AAOS & ABOS Anatomy MCQs (Set 2): Musculoskeletal, Neuro, & Regional Topography for Board Review

Key Takeaway
This high-yield question set for AAOS/ABOS exams focuses on critical musculoskeletal anatomy, including bone landmarks, joint structures, and muscle actions. It also covers peripheral nerve pathways and key regional topographic anatomy essential for surgical understanding and diagnostic skills, specifically for Set 2.
AAOS & ABOS Anatomy MCQs (Set 2): Musculoskeletal, Neuro, & Regional Topography for Board Review
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figure 14 shows a lateral radiograph of a knee joint. The bony structure indicated by the arrow is a sesamoid bone that resides in what tendon?

Explanation
Question 2
Talar compression syndrome in ballet dancers typically involves injury to which of the following structures?

Explanation
Question 3
The sartorius muscle is innervated by which of the following nerves?

Explanation
Question 4
Pacinian corpuscles are lamellated nerve endings that are responsible for providing the perception of

Explanation
Question 5
An elite gymnast injured her ankle in an awkward dismount 36 hours ago. Examination reveals weakness on single leg step-up. A clinical photograph of the medial ankle is shown in Figure 15. Plain radiographs are normal. To help confirm the diagnosis, the next step in evaluation should consist of

Explanation
Question 6
Figure 16 shows an axial MRI scan through the knee joint. What structure is identified by the arrow?

Explanation
Question 7
Which of the following nerves is most commonly injured when obtaining a bone graft from the posterior ilium?

Explanation
Question 8
Based on the findings seen in the posteroanterior radiograph of the wrist shown in Figure 17, which of the following structures is torn?

Explanation
Question 9
What tendon has an intra-articular (instrasynovial) location in the knee joint?

Explanation
Question 10
A patient undergoes hip arthroscopy, and the pathology is seen in Figure 18. What is the most likely diagnosis?

Explanation
Question 11
Figure 19 shows an arthroscopic view from the anterior lateral portal of the knee looking into the suprapatella pouch. The use of an electrothermal device during this procedure most commonly causes significant postoperative complications by damaging which of the following structures?

Explanation
Question 12
Figure 20 shows the resting and stress radiographs of a patient who has had pain and feelings of instability after undergoing a total knee arthroplasty 1 year ago. Which of the following ligaments is not functional and is therefore responsible for the patient's symptoms?

Explanation
Question 13
On MRI, a nonsanguinous effusion has what appearance?

Explanation
Question 14
Which of the following illustrations shown in Figures 21a through 21e correctly shows the projection of the sacroiliac joint on the outer table of the ilium?
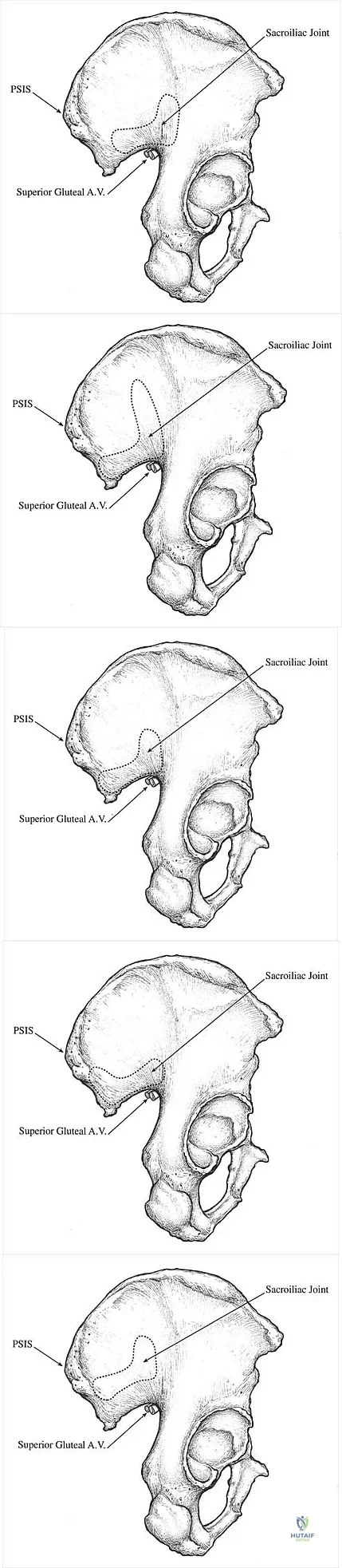
Explanation
Question 15
In children between the ages of 4 and 8 years, the major blood supply to the femoral head comes from the
Explanation
Question 16
What is the most anatomic location for placement of the femoral tunnel in anterior cruciate ligament reconstruction?

Explanation
Question 17
In the anterior approach (Smith-Petersen) to the hip, dissection is carried out between muscles innervated by the

Explanation
Question 18
What structure is marked Q in the diagram of the brachial plexus shown in Figure 22?

Explanation
Question 19
A sagittal T1-weighted MRI scan of the knee joint is shown in Figure 23. What structure is identified by the arrow?

Explanation
Question 20
Figure 24 shows the arthroscopic view of a patient with ankle impingement syndrome. This is commonly seen after high ankle sprains and represents fibrotic granulation thickening of what structure?

Explanation
Question 21
The modified Brostrom lateral ankle ligamentous reconstruction uses which of the following structures to provide supplementary stabilization?

Explanation
Question 22
Figure 25 shows an arthroscopic thermal capsular shrinkage device being used in the anterior inferior quadrant of a patient with a subluxating shoulder. Which of the following neurologic complications is most frequently reported with this technique?

Explanation
Question 23
A coronal MRI scan through the shoulder joint is shown in Figure 26. The cyst indicated by the arrow will most likely cause compression of what nerve?

Explanation
Question 24
Which of the following ligaments is most commonly involved in posterolateral rotatory instability of the elbow?

Explanation
Question 25
Which of the following anatomic structures is labeled 6 in Figure 27?

Explanation
Question 26
During a deltopectoral approach to the shoulder, the cephalic vein is identified. Which of the following is the most appropriate management of the cephalic vein to preserve its primary venous drainage?
Explanation
Question 27
A patient sustains a midshaft humerus fracture. Which of the following structures is at greatest risk of injury as it passes through the lateral intermuscular septum?
Explanation
Question 28
In the anterior approach to the hip (Smith-Petersen), the internervous plane is between muscles supplied by which two nerves?
Explanation
Question 29
During an open reduction and internal fixation of a distal radius fracture via a volar approach (Henry), the flexor carpi radialis (FCR) is retracted medially. The surgeon must be careful to avoid injury to which of the following structures immediately ulnar to the FCR tendon?
Explanation
Question 30
The Martin-Gruber anastomosis most commonly involves a transfer of motor nerve fibers from the:
Explanation
Question 31
Which of the following structures forms the roof of the cubital tunnel?
Explanation
Question 32
During a posterolateral approach to the tibia, the surgeon develops a plane between the lateral and superficial posterior compartments. Which nerve is at risk if dissection strays too far anteriorly into the lateral compartment?
Explanation
Question 33
A 45-year-old male presents with weakness in thumb extension and index finger extension following a radial head fracture. Sensation in the first web space is normal. Compression of the involved nerve most commonly occurs at which of the following structures?
Explanation
Question 34
The medial femoral circumflex artery (MFCA) provides the primary blood supply to the adult femoral head. Which of the following muscles must be protected during a posterior approach to the hip to avoid injury to the deep branch of the MFCA?
Explanation
Question 35
A surgeon is performing an anterolateral approach to the distal femur. The internervous plane is between the vastus lateralis and the rectus femoris. What is the innervation of these two muscles?
Explanation
Question 36
During surgical release of De Quervain's tenosynovitis, the surgeon must identify and protect branches of which of the following nerves to avoid painful neuroma formation?
Explanation
Question 37
A patient demonstrates an inability to actively cross their legs (adduct the hip) following pelvic trauma. Which of the following nerves is most likely injured?
Explanation
Question 38
During placement of a retrograde intramedullary nail for a femur fracture, the starting point is made in the intercondylar notch. The surgeon must be careful to avoid injuring which of the following ligamentous structures that attaches to the medial aspect of the lateral femoral condyle?
Explanation
Question 39
During a lateral approach to the calcaneus for open reduction internal fixation of a calcaneal fracture, the sural nerve is at risk. What is the anatomical course of the sural nerve at the level of the lateral malleolus?
Explanation
Question 40
A patient with a displaced surgical neck fracture of the humerus is found to have weakness of the deltoid and loss of sensation over the lateral aspect of the shoulder. Which of the following spaces does the injured nerve pass through to exit the axilla?
Explanation
Question 41
The major arterial supply to the talus enters the bone through the tarsal canal. This artery is a branch of which of the following vessels?
Explanation
Question 42
During carpal tunnel release surgery, the recurrent motor branch of the median nerve must be avoided. What is the most common anatomical variation of this branch relative to the transverse carpal ligament?
Explanation
Question 43
A patient presents with a deep infection of the midpalmar space. The infection is most likely to spread proximally into the forearm via which of the following structures?
Explanation
Question 44
During an ilioinguinal approach to the acetabulum, the external iliac vessels are mobilized. Which of the following structures is at greatest risk of injury when working in the middle window of this approach?
Explanation
Question 45
Which of the following tendons is contained within the third extensor compartment of the wrist?
Explanation
Question 46
During a lateral approach to the fibula, the superficial peroneal nerve is at risk of iatrogenic injury. At what approximate location does this nerve typically pierce the crural fascia to become subcutaneous?
Explanation
Question 47
A patient presents with winging of the scapula and an inability to elevate the shoulder above 90 degrees following a diagnostic lymph node biopsy in the posterior cervical triangle. Injury to which of the following nerves is the most likely cause?
Explanation
Question 48
During an anterior approach to the hip, knowledge of the lumbar plexus is essential. The femoral nerve is formed by which of the following combinations of nerve roots?
Explanation
Question 49
Which of the following neurovascular structures pass through the quadrangular space of the shoulder?
Explanation
Question 50
The ulnar nerve passes through Guyon's canal at the wrist. Which of the following structures forms the floor of this canal?
Explanation
Question 51
A Martin-Gruber anastomosis is a well-documented anatomical variant. This anomaly most commonly involves the transfer of motor fibers from which nerve to which nerve?
Explanation
Question 52
The superficial medial collateral ligament (sMCL) is a primary static stabilizer of the knee. What is the precise location of its distal attachment?
Explanation
Question 53
The medial plantar nerve provides motor innervation to a specific subset of intrinsic foot muscles. Which of the following muscles is innervated by the medial plantar nerve?
Explanation
Question 54
The proximal pole of the scaphoid is notoriously susceptible to avascular necrosis following fracture. The major blood supply to the proximal pole enters the scaphoid at which anatomical location?
Explanation
Question 55
Lanz classified the anatomical variations of the recurrent motor branch of the median nerve. Which of the following is the most common anatomic path of this branch?
Explanation
Question 56
During the anterior (Henry) approach to the proximal radius, the posterior interosseous nerve (PIN) must be protected. Which muscle is fully supinated to carry the PIN away from the surgical field?
Explanation
Question 57
From anterior to posterior, what is the correct sequence of structures passing behind the medial malleolus within the tarsal tunnel?
Explanation
Question 58
The upper and lower subscapular nerves provide critical motor innervation to the subscapularis muscle. These nerves originate from which specific portion of the brachial plexus?
Explanation
Question 59
Displaced fractures of the talar neck frequently result in osteonecrosis of the talar body due to disruption of its vascular supply. Which artery provides the primary blood supply to the body of the talus?
Explanation
Question 60
The sural nerve is frequently harvested for nerve grafts. It is typically formed by the union of the medial sural cutaneous nerve and the sural communicating branch of the lateral sural cutaneous nerve. The lateral sural cutaneous nerve is a direct branch of which nerve?
Explanation
Question 61
The anterior cruciate ligament (ACL) is composed of two primary bundles. In which position is the anteromedial (AM) bundle under the greatest tension?
Explanation
Question 62
Lister's tubercle serves as a bony fulcrum for a major extensor tendon of the wrist and hand. This tendon resides in which dorsal extensor compartment?
Explanation
Question 63
The radial nerve descends in the spiral groove of the humerus. At approximately what distance proximal to the radiocapitellar joint line does the radial nerve pierce the lateral intermuscular septum to enter the anterior compartment?
Explanation
Question 64
The pectoralis major muscle has a complex bilaminar insertion onto the lateral lip of the bicipital groove. Which statement correctly describes the distinct anatomy of its sternocostal head insertion?
Explanation
Question 65
Which of the following genicular arteries passes anterior to the popliteus muscle and proximal to the head of the fibula, playing a key role in the knee's collateral circulation?
Explanation
Question 66
During an ulnar nerve transposition, the medial intermuscular septum is excised to prevent compression of the nerve. What structure is most at risk of injury when excising this septum?
Explanation
Question 67
Which two tendons intersect at the Master Knot of Henry in the plantar aspect of the midfoot?
Explanation
Question 68
At what cervical level does the vertebral artery typically enter the transverse foramen?
Explanation
Question 69
The medial femoral circumflex artery (MFCA) provides the primary blood supply to the adult femoral head. Between which two muscles does its deep branch travel to reach the posterior capsule?
Explanation
Question 70
Which of the following structures is NOT a border or content of the rotator interval?
Explanation
Question 71
The posterior interosseous nerve (PIN) passes between the two heads of which muscle?
Explanation
Question 72
In the popliteal fossa, what is the anatomical relationship of the popliteal artery to the popliteal vein and tibial nerve?
Explanation
Question 73
What is the most radial structure within the carpal tunnel?
Explanation
Question 74
The "corona mortis" is an anomalous vascular anastomosis that is at risk during the ilioinguinal approach to the acetabulum. It connects which two vascular systems?
Explanation
Question 75
The lumbrical muscles of the hand originate from the tendons of the flexor digitorum profundus. Which nerve typically innervates the first and second lumbricals?
Explanation
Question 76
Which of the following structures form the borders of the quadrilateral space in the shoulder?
Explanation
Question 77
Approximately how many centimeters proximal to the lateral malleolus does the superficial peroneal nerve pierce the crural fascia to become subcutaneous?
Explanation
Question 78
The floor of the cubital tunnel is formed by which of the following structures?
Explanation
Question 79
The medial plantar nerve provides motor innervation to which of the following muscles?
Explanation
Question 80
Which ligament is considered the primary restraint to anterior translation of the distal fibula relative to the tibia?
Explanation
Question 81
The saphenous nerve exits the adductor (Hunter's) canal by piercing which structure?
Explanation
Question 82
The posterior cord of the brachial plexus gives rise to all of the following nerves EXCEPT:
Explanation
Question 83
During a lateral transpsoas approach to the lumbar spine, which nerve is most at risk of injury when retracting the psoas muscle posteriorly at the L4-L5 disc space?
Explanation
Question 84
The suprascapular nerve passes through the suprascapular notch and then the spinoglenoid notch. At the spinoglenoid notch, it is accompanied by which blood vessel?
Explanation
Question 85
Which structure passes intra-articularly through a hiatus between the lateral meniscus and the posterolateral joint capsule?
Explanation
Question 86
During a posterior approach to the humerus, the radial nerve is at risk as it pierces the lateral intermuscular septum to enter the anterior compartment. On average, what is the distance from the lateral epicondyle to this point of penetration?
Explanation
Question 87
Which of the following structures forms the superior border of the quadrilateral space in the shoulder?
Explanation
Question 88
A surgeon is performing a standard anterior (Smith-Petersen) approach to the hip. To prevent denervation of the tensor fasciae latae (TFL), the dissection should remain superficial to what nerve?
Explanation
Question 89
The lumbrical muscles of the hand play a key role in fine motor movements by flexing the metacarpophalangeal joints and extending the interphalangeal joints. Which of the following best describes the typical origin and innervation of the third lumbrical?
Explanation
Question 90
To protect the posterior interosseous nerve (PIN) during an anterior (Henry) approach to the proximal radius, the forearm should be positioned in what way and why?
Explanation
Question 91
The corona mortis is a critical vascular anastomosis that can cause life-threatening hemorrhage during pelvic surgery, particularly during the ilioinguinal approach. It represents a connection between which two vascular systems?
Explanation
Question 92
Avascular necrosis of the talus is a well-known complication of talar neck fractures due to its tenuous blood supply. Which structure serves as the primary blood supply to the talar body?
Explanation
Question 93
A 35-year-old male sustains a midshaft clavicle fracture. During open reduction and internal fixation, the surgeon must be mindful of the underlying neurovascular structures. Which of the following structures is most closely applied to the posterior-inferior aspect of the middle third of the clavicle?
Explanation
Question 94
In the cervical spine, the vertebral artery typically enters the transverse foramen at which vertebral level?
Explanation
Question 95
During an open carpal tunnel release, the recurrent motor branch of the median nerve must be avoided. In a standard textbook description (extraligamentous origin), where does this branch typically originate and how does it course?
Explanation
None
