'Post-Operative Rehabilitation Protocols' section details the immediate post-operative management:
- Option B (Correct): The case states: 'A dorsal blocking splint is typically applied. The wrist is positioned in slight flexion (e.g., 20-30 degrees), the MCP joints are in moderate flexion (e.g., 70-90 degrees), and the IP joints are in full extension. This "intrinsic plus" position helps to prevent flexion contractures of the MCPs and facilitates IP flexion once active motion begins.' This option accurately describes both the position and its purpose.
- Option A (Incorrect): Full wrist extension and MCP extension are not the typical positions for a dorsal blocking splint in this context. The goal is to prevent MCP extension contracture and facilitate IP flexion.
- Option C (Incorrect): While protection is a goal, the specific MCP flexion angle is typically greater (70-90 degrees), and the primary purpose is not just to protect the lumbrical repair (which is a tenotomy, not a repair needing protection from tension).
- Option D (Incorrect): Full wrist flexion would put excessive tension on the extensor tendons and is not a functional position. Full IP flexion is also not the initial splinting position.
- Option E (Incorrect): Slight wrist extension and IP flexion are not the typical initial splinting positions. Early strengthening of lumbricals is not a goal after a tenotomy.
Question 8
A 50-year-old patient presents with a recurrent lumbrical plus deformity after a previous lumbrical tenotomy. Intraoperative assessment confirms significant over-tensioning of the flexor digitorum profundus (FDP) tendon as the primary underlying cause. The surgeon decides to perform an FDP lengthening procedure. Which of the following statements accurately describes this technique and its implications?
Explanation
Correct Answer: C
Explanation:
The case provides specific details regarding FDP lengthening:
- Option C (Correct): The case states: 'Expose the FDP tendon well, typically in the mid-palmar or forearm region to gain sufficient length for a Z-plasty... Perform a Z-lengthening of the FDP tendon... The ideal tension is achieved when the affected digit can passively extend completely while maintaining a normal resting cascade, and can actively flex without paradoxical extension. A useful clinical test is to ensure the repaired FDP tendon allows the digit to passively extend fully without causing adjacent digits to flex prematurely (quadriga effect).' The image provided could represent such a Z-lengthening.
- Option A (Incorrect): The case states that 'simple lumbrical tenotomy... is the most effective and least morbid surgical intervention for established lumbrical plus deformity.' FDP lengthening is 'generally reserved for cases where... The primary etiology is clearly demonstrated to be iatrogenic overtensioning of the FDP tendon... or a simple lumbrical tenotomy has failed.'
- Option B (Incorrect): FDP lengthening is typically performed via a Z-plasty (longitudinal incision with a Z-shape or step-cut), not a simple transverse incision with a gap, which would be less stable and prone to gapping.
- Option D (Incorrect): The case explicitly states that FDP lengthening is 'More extensive surgery, longer recovery, higher risk of adhesions, and potential for flexor weakness if over-lengthened.' This contradicts the statement.
- Option E (Incorrect): The ideal tension ensures the digit can passively extend completely without causing adjacent digits to flex prematurely (quadriga effect). The option incorrectly states that it allows adjacent digits to flex prematurely.
Question 9
A 22-year-old athlete undergoes surgical correction of a lumbrical plus deformity. Post-operatively, he develops persistent, disproportionate pain, swelling, skin color changes, and allodynia in the affected hand. These symptoms are suggestive of Complex Regional Pain Syndrome (CRPS). According to the case, what is the MOST appropriate initial management strategy for CRPS?
Explanation
Correct Answer: C
Explanation:
The 'Complications & Management' section addresses CRPS:
- Option C (Correct): The case states for CRPS: 'Early recognition is key. Multimodal pain management (medications, sympathetic blocks), aggressive hand therapy focusing on desensitization and active motion, psychological support.' This option accurately reflects the recommended approach.
- Option A (Incorrect): While nerve entrapment can cause pain, CRPS is a distinct syndrome. Immediate surgical re-exploration is not the initial management for CRPS, which is a diagnosis based on clinical criteria.
- Option B (Incorrect): Aggressive passive range of motion can exacerbate CRPS symptoms and is generally contraindicated in the early stages. Therapy should focus on gentle, active motion and desensitization.
- Option D (Incorrect): While corticosteroids might be used in some pain syndromes, they are not the primary or sole initial management for CRPS, which requires a broader, multimodal approach.
- Option E (Incorrect): Strict immobilization is generally detrimental in CRPS, as it can worsen stiffness and pain. Early, gentle active motion is preferred.
Question 10
A 42-year-old patient is recovering from a lumbrical tenotomy for a lumbrical plus deformity. During Phase II (Weeks 1-3) of rehabilitation, the hand therapist initiates several interventions. Which of the following is a key component of rehabilitation during this early mobilization phase?
Explanation
Correct Answer: C
Explanation:
The 'Post-Operative Rehabilitation Protocols' section details Phase II (Early Mobilization):
- Option C (Correct): The case states: 'Initiate gentle, active flexion and extension exercises for the affected MCP, PIP, and DIP joints. The goal is full, coordinated motion without paradoxical extension. Focus on isolated FDP and FDS gliding exercises to prevent adhesions and improve tendon excursion.' This is a core component of early mobilization.
- Option A (Incorrect): Heavy strengthening exercises are introduced in Phase III (Weeks 4-6), not Phase II.
- Option B (Incorrect): Splinting is continued in Phase II ('Continue dorsal blocking splint or a custom static-progressive splint between exercise sessions and at night'), not completely ceased.
- Option D (Incorrect): Surgical capsulotomy is a salvage strategy for severe, fixed contractures that have failed conservative management, not a routine part of Phase II rehabilitation.
- Option E (Incorrect): Strict immobilization is characteristic of Phase I, but Phase II emphasizes early mobilization and controlled motion, not strict rest.
Question 11
A hand surgeon is reviewing the literature on lumbrical plus deformity to prepare for a complex case. The literature consistently emphasizes the standard surgical approach and its rationale. Which of the following statements accurately reflects the consensus in current hand surgery literature regarding the primary surgical intervention for established lumbrical plus deformity?
Explanation
Correct Answer: C
Explanation:
The 'Summary of Key Literature / Guidelines' section clearly outlines the standard surgical approach:
- Option C (Correct): The case states: 'The overwhelming consensus in current hand surgery literature is that simple lumbrical tenotomy at its origin from the FDP tendon is the most effective and least morbid surgical intervention for established lumbrical plus deformity... The loss of a single lumbrical's specific function is generally well-compensated by other intrinsic muscles, and the functional gain from improved FDP excursion is significant.'
- Option A (Incorrect): FDP lengthening is described as 'a more involved procedure and is generally reserved for cases where... The primary etiology is clearly demonstrated to be iatrogenic overtensioning of the FDP tendon... or a simple lumbrical tenotomy has failed.' It is not the preferred initial procedure for all cases.
- Option B (Incorrect): Lumbrical advancement/recession is described as 'Less commonly performed as the primary solution for established lumbrical plus' and 'Technically more demanding, higher risk of recurrence.'
- Option D (Incorrect): EDC tendon transfer to the FDP is not mentioned as a standard treatment for lumbrical plus deformity.
- Option E (Incorrect): Arthrodesis is a joint fusion procedure, typically reserved for severe, painful arthritis or instability, not for correcting a dynamic tendon imbalance like lumbrical plus. The goal is to restore motion, not eliminate it.
Question 12
Question 1
A 52-year-old right-hand dominant carpenter presents with a firm, mobile, non-tender mass on the volar aspect of his left wrist, which has been slowly growing over the past year. He reports mild discomfort with repetitive wrist flexion and extension, but no neurological symptoms. Physical examination confirms a 2x1.5 cm mass, distinct from tendons, with no overlying skin changes. Imaging (ultrasound and MRI) suggests a benign soft tissue tumor, likely a lipoma or giant cell tumor of the tendon sheath, with close proximity to the radial artery and superficial branch of the radial nerve. The patient is considering surgical excision due to increasing mechanical interference with his work. Based on the principles outlined in the case, why is a 'wide local excision' (WLE) approach generally considered detrimental for this type of benign hand mass?
Explanation
Correct Answer: C
The case explicitly states that 'The compact nature of critical neurovascular structures, tendons, and joint capsules within the hand means that indiscriminate 'wide' margins can lead to significant iatrogenic morbidity, including nerve injury, vascular compromise, tendon rupture, joint stiffness, and profound functional deficits.' For benign hand masses, the objective is precise, en bloc excision with meticulous preservation of adjacent healthy, functional structures, rather than the removal of a broad cuff of uninvolved tissue.
- Option A is incorrect. There is no evidence that WLE increases the risk of malignant transformation of benign lesions. The concern with WLE in the hand is iatrogenic damage, not oncologic transformation.
- Option B is incorrect. For benign lesions like GCTTS, recurrence is primarily due to incomplete excision, not the width of the margin of healthy tissue removed. WLE, by damaging surrounding structures, might even complicate subsequent re-excision if recurrence occurs.
- Option D is incorrect. WLE, by definition, aims for wide margins. The issue in the hand is that these 'wide' margins are often unnecessary for benign lesions and cause more harm than good due to the dense packing of vital structures. For benign lesions, 'tumor-free margins immediately adjacent to the lesion' are sufficient, not wide margins of healthy tissue.
- Option E is incorrect. The principle against WLE applies to most benign hand masses, whether cystic (e.g., ganglion cysts) or solid (e.g., lipomas, GCTTS). The commonality is their benign nature and the need for functional preservation.
Question 13
Question 2
A 38-year-old patient presents with a 1.5 cm, ill-defined, deep-seated mass in the palm, causing intermittent pain and mild weakness in grip strength. On physical examination, the mass is firm and appears fixed to deeper structures. There is no transillumination. Plain radiographs are unremarkable. Given the diagnostic uncertainty and the mass's deep location and potential relationship to critical structures, which advanced imaging modality is considered the 'gold standard' for detailed soft tissue characterization, defining the extent of the lesion, and its relationship to critical neurovascular bundles and tendons?
Explanation
Correct Answer: C
The case states that 'Magnetic Resonance Imaging (MRI): The gold standard for detailed soft tissue characterization, defining the extent of the lesion, and its relationship to critical structures. Superior for distinguishing between benign and malignant features (e.g., T1/T2 signal characteristics, enhancement patterns, presence of perilesional edema). Crucial for larger, deeper, or diagnostically challenging masses.' Given the deep, ill-defined nature and diagnostic uncertainty, MRI is the most appropriate choice.
- Option A (CT) is incorrect. CT is less frequently used for primary soft tissue masses unless bony involvement is a major concern. It provides less soft tissue detail than MRI.
- Option B (Ultrasound) is incorrect. While ultrasound is an excellent first-line advanced imaging for differentiating cystic from solid lesions and assessing neurovascular proximity, MRI offers superior detailed soft tissue characterization and is the gold standard for defining the full extent and relationship to critical structures, especially for deeper or diagnostically challenging masses.
- Option D (Arthrography) is incorrect. Arthrography is primarily used to evaluate joint pathology, particularly tears in ligaments or cartilage, and is not the primary imaging modality for characterizing a soft tissue mass.
- Option E (Bone Scintigraphy) is incorrect. Bone scintigraphy (bone scan) is used to detect increased metabolic activity in bone, such as infections, fractures, or tumors, but it does not provide detailed soft tissue characterization.
Question 14
Question 3
A 68-year-old patient presents with a rapidly growing, firm, and fixed mass on the ulnar side of the palm, which has developed over the past 3 months. The patient reports increasing pain and paresthesias in the small finger. MRI reveals a 3 cm mass with irregular borders, heterogeneous enhancement, and evidence of local infiltration into adjacent soft tissues. There is a high clinical suspicion for malignancy. Based on the case's guidelines for suspicious masses, what is the *most appropriate* next step in management?
Explanation
Correct Answer: C
The case explicitly states: 'For highly suspicious masses (rapid growth, deep location, large size, concerning MRI features), an incisional biopsy (rather than initial wide local excision) performed by an experienced orthopedic oncologist or hand surgeon is often warranted. This allows for definitive histological diagnosis and appropriate oncologic staging before definitive wide resection, if malignancy is confirmed. A poorly performed excisional biopsy (especially 'wide') can compromise subsequent oncologic resection and limb salvage.'
- Option A is incorrect. Initial wide local excision is generally contraindicated as a diagnostic maneuver for a suspected malignancy in the hand, as it can compromise subsequent definitive oncologic resection and limb salvage if the diagnosis is confirmed.
- Option B is incorrect. Given the rapid growth, fixed nature, and concerning MRI features, observation is inappropriate and could delay critical treatment for a potential malignancy.
- Option D is incorrect. While FNA can be useful for cystic lesions or to confirm benignity, the case notes it 'has limitations in solid tumors' and for highly suspicious solid masses, an incisional biopsy provides more tissue for comprehensive histological analysis and definitive diagnosis.
- Option E is incorrect. Radiation therapy is a treatment modality, not a diagnostic step. Definitive histological diagnosis via biopsy is essential before initiating oncologic treatment.
Question 15
Question 4
A 45-year-old patient is undergoing surgical excision of a dorsal wrist ganglion. The surgeon is meticulously dissecting through the subcutaneous tissue and extensor retinaculum. The case highlights the importance of identifying and protecting vulnerable neurovascular structures. Which of the following nerves is *most commonly* at risk of iatrogenic injury during the excision of a dorsal wrist ganglion?
Explanation
Correct Answer: C
The case specifically mentions, 'For instance, volar wrist masses (e.g., ganglion cysts) often lie immediately adjacent to the radial artery and superficial branch of the radial nerve, while masses in the ulnar side of the palm may involve branches of the ulnar nerve.' More directly, under 'Specific Techniques for Common Hand Masses' for 'Dorsal Wrist Ganglion,' it states: 'Identify and protect the dorsal sensory branch of the radial nerve and its branches, which are highly variable and vulnerable.'
- Option A (Median nerve) is incorrect. The median nerve is located volarly and centrally in the wrist and palm, not typically in the dorsal wrist surgical field for a ganglion.
- Option B (Ulnar nerve) is incorrect. The ulnar nerve is located on the ulnar side of the wrist and hand, primarily volarly, and is not the most vulnerable nerve during dorsal wrist ganglion excision.
- Option D (Anterior interosseous nerve) is incorrect. The anterior interosseous nerve is a deep motor branch of the median nerve in the forearm and is not typically at risk during a dorsal wrist approach.
- Option E (Posterior interosseous nerve) is incorrect. While the posterior interosseous nerve is dorsal, it is a deep motor nerve in the forearm and wrist, and its sensory component is minimal. The superficial dorsal sensory branch of the radial nerve is much more superficially located and directly in the surgical field for dorsal wrist ganglions.
Question 16
Question 5
A 40-year-old patient has undergone precise excision of a giant cell tumor of the tendon sheath (GCTTS) from the flexor tendon sheath of the index finger. The surgeon meticulously removed the tumor, ensuring complete en bloc excision while preserving the tendon and A2 pulley. Post-operatively, the patient is concerned about stiffness. Based on the rehabilitation protocols outlined in the case, what is the *most crucial* principle to prevent adhesions and optimize long-term function in this patient?
Explanation
Correct Answer: C
The case emphasizes: 'Early Mobilization: This is the most crucial principle in hand surgery to prevent adhesions and stiffness. Unless there is a specific reason for immobilization (e.g., tendon repair, joint instability), active range of motion (AROM) exercises are initiated as soon as pain allows, often within the first few days post-surgery.' For flexor tendon sheath excisions, it specifically states: 'Crucial to initiate early AROM of the affected digit to prevent flexor tendon adhesions and subsequent triggering or loss of motion.'
- Option A is incorrect. Prolonged immobilization is generally detrimental in hand surgery, leading to stiffness and adhesions, especially after flexor tendon sheath surgery where tendon glide is critical.
- Option B is incorrect. While strengthening is part of rehabilitation, it is introduced gradually, typically after 3-4 weeks, once initial healing is sufficient and ROM goals are met. Immediate aggressive strengthening could jeopardize healing.
- Option D is incorrect. Scar management, including gentle scar massage, is recommended once sutures are removed and the wound is fully closed to improve pliability and prevent adhesions.
- Option E is incorrect. While adequate pain management is vital, the goal is to control pain to allow participation in therapy, not necessarily to eliminate all pain with high-dose opioids, which carry their own risks.
Question 17
Question 6
A 28-year-old patient presents with a recurrent dorsal wrist ganglion 8 months after undergoing surgical excision. The patient reports that the mass reappeared in the same location and is now causing similar intermittent discomfort. During the initial surgery, the ganglion was excised, but the patient is unsure if the stalk was completely removed. Based on the case, what is the approximate recurrence rate for dorsal wrist ganglions after surgical excision, and what is a common reason for this recurrence?
Explanation
Correct Answer: C
The case states under 'Complications & Management' that 'Ganglion cysts (especially dorsal wrist) have a recurrence rate of 10-30%, often due to incomplete excision of the stalk or underlying wrist joint pathology.' It further reinforces this in the 'Summary of Key Literature / Guidelines' section.
- Option A is incorrect. The recurrence rate is higher than 5%, and infection is a separate complication, not the primary cause of recurrence for ganglions.
- Option B is incorrect. While immobilization can cause stiffness, it is not the primary reason for ganglion recurrence, and the recurrence rate is higher than 5-10%.
- Option D is incorrect. The recurrence rate is not typically as high as 30-50%, and while patient compliance is important for overall outcome, it's not cited as the primary reason for ganglion recurrence.
- Option E is incorrect. Ganglion cysts are benign. Recurrence does not indicate malignant transformation.
Question 18
Question 7
A 60-year-old patient is undergoing excision of a giant cell tumor of the tendon sheath (GCTTS) located in the palm, intimately associated with the digital neurovascular bundle and flexor tendon. The surgeon is aware of the high recurrence rate of GCTTS if incompletely removed. Based on the detailed surgical approach described in the case, what is the *most critical* aspect of the surgical technique for GCTTS excision to minimize recurrence while preserving function?
Explanation
Correct Answer: C
The case states under 'Specific Techniques for Common Hand Masses' for GCTTS: 'Complete en bloc excision is critical to minimize recurrence. Care must be taken to avoid stripping the healthy tendon surface, which can lead to adhesions. If the tumor infiltrates a nerve fascicle, a decision must be made whether to resect the involved fascicle or carefully debulk. Nerve resection should be avoided if possible.' It also notes: 'The literature consistently emphasizes that the primary risk factor for recurrence is incomplete excision. Given the lobulated and often infiltrative nature of GCTTS, meticulous dissection and complete removal... are critical.'
- Option A is incorrect. The case explicitly states: 'There is no role for wide local excision with substantial normal tissue margins for GCTTS; the goal is tumor-free margins immediately adjacent to the lesion.' WLE would cause unacceptable morbidity in the hand.
- Option B is incorrect. While judicious blunt dissection can be used, the case recommends 'Sharp Dissection: Use a sharp scalpel or fine scissors for tissue separation. Blunt dissection should be used judiciously, particularly near critical structures, as it can cause traction injury to nerves.' Meticulous sharp dissection is often necessary.
- Option D is incorrect. Leaving a portion of the tumor, especially if it's infiltrative, is a primary cause of recurrence for GCTTS. While nerve preservation is paramount, the goal is complete removal, often requiring careful debulking around nerves rather than leaving gross tumor.
- Option E is incorrect. Post-operative radiation therapy is not a standard or immediate treatment for benign GCTTS and is not mentioned as a primary strategy to prevent recurrence in the case.
Question 19
Question 8
Three weeks after excision of a benign hand mass, a 42-year-old patient presents with severe, burning pain, allodynia (pain from non-painful stimuli), and disproportionate swelling and skin color changes (mottling) in the affected hand. The patient is reluctant to move the hand due to pain. Physical examination reveals increased warmth and tenderness, and limited active range of motion. This clinical presentation is most suggestive of which complication, and what is a key aspect of its management?
Explanation
Correct Answer: C
The clinical presentation of severe burning pain, allodynia, disproportionate swelling, and skin changes (mottling, warmth) is classic for Complex Regional Pain Syndrome (CRPS). The case describes CRPS as 'Rare (<1%), but devastating. More common after nerve injury or highly painful procedures.' For management, it states: 'Early recognition is key. Multidisciplinary approach involving pain management specialists, physical/occupational therapists, and psychological support. Sympathetic nerve blocks, neuromodulation, medications (gabapentinoids, tricyclic antidepressants). Vitamin C supplementation (500mg daily for 50 days) has shown some evidence in reducing CRPS risk.'
- Option A is incorrect. While infection can cause pain and swelling, the burning quality, allodynia, and disproportionate nature of the symptoms are more characteristic of CRPS.
- Option B is incorrect. Neuroma formation typically presents as a localized, sharp, shooting pain with percussion (Tinel's sign) at the site of nerve injury, not diffuse burning pain, allodynia, and widespread autonomic changes.
- Option D is incorrect. Tendon adhesions cause stiffness and restricted motion, but not the severe burning pain, allodynia, and autonomic changes seen in CRPS.
- Option E is incorrect. A hematoma would typically present as a localized, firm, tender swelling, often with ecchymosis, and would usually manifest earlier in the post-operative course. It would not typically cause allodynia or diffuse burning pain.
Question 20
Question 9
A hand surgeon is preparing to excise a small, deep-seated mass in the digital pulp, which is suspected to be an epidermal inclusion cyst. The area is densely packed with neurovascular structures. The case emphasizes specific tools and techniques for precise dissection. The use of surgical loupes (2.5x to 4.5x magnification) is highly recommended, if not mandatory, for all hand mass excisions primarily because it:
Explanation
Correct Answer: C
The case states under 'Patient Positioning and Setup': 'Magnification: Use of surgical loupes (2.5x to 4.5x magnification) is highly recommended, if not mandatory, for all hand mass excisions. This enhances visualization of small nerves, vessels, and the true margins of the mass, significantly reducing iatrogenic injury.'
- Option A is incorrect. While magnification can make dissection more efficient, its primary benefit is precision and safety, not necessarily a reduction in overall operative time, which can sometimes be longer due to meticulous dissection.
- Option B is incorrect. A bloodless field (achieved with a tourniquet) is still 'absolutely critical for meticulous dissection in the hand where small, vital structures are easily obscured by bleeding,' even with magnification. Magnification does not negate the need for a bloodless field.
- Option D is incorrect. Magnification allows for more precise dissection through smaller, well-planned incisions, rather than necessitating wider incisions. The goal is adequate exposure, not unnecessarily large incisions.
- Option E is incorrect. A pneumatic tourniquet is essential for a bloodless field, which is critical for hand surgery. Magnification complements, but does not replace, the need for a tourniquet.
Question 21
Question 10
A 30-year-old patient presents with a 1 cm, soft, mobile, non-tender subcutaneous mass in the thenar eminence. The mass has been present for several years and has not changed in size or caused any symptoms. Physical examination confirms a classic presentation of a benign lipoma. The patient is otherwise healthy and has no significant medical comorbidities. Based on the indications and contraindications for hand mass excision outlined in the case, what is the *most appropriate* initial management strategy for this patient?
Explanation
Correct Answer: C
The case clearly outlines 'Non-Operative Indications / Contraindications for Excision,' stating: 'Asymptomatic Mass: The vast majority of benign hand masses are asymptomatic. If the patient has no pain, functional impairment, or significant cosmetic concern, observation is the preferred initial management. Many benign masses (e.g., ganglion cysts) may spontaneously resolve or remain stable.' It also lists 'Clear Benign Diagnosis: If the diagnosis is unequivocally benign through clinical assessment and imaging (e.g., a classic dorsal wrist ganglion, a subcutaneous lipoma that is soft and mobile, an epidermal inclusion cyst with characteristic features) and the mass is asymptomatic or minimally symptomatic' as a non-operative indication.
- Option A is incorrect. Immediate surgical excision is not indicated for an asymptomatic, clearly benign mass.
- Option B is incorrect. An incisional biopsy is reserved for suspicious masses where malignancy is a concern. For a classic, asymptomatic lipoma, it is unnecessary.
- Option D is incorrect. Wide local excision is generally detrimental for benign hand masses and is not indicated for an asymptomatic lipoma. Lipomas do not undergo malignant transformation.
- Option E is incorrect. Lipomas are solid, fatty tumors, not cystic. Aspiration would not confirm a cystic nature and is not the appropriate diagnostic or management step for a solid, benign, asymptomatic lipoma.
Question 22
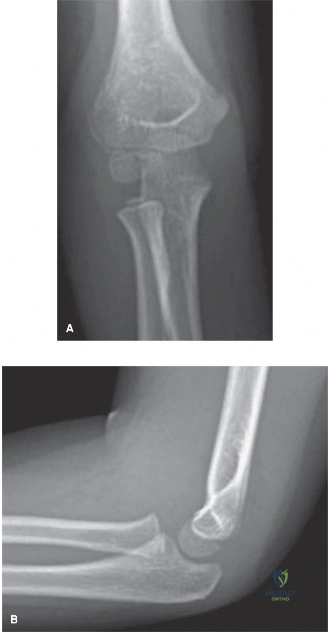
A 7-year-old male presents to the emergency department after falling from monkey bars onto an outstretched right hand. Clinical examination reveals marked diffuse swelling over the right elbow, predominantly on the lateral aspect, with significant tenderness over the lateral epicondyle. Active and passive range of motion are severely restricted and painful. Initial standard AP and lateral radiographs are equivocal for the extent of displacement and articular involvement of a suspected lateral condyle fracture. Given the high clinical suspicion, an additional radiograph is obtained, as shown below:
Which of the following statements best describes the utility of this specific radiographic view in this clinical scenario?
Explanation
Correct Answer: C
The image provided is an internal oblique radiograph of the elbow. As detailed in the teaching case, this view is crucial in pediatric elbow trauma, particularly for assessing lateral condyle fractures. It is obtained by internally rotating the arm 45 degrees, which places the lateral condyle in profile and removes the superimposition of the ulna and radial head. This specific projection is highly sensitive for detecting gap formation at the posterior aspect of the lateral metaphysis, often the first sign of displacement, and unequivocally demonstrates the true extent of the fracture line and any subtle displacement or rotation that might be missed on standard AP and lateral projections.
- Option A is incorrect: While supracondylar fractures are common, this view is not primarily for their assessment or neurovascular compromise, which is a clinical finding.
- Option B is incorrect: The internal oblique view is not specifically designed to visualize the olecranon fossa or diagnose olecranon fractures.
- Option D is incorrect: Medial epicondyle fractures are best assessed on standard AP and lateral views, sometimes with an external oblique view, but not typically the internal oblique. Ulnar nerve entrapment is a clinical diagnosis.
- Option E is incorrect: Radial head subluxation (nursemaid's elbow) is a clinical diagnosis, and while radial head dislocations can be seen on standard views, the internal oblique is not the primary view for this assessment.
Question 23
A 7-year-old male presents with a lateral condyle fracture of the humerus, confirmed on internal oblique radiographs. The fracture line extends from the lateral metaphysis, through the physis, and into the articular surface. The fracture fragment includes the entire capitellum and a portion of the lateral trochlear ridge. Based on the provided case information, which of the following classifications best describes this fracture type and its implications?
Explanation
Correct Answer: E
The case explicitly states that the internal oblique view unequivocally demonstrated a Salter-Harris Type IV fracture of the lateral condyle of the humerus. It further describes the fracture line as extending from the lateral metaphysis, through the physis, and into the articular surface. This definition perfectly matches Salter-Harris Type IV, which involves the metaphysis, physis, and epiphysis (articular surface). Lateral condyle fractures are inherently intra-articular and involve the physis, making Salter-Harris Type IV a common classification for these injuries.
- Option A is incorrect: While Milch Type I describes a fracture lateral to the trochlear groove, the primary Salter-Harris classification for a fracture extending into the articular surface is Type IV, not Type I. Milch Type I is also a Salter-Harris IV, but the question asks for the best description of the fracture type and its implications, and Salter-Harris IV directly describes the physeal and articular involvement.
- Option B is incorrect: Milch Type II describes a fracture extending into the apex of the trochlear groove, which is also typically a Salter-Harris Type IV (or II). However, the case specifically states Salter-Harris Type IV.
- Option C is incorrect: Salter-Harris Type II fractures involve the physis and metaphysis but spare the epiphysis and articular surface. This does not match the description of an intra-articular lateral condyle fracture.
- Option D is incorrect: Salter-Harris Type III fractures involve the physis and epiphysis (articular surface) but spare the metaphysis. While intra-articular, the case explicitly states the fracture extends from the metaphysis, making Type IV more accurate.
Question 24
A 9-year-old patient presents with a displaced lateral condyle fracture. During open reduction and internal fixation (ORIF), the surgeon is meticulously clearing the fracture hematoma and preparing for reduction. Which of the following surgical maneuvers carries the highest risk of avascular necrosis (AVN) of the capitellum?
Explanation
Correct Answer: C
The teaching case explicitly highlights the critical vascular anatomy of the lateral condyle: 'The capitellum receives its primary blood supply from posterior end-arteries that enter the non-articular posterior aspect of the lateral condyle. There is no significant collateral circulation. Consequently, aggressive posterior soft tissue dissection during open reduction risks devascularizing the fragment, leading to avascular necrosis (AVN) of the capitellum.' Therefore, aggressively stripping soft tissue attachments from the posterior aspect of the lateral condyle is the maneuver with the highest risk of AVN.
- Option A is incorrect: The direct lateral incision utilizing the internervous plane between the anconeus and extensor carpi ulnaris (Kocher interval) is the standard and safe approach for lateral condyle fractures.
- Option B is incorrect: Gentle manipulation of the metaphyseal fragment with instruments like a dental pick or skin hook is a standard technique for achieving reduction and does not inherently risk AVN if performed carefully.
- Option D is incorrect: Fixation with two divergent smooth K-wires achieving bicortical purchase is the recommended and biomechanically stable method of internal fixation, not a cause of AVN.
- Option E is incorrect: Meticulous repair of the joint capsule and extensor aponeurosis is a crucial step to prevent late soft tissue prominence and does not contribute to AVN.
Question 25
A 6-year-old child presents with a lateral condyle fracture. Radiographs confirm a fracture with 3 mm of displacement and an intact articular hinge. According to the Jakob classification, this fracture would be categorized as Stage 2. Based on the case information, what is the most appropriate initial management strategy?
Explanation
Correct Answer: C
The teaching case outlines the Jakob classification and its treatment implications. Jakob Stage 2 fractures are defined as displaced fractures (>2 mm) with an intact articular hinge, but the metaphyseal fragment is displaced laterally. The text states: 'While closed reduction and percutaneous pinning can be attempted for Jakob Stage 2 fractures (2-4 mm displacement with an intact hinge), open reduction and internal fixation (ORIF) is the gold standard for any fracture with a disrupted articular hinge or rotation (Jakob Stage 3).' It also notes that 'Even in fractures with exactly 2 mm of displacement, many surgeons favor closed reduction and percutaneous pinning (CRPP) or open reduction and internal fixation (ORIF) due to the high rate of late displacement in cast immobilization.' Therefore, CRPP or ORIF is the most appropriate management for a Jakob Stage 2 fracture with 3 mm of displacement.
- Option A is incorrect: Long arm cast immobilization is reserved strictly for truly nondisplaced fractures (Jakob Stage 1, <2 mm displacement) due to the high risk of late displacement in fractures with >2 mm displacement.
- Option B is incorrect: While ORIF is a valid option, cannulated screw fixation is typically reserved for older children or adolescents approaching skeletal maturity, and screws must not cross an open physis. K-wires are the standard for most pediatric cases.
- Option D is incorrect: Observation with a sling and early active range of motion is inappropriate for a displaced intra-articular fracture, which requires stabilization.
- Option E is incorrect: Delayed open reduction and bone grafting is a salvage strategy for established nonunions, not an initial management for an acute displaced fracture, and carries a high risk of AVN.
Question 26
A 7-year-old patient undergoes open reduction and internal fixation for a displaced lateral condyle fracture. Postoperatively, the patient is placed in a long arm splint. Three weeks later, radiographs show early callus formation and maintenance of reduction. The pins are removed. Which of the following instructions is most appropriate for the immediate post-pin removal rehabilitation phase?
Explanation
Correct Answer: B
The teaching case explicitly states the postoperative rehabilitation protocol: 'Following pin removal, the patient may begin active range of motion exercises. It is critical to emphasize active motion only. Passive stretching or aggressive physical therapy is strictly contraindicated in the pediatric elbow, as it increases the risk of joint stiffness, heterotopic ossification, and myositis ossificans.' This approach protects the healing fracture while allowing for gradual restoration of motion.
- Option A is incorrect: Passive stretching is strictly contraindicated due to the risk of complications like joint stiffness, heterotopic ossification, and myositis ossificans.
- Option C is incorrect: Immobilization is typically for 3-4 weeks. If callus formation is evident and reduction maintained, pins are removed, and active motion is initiated. Prolonged strict immobilization can lead to stiffness.
- Option D is incorrect: Weight-bearing activities are not appropriate immediately after pin removal and before complete bony remodeling, which takes longer.
- Option E is incorrect: Return to contact sports and high-impact activities is generally restricted for 10 to 12 weeks post-injury to allow for complete bony remodeling, not immediately after pin removal.
Question 27
A 10-year-old patient presents with a lateral condyle fracture that was initially missed and now presents 6 months later with an established nonunion and progressive cubitus valgus deformity. The patient is experiencing symptoms of tardy ulnar nerve palsy. Based on the case information, what is the most appropriate management strategy?
Explanation
Correct Answer: C
The teaching case addresses the management of established nonunion: 'If a nonunion is identified late (e.g., months or years after the injury) but the patient is completely asymptomatic with good range of motion, many surgeons advocate for benign neglect. Attempting to achieve union late requires extensive soft tissue stripping, which carries an unacceptably high risk of devascularizing the fragment and causing AVN. If the nonunion is symptomatic or associated with progressive valgus deformity, in situ fixation with bone grafting, often accompanied by an ulnar nerve transposition, is the preferred salvage strategy.' In this scenario, the patient is symptomatic with progressive cubitus valgus and tardy ulnar nerve palsy, making in situ fixation with bone grafting and ulnar nerve transposition the appropriate choice.
- Option A is incorrect: Benign neglect is for asymptomatic nonunions. This patient is symptomatic with progressive deformity and nerve palsy.
- Option B is incorrect: Aggressive open reduction with extensive soft tissue stripping is specifically cautioned against due to the exceedingly high risk of avascular necrosis in late presentations.
- Option D is incorrect: Elbow arthrodesis (fusion) is a drastic measure typically reserved for end-stage arthritis or severe instability, not a primary treatment for a symptomatic nonunion with cubitus valgus.
- Option E is incorrect: Serial casting and passive range of motion are not effective for correcting an established bony deformity like cubitus valgus or addressing a nonunion.
Question 28
A 5-year-old child sustains a lateral condyle fracture. The fracture fragment, which is largely cartilaginous at this age, includes the lateral metaphysis and the entire capitellum. Which of the following statements accurately describes the anatomical and biomechanical considerations relevant to this injury?
Explanation
Correct Answer: D
The teaching case states: 'At the typical age of injury (6 to 10 years), the lateral condyle is largely cartilaginous. The fracture fragment invariably includes the lateral metaphysis, the entire capitellum, and a variable portion of the lateral trochlear ridge.' This accurately describes the anatomical components of the fracture fragment.
- Option A is incorrect: The capitellum is the first ossification center to appear (1-2 years), not the last. The external (lateral) epicondyle is the last (10-12 years).
- Option B is incorrect: The 'pull-off' theory suggests a varus force applied to an extended elbow causes avulsion by the lateral collateral ligament complex and common extensor origin. The 'push-off' theory describes the axial load through the radius.
- Option C is incorrect: Standard radiographs consistently underestimate the true size of the fractured segment because the majority of the fragment is radiolucent cartilage.
- Option E is incorrect: The primary blood supply to the capitellum is from posterior end-arteries, and aggressive posterior soft tissue dissection risks devascularization, not anterior collateral arteries.
Question 29
During open reduction and internal fixation of a pediatric lateral condyle fracture, the surgeon has achieved anatomic reduction of the fracture fragment, as shown in the intraoperative image. The next critical step is to secure this reduction. Which of the following fixation strategies is generally considered the most biomechanically stable for this injury?

Explanation
Correct Answer: C
The teaching case states: 'Definitive fixation is typically achieved using two or three smooth K-wires (1.6 mm or 2.0 mm, depending on patient age). The most biomechanically stable configuration utilizes divergent pins. The first pin is directed from the lateral condyle, across the fracture site, engaging the medial cortex of the distal humerus. The second pin is directed more proximally up the lateral column. Parallel pins are also acceptable provided they achieve bicortical purchase.' Therefore, two or three divergent smooth K-wires achieving bicortical purchase is the most biomechanically stable configuration.
- Option A is incorrect: A single K-wire is generally insufficient for stable fixation of a displaced fracture.
- Option B is incorrect: While parallel pins are acceptable, divergent pins offer superior torsional stability. Unicortical purchase is less stable than bicortical.
- Option D is incorrect: Cannulated screws may be used in older children, but they must not cross an open physis to avoid premature growth arrest. A 5-year-old has an open physis.
- Option E is incorrect: Absorbable sutures are used to repair the capsule and extensor aponeurosis, but they do not provide sufficient bony fixation for a displaced fracture.
Question 30
A 7-year-old male presents with a lateral condyle fracture. The initial AP and lateral radiographs are ambiguous regarding the degree of displacement. An internal oblique view is obtained, which shows a fracture gap of 2.5 mm at the posterior aspect of the lateral metaphysis. Based on the current literature and guidelines, what is the most appropriate next step in management?
Explanation
Correct Answer: C
The teaching case emphasizes the critical threshold for operative management: 'Operative intervention is strongly indicated for any fracture demonstrating greater than 2 mm of displacement. Even in fractures with exactly 2 mm of displacement, many surgeons favor closed reduction and percutaneous pinning (CRPP) or open reduction and internal fixation (ORIF) due to the high rate of late displacement in cast immobilization.' The internal oblique view is highlighted as highly sensitive for detecting gap formation, and if the fracture gap measures greater than 2 mm, surgical fixation is warranted. A 2.5 mm gap clearly exceeds this threshold.
- Option A is incorrect: Cast immobilization is reserved for truly nondisplaced fractures (<2 mm). A 2.5 mm displacement has a high risk of late displacement in a cast.
- Option B is incorrect: While MRI can visualize cartilage, the case states that 'In rare cases where radiographs remain equivocal, magnetic resonance imaging (MRI) or an arthrogram can be utilized... though these are rarely necessary if high-quality internal oblique views are obtained.' With a clear 2.5 mm displacement on the internal oblique, further imaging is generally not needed to confirm the need for surgery.
- Option D is incorrect: Attempting a closed reduction in the ED for a displaced lateral condyle fracture is often unsuccessful and can cause further soft tissue damage or fragment rotation. Definitive reduction and fixation in the operating room are preferred.
- Option E is incorrect: Physical therapy to maintain range of motion is inappropriate for an acute, displaced fracture requiring stabilization.
Question 31
A 7-year-old patient undergoes successful open reduction and internal fixation of a lateral condyle fracture. During the follow-up period, the patient develops a 'fishtail' deformity of the capitellum on radiographs. Which of the following complications is most consistent with this radiographic finding?
Explanation
Correct Answer: D
The teaching case specifically describes avascular necrosis (AVN) of the capitellum as 'often manifesting radiographically as a "fishtail" deformity.' This complication is typically caused by iatrogenic disruption of the posterior vascular supply during open reduction, leading to central capitellar collapse.
- Option A is incorrect: Lateral spurring (overgrowth) is common but usually asymptomatic and does not present as a 'fishtail' deformity.
- Option B is incorrect: Delayed union refers to slow healing of the fracture, not a specific deformity of the capitellum.
- Option C is incorrect: Cubitus valgus is an angular deformity of the elbow (increased carrying angle) often secondary to nonunion or premature physeal closure, but it is not described as a 'fishtail' deformity of the capitellum itself.
- Option E is incorrect: Pin tract infection is a localized infection around the K-wires and does not cause a 'fishtail' deformity of the capitellum.
Question 32
Which of the following statements accurately reflects a key principle in the management of pediatric lateral condyle fractures, as emphasized by the provided teaching case and current guidelines?
Explanation
Correct Answer: D
The teaching case strongly emphasizes the importance of anatomic reduction: 'The management of pediatric lateral condyle fractures hinges entirely on the precise measurement of displacement and the assessment of articular congruity.' And in the summary, 'Recent guidelines from the Pediatric Orthopaedic Society of North America (POSNA) emphasize the absolute necessity of anatomic reduction. While K-wire fixation remains the standard of care for the vast majority of these fractures, biomechanical studies have shown that divergent pin placement offers superior torsional stability compared to parallel pins. Furthermore, literature regarding the late management of nonunions continues to caution against aggressive late open reduction, reinforcing the principle that the best treatment for a lateral condyle nonunion is its prevention through accurate initial diagnosis and meticulous surgical execution.'
- Option A is incorrect: The case states, 'More clinically relevant for treatment algorithms is the Jakob classification, which evaluates the degree of displacement and the integrity of the cartilaginous articular hinge.'
- Option B is incorrect: The case explicitly states, 'Passive stretching or aggressive physical therapy is strictly contraindicated in the pediatric elbow, as it increases the risk of joint stiffness, heterotopic ossification, and myositis ossificans.'
- Option C is incorrect: The case cautions against aggressive late open reduction for nonunions due to the high risk of AVN, advocating for benign neglect in asymptomatic cases and in situ fixation for symptomatic ones.
- Option E is incorrect: Cannulated screw fixation is an alternative for older children or adolescents approaching skeletal maturity, and must not cross an open physis. K-wires are the standard for most pediatric cases.
Question 33
A 5-year-old boy falls from monkey bars and sustains an extension-type supracondylar humerus fracture. Radiographs demonstrate that the distal fragment is displaced posteromedially. Based on this displacement pattern, which nerve is at the highest risk of injury?
Explanation
Question 34
A 35-year-old man presents with progressive weakness in his hands and numbness in his ring and small fingers. He sustained an untreated pediatric elbow fracture 30 years ago. Physical examination reveals a profound cubitus valgus deformity. Which of the following original pediatric injuries most likely led to this clinical presentation?
Explanation
Question 35
A 42-year-old woman presents with a slow-growing, painless mass on the volar aspect of her right index finger. Excisional biopsy is performed. Histopathologic examination reveals a lobulated proliferation of mononuclear cells, multinucleated giant cells, and lipid-laden macrophages with hemosiderin deposition. What is the most likely diagnosis?
Explanation
Question 36
An 11-year-old gymnast sustains an acute elbow dislocation. Following a successful closed reduction in the emergency department, post-reduction radiographs reveal that the medial epicondyle is fractured and incarcerated within the ulnohumeral joint. What is the most appropriate management?
Explanation
Question 37
A 29-year-old woman complains of excruciating, paroxysmal pain in her left ring fingertip. She reports severe cold intolerance in the digit. Examination reveals a subtle bluish discoloration beneath the nail plate. Point tenderness is exquisitely localized using the head of a pin (Love's test). What is the most likely diagnosis?
Explanation
Question 38
A 24-year-old chef sustains a laceration to the volar aspect of his right hand, severing the flexor tendons. The surgeon notes the injury is located in Zone II of the hand. Which of the following anatomic landmarks defines the boundaries of Zone II?
Explanation
Question 39
A 6-year-old boy falls from a trampoline and sustains a Gartland Type III supracondylar humerus fracture. On initial examination, the hand is pink and warm, but the radial pulse is not palpable. What is the most appropriate next step in management?
Explanation
Question 40
A 35-year-old man presents with a pathologic fracture of the proximal phalanx of the middle finger after minimal trauma. Radiographs show a well-circumscribed, central lytic lesion with stippled calcifications. The fracture is allowed to heal non-operatively over 6 weeks. What is the definitive management of the underlying lesion?
Explanation
Question 41
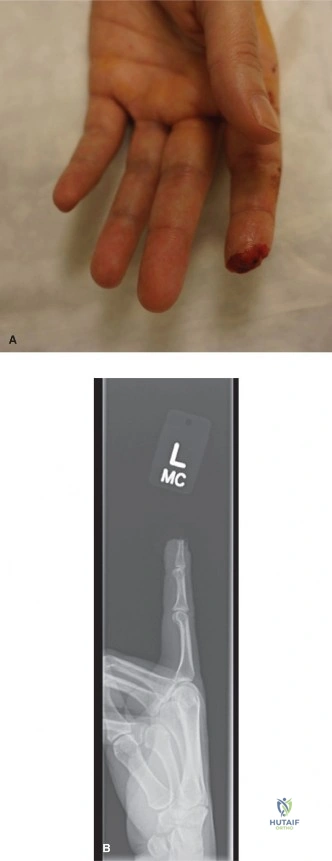
A 22-year-old rugby player grasps an opponent's jersey and sustains a forced extension injury to a maximally flexed ring finger. He cannot actively flex his DIP joint. Radiographs reveal a bony avulsion fracture of the distal phalanx resting at the level of the proximal interphalangeal (PIP) joint. According to the Leddy-Packer classification, what structure preserves the blood supply to the retracted tendon in this injury type?
Explanation
Question 42
An 8-year-old girl falls onto an outstretched hand and presents with lateral elbow pain. Radiographs reveal a radial neck fracture with 45 degrees of angulation. The radial head is not displaced from the capitellum. What is the initial step in management?
Explanation
Question 43
A 45-year-old carpenter develops a firm, subcutaneous mass on the volar aspect of his left thumb. He recalls a puncture wound to the same area several years prior. Excision reveals a cyst filled with cheesy, malodorous material. Histology shows a wall composed of stratified squamous epithelium. What is the diagnosis?
Explanation
Question 44
Intraoperative fluoroscopy is used to assess the reduction of a pediatric supracondylar humerus fracture. The surgeon measures Baumann's angle. Which two radiographic lines form this angle, and what does it assess?
Explanation
Question 45
A 30-year-old recreational basketball player jams his right middle finger. He presents with an inability to actively extend the distal interphalangeal (DIP) joint. Radiographs show no fracture. What is the most appropriate treatment for this closed tendinous mallet finger?
Explanation
Question 46
A 65-year-old woman presents with a slow-growing mass over the dorsal aspect of the distal interphalangeal (DIP) joint of her index finger. Examination reveals longitudinal grooving of the nail plate. Which underlying joint pathology is most universally associated with this soft tissue lesion?
Explanation
Question 47
A 7-year-old child sustains a Bado Type I Monteggia equivalent lesion. Which of the following best describes the typical bony and ligamentous configuration of this injury?
Explanation
Question 48
During a complex flexor tendon repair in Zone II, a surgeon must be careful to preserve the flexor tendon sheath pulleys to prevent biomechanical failure. Which two annular pulleys are the most critical to preserve to prevent bowstringing of the flexor tendons?
Explanation
Question 49
A 14-month-old child presents to the emergency department after a fall. The clinician reviews the elbow radiographs to rule out a fracture. According to normal pediatric development, which ossification center of the elbow is expected to be visible on radiographs at this age?
Explanation
Question 50
A 25-year-old rock climber presents with a sudden 'pop' and inability to flex the DIP joint of his middle finger. MRI confirms a Leddy-Packer Type I flexor digitorum profundus (FDP) avulsion. The tendon has retracted into the palm. Within what timeframe must surgical repair ideally be performed to prevent irreversible tendon necrosis and myostatic contracture?
Explanation
Question 51
During excision of a slow-growing, painful mass in the volar forearm of a 40-year-old man, the surgeon notes the tumor is eccentrically located on the median nerve. The mass is successfully dissected and 'shelled out' while completely preserving the continuity of the nerve fascicles. What is the most likely diagnosis?
Explanation
Question 52
A 4-year-old girl is evaluated for elbow pain after a fall. Radiographs demonstrate a supracondylar humerus fracture. The anterior humeral line passes anterior to the capitellum, but the posterior humeral cortex remains intact. According to the Gartland classification, what type of fracture is this?
Explanation
Question 53
A 6-year-old boy falls from the monkey bars and sustains an extension-type Gartland type III supracondylar humerus fracture. Upon physical examination, which of the following nerve injuries is MOST likely to be identified?
Explanation
Question 54
A 5-year-old girl sustains a severely displaced supracondylar humerus fracture. After successful closed reduction and percutaneous pinning in the operating room, her hand remains pink with brisk capillary refill, but the radial pulse is nonpalpable. What is the most appropriate next step in management?
Explanation
Question 55
A 4-year-old child falls on an outstretched hand. A radiograph similar to
demonstrates a lateral condyle fracture. If this fracture is left untreated and goes on to nonunion, which of the following is the most classic long-term complication?
Explanation
Question 56
A 12-year-old boy suffers a posterior elbow dislocation. Following closed reduction, a radiograph is obtained. Which of the following is considered an absolute indication for operative intervention in a pediatric medial epicondyle fracture?
Explanation
Question 57
A 35-year-old female presents with exquisite pain at the nail bed of her left index finger. She notes severe cold intolerance and pinpoint tenderness over the lunula. Love's pin test and Hildreth's test are positive. What is the most likely diagnosis?
Explanation
Question 58
A 45-year-old man notes a slowly enlarging, painless, firm mass on the volar aspect of his right middle finger. Excisional biopsy is performed. Histopathology reveals a lobulated lesion with multinucleated giant cells, foamy macrophages, and prominent hemosiderin deposition. What is the diagnosis?
Explanation
Question 59
A 30-year-old patient presents with a pathologic fracture of the proximal phalanx after a minor twisting injury. Radiographs show a well-defined, centrally located radiolucent lesion with stippled calcifications. What is the recommended treatment once the fracture has healed?
Explanation
Question 60
Which of the following is the most common late deformity resulting from a malunited pediatric supracondylar humerus fracture?
Explanation
Question 61
A 25-year-old rugby player sustains a jersey finger (avulsion of the flexor digitorum profundus). Imaging reveals a Leddy-Packer Type 1 injury, where the tendon has retracted into the palm. What is the recommended timing for surgical repair?
Explanation
Question 62
A 40-year-old man was struck on the tip of his long finger by a basketball and presents with a mallet finger deformity. Radiographs show a dorsal avulsion fracture involving 20% of the articular surface without joint subluxation. What is the most appropriate initial management?
Explanation
Question 63
A 7-year-old falls onto an outstretched hand and sustains a Bado Type I Monteggia fracture-dislocation (anterior dislocation of the radial head with a proximal ulna fracture). What is the critical first step in the management of this injury?
Explanation
Question 64
A 45-year-old diabetic patient presents with a swollen, painful index finger. Which of the following is NOT one of Kanavel's cardinal signs for pyogenic flexor tenosynovitis?
Explanation
Question 65
A 60-year-old female presents with a soft, translucent mass on the dorsal aspect of her right index DIP joint, associated with longitudinal nail grooving. To minimize the risk of recurrence during surgical excision, which of the following must be performed?
Explanation
Question 66
A 22-year-old chef lacerates his volar index finger. The attending hand surgeon diagnoses a 'Zone II' flexor tendon injury. What are the anatomic boundaries of Zone II?
Explanation
Question 67
A 5-year-old sustains a lateral condyle fracture of the humerus. Which of the following radiographic findings serves as an absolute indication for operative intervention (CRPP or ORIF)?
Explanation
Question 68
A 40-year-old presents with a volar forearm mass. Tinel's sign is positive over the mass. During surgical excision, the mass is noted to be eccentric, encapsulated, and easily separable from the main nerve fascicles. What is the most likely diagnosis?
Explanation
Question 69
Based on the expected chronological appearance of secondary ossification centers in the pediatric elbow (CRITOE), which center should be radiographically visible in a normal 6-year-old child, while the subsequent center is not yet visible?
Explanation
Question 70
A 2-year-old girl is brought to the emergency department refusing to move her right arm after her father lifted her by the wrist to step onto a curb. Her elbow is held in slight flexion and the forearm is pronated. What is the pathophysiology of this condition?
Explanation
Question 71
A 35-year-old tailor presents with a painless, firm mass at the tip of his left thumb. He recalls a penetrating injury with a needle at the same site approximately a year ago. Histopathology shows a sac lined by stratified squamous epithelium filled with laminated keratin. What is the diagnosis?
Explanation
Question 72
When utilizing a crossed-pinning technique (one medial and one lateral K-wire) for the fixation of a pediatric supracondylar humerus fracture, what is the most significant iatrogenic risk associated with the medial pin placement?
Explanation
Question 73
A 6-year-old boy presents to the emergency department after falling from a trampoline. Radiographs reveal a Gartland Type III supracondylar humerus fracture. The distal fragment is displaced posterolaterally. Based on this specific displacement pattern, which of the following nerve deficits is most likely to be present on examination?
Explanation
Question 74
A 13-year-old boy is evaluated for progressive weakness and clawing of his right ring and small fingers over the past two years. He sustained a right elbow fracture at age 4 that was managed non-operatively. Physical examination reveals a significant cubitus valgus deformity. Which of the following pediatric elbow fractures is most strongly associated with this late complication?
Explanation
Question 75
A 42-year-old woman complains of excruciating, pinpoint pain at the tip of her left index finger. She notes that the pain is severely exacerbated by cold weather. On examination, she is exquisitely tender at the nail bed, but the pain is entirely relieved when a tourniquet is applied to the base of the digit. What is the most likely diagnosis?
Explanation
Question 76
A 35-year-old carpenter underwent a primary flexor digitorum profundus (FDP) repair in his right ring finger one month ago. He now complains that he is entirely unable to make a full fist with his uninjured middle and small fingers. Which of the following biomechanical phenomena explains this presentation?
Explanation
Question 77
A 9-year-old girl falls onto her outstretched arm and sustains an acute posterior elbow dislocation. Following closed reduction in the emergency department, post-reduction radiographs demonstrate a medial epicondyle fracture with the avulsed fragment located inside the ulnohumeral joint. What is the most appropriate management?
Explanation
Question 78
A 50-year-old man presents with a firm, painless, slow-growing mass on the volar aspect of his right index finger proximal interphalangeal (PIP) joint. Excisional biopsy is performed. Histopathologic analysis demonstrates multinucleated giant cells, histiocytes, and extensive hemosiderin deposition. What is the diagnosis?
Explanation
Question 79
A 5-year-old boy presents with a completely displaced, extension-type supracondylar humerus fracture. The hand is pulseless and pale on presentation. Following closed reduction and percutaneous pinning, the hand becomes warm and pink with a capillary refill time of less than 2 seconds; however, the radial pulse remains unpalpable. What is the most appropriate next step in management?
Explanation
Question 80
A 28-year-old male sustains a minor twisting injury to his hand and presents with swelling and pain. Radiographs reveal a pathologic fracture through a central, expansile, lytic lesion in the proximal phalanx of the ring finger. Stippled calcifications are noted within the matrix. What is the recommended management after the fracture has healed?
Explanation
Question 81
A 22-year-old collegiate rugby player sustained an injury to his right ring finger when he violently grabbed an opponent's jersey. He is unable to actively flex the distal interphalangeal (DIP) joint. Ultrasound confirms a Type I Leddy-Packer avulsion, with the flexor digitorum profundus (FDP) tendon retracted into the palm. Within what timeframe must surgical repair ideally be performed to prevent permanent contracture and tendon necrosis?
Explanation
Question 82
A 4-year-old girl falls from monkey bars. Radiographs of the elbow reveal a fracture of the distal humerus. The anterior humeral line passes completely anterior to the capitellum, indicating posterior displacement of the distal fragment, but the posterior cortex remains intact, functioning as a hinge. What is the correct Gartland classification for this fracture?
Explanation
Question 83
A 38-year-old tailor presents with a painless, firm, superficial mass on the palmar tip of his left index finger. He recalls a deep penetrating needle prick injury at that exact location 3 years ago. Surgical excision reveals a well-encapsulated sac filled with a white, cheesy material. What is the most likely diagnosis?
Explanation
Question 84
A 32-year-old competitive rower presents with pain and swelling on the dorsal radial aspect of his distal forearm. Examination reveals palpable crepitus approximately 4 to 6 cm proximal to Lister's tubercle during active wrist extension. This condition is caused by friction between which of the following extensor compartments?
Explanation
Question 85
When interpreting pediatric elbow radiographs, understanding the chronologic appearance of secondary ossification centers is crucial. Which of the following sequences represents the normal order of ossification center appearance in a growing child?
Explanation
Question 86
A 45-year-old male presents with a slowly enlarging, painful mass in his volar forearm. Exam reveals a strongly positive Tinel's sign over the mass. Intraoperatively, the mass is found to be eccentric to the median nerve and is enucleated smoothly without disrupting the parent nerve fascicles. Which of the following histologic findings is characteristic of this tumor?
Explanation
Question 87
A 30-year-old recreational basketball player sustained an untreated mallet injury to his middle finger eight months ago. He now presents complaining of a secondary finger deformity. Based on the pathophysiology of chronic mallet finger, which of the following deformities is he at greatest risk of developing?
Explanation
Question 88
During intraoperative fluoroscopic evaluation of a reduced Gartland Type III supracondylar humerus fracture, the surgeon measures Baumann's angle on the anteroposterior (AP) view. What post-traumatic deformity is this measurement primarily designed to assess and prevent?
Explanation
Question 89
A 6-year-old girl falls on an outstretched hand and sustains an extension-type supracondylar humerus fracture. Upon initial presentation, her hand is pink but pulseless. After closed reduction and percutaneous pinning in the operating room, her hand remains pink and well-perfused, but the radial pulse remains unpalpable. What is the most appropriate next step in management?
Explanation
Question 90
A 45-year-old woman presents with a slow-growing, painless, firm, multilobulated mass on the volar aspect of her right index finger. Radiographs show soft tissue swelling but no bony involvement. MRI demonstrates a lobulated mass with decreased signal intensity on both T1- and T2-weighted images. Histology shows multinucleated giant cells and hemosiderin-laden macrophages. What is the most likely diagnosis and optimal treatment?
Explanation
Question 91
A 35-year-old woman presents with severe, cold-intolerant, pinpoint pain under her left index fingernail. Examination reveals a faint bluish discoloration beneath the nail plate and exquisite tenderness when pressure is applied with a pinhead (positive Love's test). The tumor responsible for this presentation originates from which of the following cell types?
Explanation
Question 92
A 5-year-old boy presents with an elbow injury. Radiographs reveal a displaced Milch Type II lateral condyle fracture. The surgeon recommends open reduction and internal fixation to prevent long-term sequelae. Which complication is most uniquely associated with nonunion of this specific pediatric fracture pattern?
Explanation
Question 93
A 25-year-old chef sustains a knife laceration to the volar aspect of his palm at the level of the A1 pulley. During surgical exploration, both the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons are found cleanly transected. In which flexor tendon zone did this injury occur, and what is the current standard of care?
Explanation
Question 94
A 12-year-old boy sustains a posterior elbow dislocation during a wrestling match. After a closed reduction in the emergency department, post-reduction radiographs show a slightly widened medial joint space and an absent medial epicondyle on the AP view. The lateral view shows a bony fragment within the ulnohumeral joint. What is the most appropriate management?
Explanation
Question 95
A 22-year-old man presents with a pathological fracture of the proximal phalanx of the ring finger after mildly bumping his hand against a door. Radiographs show a centrally located, expansile radiolucent lesion with stippled calcifications. What is the most appropriate treatment sequence for this patient?
Explanation
Question 96
An 18-year-old rugby player presents with inability to actively flex the DIP joint of his right ring finger. Radiographs show a large bony fragment avulsed from the volar aspect of the distal phalanx, which has retracted to the level of the distal interphalangeal (DIP) joint.
According to the Leddy and Packer classification, what type of flexor digitorum profundus (FDP) avulsion injury is this?
Explanation
None
