AAOS & ABOS Spine MCQs (Set 4): Trauma, Degenerative & Deformity | Board Prep

Key Takeaway
This high-yield question set (Set 4) for AAOS and ABOS board exams focuses on critical spine surgery topics. It includes multiple-choice questions on the diagnosis and management of spinal trauma, degenerative disc disease, and various adult spinal deformities. Ideal for residents and practicing orthopedic surgeons preparing for certification.
AAOS & ABOS Spine MCQs (Set 4): Trauma, Degenerative & Deformity | Board Prep
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
During the application of halo skeletal fixation, the most appropriate position for the placement of the anterior halo pins is approximately 1 cm above the superior orbital rim and
Explanation
Question 2
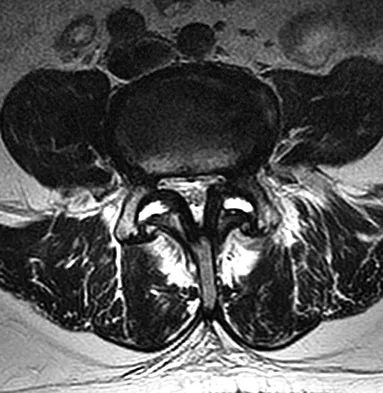
Figures 28a and 28b show the sagittal and axial lumbar MRI scans of a 72-year-old man who reports dull aching back pain that spreads to his legs, calves, and buttocks. He has had the pain for several years and it is precipitated by standing and walking and relieved by sitting. His symptoms have been worsening over the past year and he notes that he is leaning forward while walking to help relieve his symptoms. He has had no treatment to date. What is his prognosis if he chooses to pursue nonsurgical management for this condition?
Explanation
Question 3
Which of the following vertebrae has the smallest pedicle isthmic width in a nondeformity patient?
Explanation
Question 4
Which of the following represents a contraindication for interspinous process decompression for the treatment of lumbar spinal stenosis?
Explanation
Question 5
Which of the following statements about hoarseness due to vocal cord paralysis after anterior cervical diskectomy and fusion is most accurate?
Explanation
Question 6
A 23-year-old man is involved in a motor vehicle accident. An AP radiograph is shown in Figure 29a, and axial and sagittal CT scans are shown in Figures 29b and 29c. Neurologic examination shows 1/5 strength of his quadriceps and iliopsoas on the right, with 1/5 quadriceps function on the left. Definitive treatment of his injury should consist of
Explanation
Question 7
Surgical treatment for symptomatic disk herniations is associated with which of the following?
Explanation
Question 8
A 25-year-old man is unresponsive at the scene of a high-speed motor vehicle accident and remains obtunded. Initial evaluation in the emergency department reveals a left-sided femoral shaft fracture and a right-sided humeral shaft fracture. The cervical spine remains immobilized in a semi-rigid cervical collar, and the initial AP and lateral radiographs obtained in the emergency department are unremarkable. What is the most appropriate management at this time?
Explanation
Question 9
A 55-year-old woman undergoes an anterior cervical diskectomy and fusion at C5-C6 through a left-sided approach. One year later, she requires an anterior cervical diskectomy and fusion on another level. Which of the following is considered a contraindication to performing a right-sided approach for the revision procedure?
Explanation
Question 10
A 56-year-old woman sustained the fracture shown in Figures 30a and 30b in a motor vehicle accident. What mechanism is most likely responsible for the injury?
Explanation
Question 11
In providing culturally competent care to a Muslim woman with a cervical spine injury, which of the following most accurately describes the steps a male orthopaedist should take to respect her religious beliefs during his examination?
Explanation
Question 12
Figure 31 shows the radiograph of a 64-year-old woman who is seen in the emergency department following a motor vehicle accident. She has no voluntary motor function in her distal upper extremities or lower extremities. She does not have a bulbocavernosus reflex. She has a blood pressure of 80/50 mm Hg with a pulse of 50/min. Her hypotension does not improve with initial fluid resuscitation. Further treatment of her hypotension should consist of
Explanation
Question 13
What is the typical axial plane transverse angulation of the thoracic pedicles?
Explanation
Question 14
What muscle is most often encountered during surgical approaches to C5-6?
Explanation
Question 15
Which of the following lumbar disk components has the highest tensile modulus to resist torsional, axial, and tensile loads?
Explanation
Question 16
When comparing the overall outcomes of surgical versus nonsurgical treatment of stable thoracolumbar burst fractures in patients without neurologic injury, 5 years following injury, the principle differences lie in
Explanation
Question 17
A 42-year-old woman who has had an 18-month history of severe low back pain is referred to your office for surgical evaluation. She reports that the pain initially began with right lower extremity pain and management consisted of oral analgesics, nonsteroidal anti-inflammatory drugs, and muscle relaxants. She has seen a chiropractor as well as a pain management specialist and she is status-post epidural steroid injections. She has also completed exhaustive physical therapy, as she is a certified athletic trainer and runs a health fitness program at a community hospital. Currently, she denies lower extremity pain and her pain is isolated to her low back and is subjectively graded as 8/10, with 10 being the worst pain she has ever experienced. The pain is interfering with her activities of daily living and she is seeking definitive treatment. Figures 32a through 32c show current MRI scans. Based on the current available medical literature, what is the most appropriate treatment?
Explanation
Question 18
Figure 33 shows the MRI scan of a 55-year-old woman who has had a 6-week history of back and leg pain. Which of the following clinical scenarios is most consistent with the MRI scan findings at L4-L5?
Explanation
Question 19
Intradiskal electrothermal therapy (IDET) uses an intradiskal catheter to deliver controlled thermal energy to the inner periphery of the annulus fibrosis of a chronically painful intervertebral disk. Lumbar diskography is used diagnostically to identify the presumed pain generator to be targeted with IDET. Based on the medical literature, what can be said about the current status of IDET?
Explanation
Question 20
A 56-year-old mechanic has had pain in the hypothenar region of his dominant right hand for the past 6 months. He reports weakness in his grip and pain is worse with activity. Which of the following examination findings is most suggestive of a cervical etiology?
Explanation
Question 21
A 35-year-old woman reports an 8-week history of neck pain radiating to her right upper extremity. She denies any history of trauma or provocative event. Examination reveals decreased pinprick sensation in her right middle finger, otherwise sensation is intact bilaterally. Finger flexors and interossei demonstrate 5/5 motor strength bilaterally. Finger extensors are 4/5 on the right and 5/5 on the left. The triceps reflex is 1+ on the right and 2+ on the left. The most likely diagnosis is a herniated nucleus pulposus at what level?
Explanation
Question 22
What is the most common nonanesthetic-related reversible cause of changes in intraoperative neurophysiologic monitoring data?
Explanation
Question 23
During a left-sided transforaminal lumbar interbody fusion at the L4-5 level, the surgeon notes a significant amount of bleeding that cannot be controlled while using a pituitary rongeur. What anatomic structure has been injured?
Explanation
Question 24
Six weeks after onset, what is the most clearly accepted indication for surgical management for lumbar disk herniation?
Explanation
Question 25
A 45-year-old woman has idiopathic scoliosis. Surgery is to include an anterior thoracic release through an open left thoracotomy. The thoracotomy will have what effect on the patient's pulmonary function postoperatively?
Explanation
Question 26
A 25-year-old obtunded male is brought to the trauma bay after a motor vehicle collision. CT shows a right-sided unilateral facet dislocation at C5-C6. What is the most appropriate next step in management?
Explanation
Question 27
In the evaluation of adult spinal deformity, achieving appropriate sagittal balance is critical. Which of the following formulas best describes the ideal relationship between pelvic incidence (PI) and lumbar lordosis (LL) to optimize outcomes?
Explanation
Question 28
A 45-year-old man presents with acute right anterior thigh pain and weakness in knee extension. A representative MRI reveals a far lateral disc herniation at the L4-L5 level on the right.
Which nerve root is most likely compressed in this scenario?

Explanation
Question 29
Which of the following morphological fracture patterns is assigned the highest point value in the Thoracolumbar Injury Classification and Severity (TLICS) system?
Explanation
Question 30
A 65-year-old female with a 20-year history of rheumatoid arthritis presents with progressive hand clumsiness. Flexion-extension cervical radiographs show an anterior atlantodens interval (ADI) of 11 mm. What is the most reliable radiographic predictor of impending neurologic deficit in this patient?
Explanation
Question 31
A 72-year-old man with cervical spondylosis falls forward, striking his forehead. He presents with profound bilateral upper extremity weakness but retains moderate strength in his lower extremities. Which of the following is true regarding his condition?
Explanation
Question 32
A 58-year-old man with advanced ankylosing spondylitis presents with severe neck pain following a ground-level fall. Neurological examination is intact. Plain radiographs of the cervical spine appear normal. What is the next most appropriate step in management?
Explanation
Question 33
A 30-year-old male dives into a shallow pool and sustains a C1 Jefferson fracture. Open-mouth odontoid radiographs reveal lateral displacement of the lateral masses. According to the Rule of Spence, rupture of the transverse ligament is highly suspected if the combined lateral mass overhang exceeds:
Explanation
Question 34
A 65-year-old man presents with bilateral hand weakness and numbness after a hyperextension injury. He is able to ambulate but struggles to button his shirt. What is the most likely anatomic location of the primary spinal cord injury?
Explanation
Question 35
In adult spinal deformity surgery, achieving proper sagittal balance is highly correlated with improved Health-Related Quality of Life (HRQOL) outcomes. Which of the following radiographic targets is generally recommended?
Explanation
Question 36
A 24-year-old male is intubated and obtunded following a severe motor vehicle collision. Radiographs demonstrate a unilateral facet dislocation at C5-C6. What is the most appropriate next step prior to attempted surgical reduction?
Explanation
Question 37
A 65-year-old man presents with progressive clumsiness in his hands and difficulty walking. Examination reveals a positive Hoffman's sign and generalized hyperreflexia.
What is the most common gait abnormality seen in patients with this condition?
Explanation
Question 38
In the Lenke classification of adolescent idiopathic scoliosis, a lumbar curve is considered a 'structural' minor curve if it bends out to what minimum Cobb angle on supine side-bending radiographs?
Explanation
Question 39
A 40-year-old male falls from a height and sustains an L1 burst fracture. He is neurologically intact.
Which of the following parameters is the strongest indication for operative stabilization over nonoperative management?
Explanation
Question 40
A 45-year-old man presents with right leg pain radiating to the dorsum of his foot and isolated weakness in great toe extension. Which nerve root is most likely compressed, and what is the typical associated reflex abnormality?
Explanation
Question 41
In surgical planning for adult spinal deformity, achieving optimal spinopelvic harmony is critical. Which formula represents the ideal relationship between pelvic incidence (PI) and lumbar lordosis (LL)?
Explanation
Question 42
A 78-year-old female presents with neck pain after a low-energy fall. CT reveals a Type II odontoid fracture with 2 mm of posterior displacement.
What is the most significant risk factor for nonunion if treated nonoperatively?

Explanation
Question 43
Three years following an L4-L5 posterior lumbar interbody fusion (PLIF), a patient develops adjacent segment degeneration at L3-L4. Which biomechanical change at the adjacent segment is most directly responsible?
Explanation
Question 44
A 16-year-old female wearing a lap belt in an MVA sustains a flexion-distraction injury (Chance fracture) of L2.
Which of the following associated injuries must be aggressively ruled out?
Explanation
Question 45
A 15-year-old boy presents with progressive mid-back pain. Radiographs show a thoracic kyphosis of 55 degrees. Which radiographic criteria is strictly required to diagnose Scheuermann's kyphosis?
Explanation
Question 46
A 78-year-old man falls and sustains a Type II odontoid fracture with 1 mm of displacement. He has a history of severe chronic obstructive pulmonary disease (COPD) and heart failure. He is neurologically intact. What is the most appropriate initial management?
Explanation
Question 47
A 65-year-old male presents with bilateral upper extremity weakness (hands > arms) and mild lower extremity weakness after a hyperextension injury. Which of the following is true regarding his prognosis?
Explanation
Question 48
A 45-year-old male arrives intubated and sedated with a unilateral C6-C7 facet dislocation. What is the most appropriate next step prior to attempting reduction?
Explanation
Question 49
What is the most common associated intra-abdominal injury in a pediatric patient with a flexion-distraction (Chance) fracture of the lumbar spine?
Explanation
Question 50
A 14-year-old female with Adolescent Idiopathic Scoliosis has a right thoracic curve. She is Risser 0 and pre-menarchal. Her curve measures 35 degrees. What is the most appropriate treatment?
Explanation
Question 51
In planning for adult spinal deformity correction, which of the following radiographic relationships is the primary goal to achieve a well-balanced spine?
Explanation
Question 52
During the anterior approach to the lower cervical spine (C5-C7), which of the following structures is at greatest risk of injury when dissecting in the tracheoesophageal groove on the right side?
Explanation
Question 53
A 30-year-old male presents with severe right leg pain and weakness in big toe extension. MRI reveals a large paracentral disc herniation at L4-L5. Which nerve root is most likely affected?
Explanation
Question 54
Which of the following is an absolute indication for surgical intervention in a patient with a traumatic thoracolumbar burst fracture?
Explanation
Question 55
A 60-year-old male with long-standing Ankylosing Spondylitis presents with neck pain after a minor fall. Initial plain radiographs of the cervical spine are unremarkable. What is the most appropriate next step in management?
Explanation
Question 56
In evaluating an atlas (C1) ring fracture, lateral mass displacement on the open-mouth odontoid radiograph indicates a tear of the transverse atlantal ligament if the combined displacement exceeds what value?
Explanation
Question 57
A 25-year-old man presents with a unilateral C5-C6 facet dislocation and a C6 radiculopathy following a motor vehicle collision. He is awake, alert, and cooperative. What is the most appropriate initial management?
Explanation
Question 58
A 35-year-old woman falls from a height and sustains a T12 burst fracture. Imaging reveals splaying of the spinous processes and an MRI shows disruption of the posterior ligamentous complex. She is neurologically intact. What is her Thoracolumbar Injury Classification and Severity (TLICS) score?
Explanation
Question 59
In planning a corrective surgery for adult spinal deformity, which of the following spinopelvic parameter relationships represents the primary goal to achieve optimal sagittal balance?
Explanation
Question 60
A 45-year-old man presents with severe right leg pain. An MRI of the lumbar spine reveals a far lateral (extraforaminal) disc herniation on the right side at the L4-L5 level. Which nerve root is most likely compressed, and what clinical finding would be expected?
Explanation
Question 61
Which of the following anatomical factors is most strongly associated with the development of degenerative spondylolisthesis at L4-L5?
Explanation
Question 62
A 40-year-old man presents to the emergency department with acute onset of severe back pain, saddle anesthesia, and urinary retention. Post-void residual volume is 400 mL. Emergent MRI confirms a massive L4-L5 disc herniation. To maximize the chance of full neurologic recovery, decompression should ideally be performed within what maximum timeframe from the onset of symptoms?
Explanation
Question 63
Which of the following factors is most predictive of nonunion following nonoperative management (halo immobilization) of a Type II odontoid fracture?
Explanation
Question 64
A 65-year-old man undergoes a posterior cervical laminectomy and fusion from C3-C7 for severe cervical spondylotic myelopathy. On postoperative day 2, he develops isolated profound weakness of bilateral deltoids and biceps, but has no sensory changes and lower extremity function remains normal. What is the most likely etiology of this complication?
Explanation
Question 65
A 60-year-old man with a long-standing history of ankylosing spondylitis sustains a minor ground-level fall. He complains of severe neck pain but has no neurologic deficits. Plain radiographs of the cervical spine are difficult to interpret due to artifact and deformity, but appear unchanged from previous. What is the next best step in management?
Explanation
Question 66
An 82-year-old male sustains a Type II odontoid fracture after a ground-level fall. He has multiple medical comorbidities. Which of the following management strategies carries the lowest treatment-related morbidity while still providing acceptable clinical outcomes, despite having the highest rate of nonunion?
Explanation
Question 67
A 25-year-old male is involved in a high-speed motor vehicle collision while wearing a lap seatbelt. Radiographs demonstrate a flexion-distraction injury (Chance fracture) at L1. Which of the following is the most commonly associated concomitant injury?
Explanation
Question 68
A 65-year-old female presents with progressive difficulty manipulating buttons, frequent dropping of objects, and a broad-based gait. Physical examination reveals a positive Hoffmann sign and hyperreflexia in the lower extremities. MRI confirms severe spinal cord compression at C4-C5. What is the most appropriate next step in management?
Explanation
Question 69
During the surgical planning for an adult patient with severe sagittal imbalance, the surgeon evaluates the spinopelvic parameters. Which of the following formulas correctly describes the fixed anatomic relationship of the pelvis?
Explanation
Question 70
A 70-year-old male reports bilateral leg heaviness, pain, and paresthesias that worsen after walking 50 yards. He notes that the symptoms are significantly relieved when he leans forward on a shopping cart or walks uphill, but worsen when walking downhill. What is the most likely diagnosis?
Explanation
Question 71
A 55-year-old male with long-standing ankylosing spondylitis presents to the emergency department complaining of neck pain following a minor ground-level fall. He is neurologically intact. Plain radiographs of the cervical spine are interpreted as negative for acute fracture. What is the most appropriate next step?
Explanation
Question 72
A 14-year-old female gymnast complains of insidious onset, activity-related low back pain. Radiographs demonstrate a Grade 1 isthmic spondylolisthesis at L5-S1 with an identifiable pars interarticularis defect. She has no neurologic deficits. What is the most appropriate initial management?
Explanation
Question 73
When utilizing the Thoracolumbar Injury Classification and Severity (TLICS) score to determine the indication for surgery in a thoracolumbar burst fracture, which of the following radiographic parameters is heavily weighted and strongly drives the recommendation toward surgical stabilization?
Explanation
Question 74
A 45-year-old male presents with severe radicular leg pain. MRI reveals a far lateral (extraforaminal) disc herniation at the L4-L5 level. Which nerve root is most likely compressed by this specific herniation?
Explanation
Question 75
A 72-year-old male with known cervical spondylosis falls forward and strikes his chin, forcefully hyperextending his neck. He arrives at the ER with significant weakness in his upper extremities and relatively preserved motor function in his lower extremities. Which incomplete spinal cord syndrome has he developed?
Explanation
Question 76
Which of the following describes the accepted radiographic criteria established by Sorensen for the diagnosis of typical Scheuermann's kyphosis?
Explanation
Question 77
A 60-year-old male of Japanese descent undergoes an anterior cervical corpectomy for progressive myelopathy caused by severe Ossification of the Posterior Longitudinal Ligament (OPLL). Which of the following is the most frequent intraoperative complication specifically associated with anterior resection of this pathology?
Explanation
Question 78
A 28-year-old male presents with severe neck pain and C6 radiculopathy after a high-speed rollover collision. Lateral radiographs reveal approximately 25% anterior translation of the C5 vertebral body over C6. What is the most likely mechanism of this injury?
Explanation
Question 79
A 60-year-old female with metastatic breast cancer presents with progressive back pain. The Spinal Instability Neoplastic Score (SINS) is utilized to evaluate her need for surgical stabilization. Which of the following factors is incorporated into the SINS calculation?
Explanation
None
