Orthopedic Anatomy 2026 MCQs: Board Review Questions & Answers (Part 2)
Key Takeaway
Discover the latest medical recommendations for Orthopedic Anatomy 2026 MCQs: Board Review Questions & Answers (Part 2). Top-rated Orthopedic Anatomy 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Anatomy 2026 MCQs: Board Review Questions & Answers (Part 2)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figure 14 shows a lateral radiograph of a knee joint. The bony structure indicated by the arrow is a sesamoid bone that resides in what tendon?
Explanation
Question 2
Talar compression syndrome in ballet dancers typically involves injury to which of the following structures?
Explanation
Question 3
The sartorius muscle is innervated by which of the following nerves?
Explanation
Question 4
Pacinian corpuscles are lamellated nerve endings that are responsible for providing the perception of
Explanation
Question 5
An elite gymnast injured her ankle in an awkward dismount 36 hours ago. Examination reveals weakness on single leg step-up. A clinical photograph of the medial ankle is shown in Figure 15. Plain radiographs are normal. To help confirm the diagnosis, the next step in evaluation should consist of
Explanation
Question 6
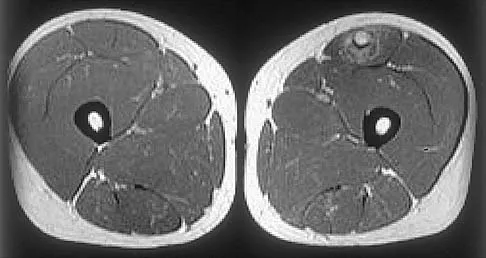
Figure 16 shows an axial MRI scan through the knee joint. What structure is identified by the arrow?
Explanation
Question 7
Which of the following nerves is most commonly injured when obtaining a bone graft from the posterior ilium?
Explanation
Question 8
Based on the findings seen in the posteroanterior radiograph of the wrist shown in Figure 17, which of the following structures is torn?
Explanation
Question 9
What tendon has an intra-articular (instrasynovial) location in the knee joint?
Explanation
Question 10
A patient undergoes hip arthroscopy, and the pathology is seen in Figure 18. What is the most likely diagnosis?
Explanation
Question 11
Figure 19 shows an arthroscopic view from the anterior lateral portal of the knee looking into the suprapatella pouch. The use of an electrothermal device during this procedure most commonly causes significant postoperative complications by damaging which of the following structures?
Explanation
Question 12
Figure 20 shows the resting and stress radiographs of a patient who has had pain and feelings of instability after undergoing a total knee arthroplasty 1 year ago. Which of the following ligaments is not functional and is therefore responsible for the patient's symptoms?
Explanation
Question 13
On MRI, a nonsanguinous effusion has what appearance?
Explanation
Question 14
Which of the following illustrations shown in Figures 21a through 21e correctly shows the projection of the sacroiliac joint on the outer table of the ilium?
Explanation
Question 15
In children between the ages of 4 and 8 years, the major blood supply to the femoral head comes from the
Explanation
Question 16
What is the most anatomic location for placement of the femoral tunnel in anterior cruciate ligament reconstruction?
Explanation
Question 17
In the anterior approach (Smith-Petersen) to the hip, dissection is carried out between muscles innervated by the
Explanation
Question 18
What structure is marked Q in the diagram of the brachial plexus shown in Figure 22?
Explanation
Question 19
A sagittal T1-weighted MRI scan of the knee joint is shown in Figure 23. What structure is identified by the arrow?
Explanation
Question 20
Figure 24 shows the arthroscopic view of a patient with ankle impingement syndrome. This is commonly seen after high ankle sprains and represents fibrotic granulation thickening of what structure?
Explanation
Question 21
The modified Brostrom lateral ankle ligamentous reconstruction uses which of the following structures to provide supplementary stabilization?
Explanation
Question 22
Figure 25 shows an arthroscopic thermal capsular shrinkage device being used in the anterior inferior quadrant of a patient with a subluxating shoulder. Which of the following neurologic complications is most frequently reported with this technique?
Explanation
Question 23
A coronal MRI scan through the shoulder joint is shown in Figure 26. The cyst indicated by the arrow will most likely cause compression of what nerve?
Explanation
Question 24
Which of the following ligaments is most commonly involved in posterolateral rotatory instability of the elbow?
Explanation
Question 25
Which of the following anatomic structures is labeled 6 in Figure 27?
Explanation
Question 26
A patient sustains a deep penetrating injury immediately anterior to the anterior scalene muscle in the lower neck. Which of the following structures is most likely injured in this specific location?
Explanation
Question 27
Hypertrophy of the teres minor and the long head of the triceps brachii can lead to nerve compression within the quadrangular space. Which of the following clinical findings would most likely be observed in this scenario?
Explanation
Question 28
During an ilioinguinal approach to the acetabulum, massive bleeding is encountered posterior to the superior pubic ramus. This bleeding is most likely originating from the 'corona mortis', which represents an anastomosis between which two vascular systems?
Explanation
Question 29
A surgeon is performing a complex midfoot reconstruction and explores the plantar aspect of the navicular. At the 'master knot of Henry', which of the following tendons crosses superior (dorsal) to the flexor digitorum longus (FDL) tendon?
Explanation
Question 30
A rock climber presents with acute bowstringing of the index finger flexor tendons following a sudden forceful grip. This condition typically results from rupture of the A2 and A4 pulleys. To what specific structures do these critical pulleys attach?
Explanation
Question 31
A cyclist complains of persistent numbness in the ring and small fingers along with weakness in finger abduction. Compression of a nerve within Guyon's canal is suspected. Which of the following structures forms the floor of this anatomic canal?
Explanation
Question 32
A professional volleyball player presents with isolated weakness of the infraspinatus muscle. MRI reveals a ganglion cyst compressing a nerve at the spinoglenoid notch. Which ligament forms the roof of this notch?
Explanation
Question 33
In an adult patient, which of the following branches of the medial femoral circumflex artery provides the primary blood supply to the weight-bearing dome of the femoral head?
Explanation
Question 34
During surgical reconstruction of the posterolateral corner (PLC) of the knee, understanding the layered anatomy is essential. Which of the following structures are located in the superficial layer (Layer 1) of the lateral side of the knee?
Explanation
Question 35
A spine surgeon is placing pedicle screws in the L4 vertebra. Which anatomical relationship best describes the position of the exiting L4 nerve root relative to the L4 pedicle?
Explanation
Question 36
A patient presents with an inability to actively extend the fingers and thumb, but wrist extension is preserved with radial deviation. Posterior interosseous nerve (PIN) syndrome is suspected. What is the most common site of compression for this nerve?
Explanation
Question 37
During an anterolateral approach to the distal tibia, a nerve is at risk of being injured where it transitions from deep to subcutaneous tissue. At what location does the superficial peroneal nerve typically pierce the deep crural fascia?
Explanation
Question 38
During a dorsal approach to the wrist, the surgeon uses Lister's tubercle as a landmark. The tendon that passes immediately adjacent and ulnar to this structure is innervated by which of the following nerves?
Explanation
Question 39
The volar approach to the proximal forearm (Henry approach) utilizes a safe internervous plane. Which of the following pairs of nerves supplies the two muscles that define this plane?
Explanation
Question 40
While performing a lateral (Hardinge) approach to the hip, the surgeon must limit the proximal splitting of the gluteus medius muscle to no more than 3 to 5 cm above the greater trochanter. This precaution primarily protects which of the following structures?
Explanation
Question 41
A marathon runner with chronic, severe medial heel pain is diagnosed with entrapment of the first branch of the lateral plantar nerve (Baxter's nerve). Which of the following muscles receives its motor innervation from this specific nerve?
Explanation
Question 42
A patient is undergoing a total knee arthroplasty and receives an ultrasound-guided saphenous nerve block within the adductor canal (Hunter's canal). Which muscle forms the anterolateral boundary of this canal?
Explanation
Question 43
The coracoclavicular (CC) ligaments provide the primary vertical stability to the acromioclavicular joint. Which of the following describes the anatomical position of the conoid ligament relative to the trapezoid ligament?
Explanation
Question 44
In cases of thumb carpometacarpal (CMC) joint arthritis, progressive attenuation of the primary static stabilizing ligament is often noted. From which anatomical structure does this critical ligament, the anterior oblique ligament (beak ligament), originate?
Explanation
Question 45
During a sacrospinous ligament fixation procedure for pelvic organ prolapse, an orthopedic surgeon assisting the case notes a suture placement too close to the ischial spine. Which nerve loops around the ischial spine and is at greatest risk of iatrogenic entrapment here?
Explanation
Question 46
The great anterior radiculomedullary artery (Artery of Adamkiewicz) provides major blood supply to the lower two-thirds of the spinal cord. It most commonly enters the spinal canal at which of the following levels?
Explanation
Question 47
During an ilioinguinal approach to the acetabulum, brisk bleeding is encountered just posterior to the superior pubic ramus. This bleeding is most likely originating from an anastomosis between which two vessels?
Explanation
Question 48
Which of the following describes the most common configuration of a Martin-Gruber anastomosis?
Explanation
Question 49
A patient presents with isolated weakness of external rotation of the shoulder with preserved abduction. At which of the following anatomical locations is nerve entrapment most likely occurring?
Explanation
Question 50
Which of the following is the primary anatomic footprint for the distal attachment of the lateral ulnar collateral ligament (LUCL)?
Explanation
Question 51
At the level of the "Master Knot of Henry" in the plantar aspect of the midfoot, what is the anatomical relationship between the flexor hallucis longus (FHL) and flexor digitorum longus (FDL) tendons?
Explanation
Question 52
The primary blood supply to the proximal pole of the scaphoid is derived from vessels entering at which anatomical location?
Explanation
Question 53
During a posterior approach to the hip, protecting the medial circumflex femoral artery (MFCA) is critical. The main branch of the MFCA runs most consistently between which two muscles before piercing the hip capsule?
Explanation
Question 54
Which of the following nerves exits the adductor (Hunter's) canal by piercing the vastoadductor fascia?
Explanation
Question 55
The vertebral artery typically enters the transverse foramen of the cervical spine at which vertebral level?
Explanation
Question 56
The posterior interosseous nerve (PIN) is most vulnerable to iatrogenic injury during a Henry approach to the proximal radius at which of the following anatomic structures?
Explanation
Question 57
The axillary nerve passes through the quadrangular space. What muscle forms the inferior border of this space?
Explanation
Question 58
In approximately 10-15% of the population, a variation in the relationship between the sciatic nerve and the piriformis muscle exists. What is the most common anatomical variant?
Explanation
Question 59
The genicular arteries provide blood supply to the menisci of the knee. In an adult, vascular penetration extends to approximately what depth of the meniscus?
Explanation
Question 60
When utilizing the direct lateral (Hardinge) approach to the hip, what is the generally accepted "safe zone" for proximal splitting of the gluteus medius to avoid injury to the superior gluteal nerve?
Explanation
Question 61
During trigger finger release of the ring finger, the A1 pulley is transected. Which pulleys are considered mechanically critical to prevent bowstringing of the flexor tendons and must be preserved?
Explanation
Question 62
The spring ligament complex is a critical static stabilizer of the longitudinal arch of the foot. Between which two osseous structures does it primarily attach?
Explanation
Question 63
Wartenberg's syndrome is characterized by pain and paresthesias over the dorsoradial hand. It is typically caused by compression of the superficial radial nerve between which two muscles during forearm pronation?
Explanation
Question 64
During reconstruction of the posterolateral corner (PLC) of the knee, the anatomic insertion of the popliteus tendon on the femur is located:
Explanation
Question 65
A Morton's neuroma most commonly occurs in the third web space of the foot. This is anatomically predisposed by the union of branches from which two nerves?
Explanation
Question 66
A 45-year-old mechanic presents with weakness in extending his fingers and thumb, but normal wrist extension. Which of the following anatomical structures is the most common site of entrapment for the affected nerve?
Explanation
Question 67
During an operative fixation of a scaphoid waist fracture using a volar approach, the surgeon must be careful to preserve the primary blood supply to the proximal pole. This blood supply enters the scaphoid primarily through which of the following areas?
Explanation
Question 68
The popliteofibular ligament is a crucial stabilizer of the posterolateral corner of the knee. From which structure does it originate and where does it insert?
Explanation
Question 69
Following a displaced femoral neck fracture in an adult, the principal blood supply to the femoral head is disrupted. Which of the following vessels provides the majority of the blood supply to the adult femoral head?
Explanation
Question 70
A patient develops a severe horseshoe abscess of the hand extending from the thumb to the small finger. The infection spreads proximally into the distal forearm. In which anatomical space does this proximal extension reside?
Explanation
Question 71
The anterolateral ligament (ALL) of the knee is increasingly recognized for its role in controlling rotatory laxity. What are its precise anatomical landmarks?
Explanation
Question 72
A marathon runner complains of medial heel pain and paresthesias radiating to the first three toes. The nerve involved in this condition runs beneath the flexor retinaculum. Which of the following muscles is innervated by the terminal branch of this nerve?
Explanation
Question 73
A professional volleyball player presents with isolated weakness in external rotation of the shoulder. Atrophy is noted in the infraspinatus fossa, while the supraspinatus is normal. Entrapment of the suprascapular nerve is suspected at which location?
Explanation
Question 74
During reconstruction of an acromioclavicular joint separation, anatomic reduction of the coracoclavicular ligaments is desired. Which of the following statements accurately describes the anatomy of the conoid and trapezoid ligaments?
Explanation
Question 75
The calcaneonavicular (spring) ligament complex is a critical stabilizer of the longitudinal arch. Which portion of the spring ligament is the strongest and most frequently torn in adult-acquired flatfoot deformity?
Explanation
Question 76
A cyclist presents with numbness in the ring and small fingers along with weakness in finger abduction and adduction. Sensory examination reveals normal sensation over the dorso-ulnar aspect of the hand. Where is the most likely site of compression?
Explanation
Question 77
An overhead throwing athlete sustains a tear of the ulnar collateral ligament (UCL) of the elbow. The anterior bundle of the UCL is the primary restraint to valgus stress. Where does the anterior bundle insert on the ulna?
Explanation
Question 78
An anatomic repair of a distal biceps tendon rupture requires reattachment to its native footprint. Which of the following best describes the normal anatomical insertion of the distal biceps tendon?
Explanation
Question 79
A 25-year-old sustains a bucket-handle tear of the medial meniscus. The surgeon decides to repair the tear, relying on the vascularity of the peripheral meniscus. Which arteries provide the primary blood supply to the peripheral menisci?
Explanation
Question 80
During a lateral approach to the calcaneus for an open reduction and internal fixation of a calcaneal fracture, the sural nerve is at risk. What is the typical course of the sural nerve at the level of the lateral malleolus?
Explanation
Question 81
The central band of the interosseous membrane is critical for longitudinal radioulnar stability, particularly after a radial head excision. What is the anatomical orientation of the central band fibers?
Explanation
Question 82
The Lisfranc ligament is crucial for midfoot stability. Between which two bones does the true Lisfranc ligament run?
Explanation
Question 83
When performing an open reduction and internal fixation of a proximal humerus fracture via a deltopectoral approach, the surgeon must be aware of the axillary nerve. How far distal to the lateral edge of the acromion does the axillary nerve typically cross the humerus?
Explanation
Question 84
The plantar fascia is a primary static stabilizer of the longitudinal arch of the foot. It originates from the calcaneal tuberosity and inserts distally. Which band of the plantar fascia is the most robust and most commonly involved in plantar fasciitis?
Explanation
Question 85
A weightlifter sustains a complete rupture of the pectoralis major tendon at its insertion. To perform an anatomic repair, the surgeon must understand its bilaminar insertion. Which segment of the muscle forms the posterior lamina of the insertion?
Explanation
Question 86
A 24-year-old male sustains a posterior shoulder dislocation. After reduction, he exhibits numbness over the lateral aspect of his shoulder and weak shoulder abduction. The injured nerve exits the axilla through a space bounded by which of the following structures?
Explanation
Question 87
During an anterolateral (Watson-Jones) approach to the hip for a total hip arthroplasty, the surgical interval lies between the tensor fasciae latae and the gluteus medius. What is the innervation of the muscles defining this interval?
Explanation
Question 88
A patient presents with a severe palmar laceration resulting in the loss of extension at the proximal and distal interphalangeal joints of the index and middle fingers. The lumbrical muscles to these specific digits are uniquely characterized by which of the following features?
Explanation
Question 89
A 22-year-old male sustains a minimally displaced scaphoid waist fracture. Which of the following best describes the primary arterial supply jeopardized by this injury, predisposing him to avascular necrosis of the proximal pole?
Explanation
Question 90
A 45-year-old female presents with adult-acquired flatfoot deformity. The primary static stabilizer of the talonavicular joint is the spring ligament. Which of the following defines the exact anatomic attachments of this ligament?
Explanation
Question 91
During an anterior cervical discectomy and fusion (ACDF) at C5-C6, the surgeon elevates the longus colli muscles. Injury to the sympathetic trunk in this region can cause Horner's syndrome. Where is the cervical sympathetic trunk typically located relative to the longus colli?
Explanation
Question 92
A 30-year-old athlete undergoes surgical reconstruction of the posterolateral corner (PLC) of the knee. The popliteus tendon must be anatomically secured. What is the normal anatomic insertion of the popliteus tendon on the femur?
Explanation
Question 93
During a modified Stoppa approach for an anterior column acetabular fracture, significant bleeding is encountered from the "corona mortis". This vascular structure represents an anastomosis between which two vascular systems?
Explanation
Question 94
A professional volleyball player presents with isolated atrophy and weakness of the infraspinatus muscle. Supraspinatus strength and muscle bulk are entirely normal. Where is the most likely site of nerve entrapment?
Explanation
Question 95
A continuous saphenous nerve block is placed in the adductor (Hunter's) canal for postoperative analgesia after total knee arthroplasty. Which of the following muscles forms the anterolateral border of this anatomic canal?
Explanation
Question 96
During a medial epicondylectomy for severe cubital tunnel syndrome, the surgeon releases the compressive structures overlying the ulnar nerve. Which of the following forms the primary roof of the cubital tunnel?
Explanation
Question 97
During open reduction and internal fixation of a severe medial malleolus fracture, the surgeon dissects posterior to the medial malleolus. In what order, from anterior to posterior, do the structures normally lie in this region?
Explanation
Question 98
The anterior cruciate ligament (ACL) is composed of two primary anatomic bundles. When the knee is in full extension, what is the relative tension state of these bundles?
Explanation
Question 99
During a posterior triceps-splitting approach to the humerus for fracture fixation, the radial nerve is identified. At what approximate distance proximal to the lateral epicondyle does the radial nerve typically pierce the lateral intermuscular septum?
Explanation
Question 100
A 45-year-old male with an MRI-confirmed L4-L5 paracentral disc herniation is evaluated in the clinic. Based on typical neuroanatomy, this lesion will most likely produce which of the following distinct clinical findings?
Explanation
None
