Orthopedic Anatomy 2026 MCQs: Board Review Questions & Answers (Part 2)
Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Orthopedic Anatomy 2026 MCQs: Board Review Questions & Answers (Part 2). Top-rated Orthopedic Anatomy 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Anatomy 2026 MCQs: Board Review Questions & Answers (Part 2)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
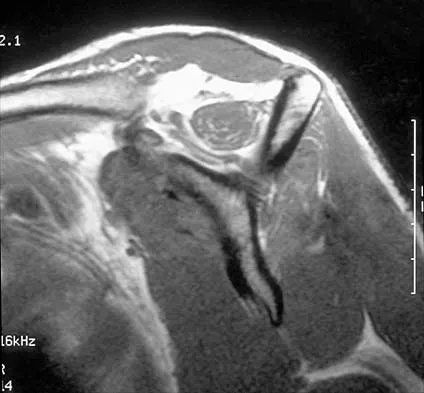
A 25-year-old tennis player has shoulder pain and weakness to external rotation. MRI scans are shown in Figures 16a and 16b. What is the most likely cause of his weakness?
Explanation
Question 2
The posterior approach to the proximal radius uses what intermuscular interval?
Explanation
Question 3
Which of the following statements best describes the anatomic considerations of the popliteal artery posterior to the knee joint?
Explanation
Question 4
A 62-year-old woman reports diffuse aches and pains of the hip and pelvis. She denies any significant trauma but does have a history of chronic anemia. Figure 17a shows a radiograph of the pelvis, and Figures 17b and 17c show T2-weighted MRI scans. What is the most likely diagnosis?
Explanation
Question 5
Involvement of what single muscle best distinguishes an L5 radiculopathy from a peroneal neuropathy?
Explanation
Question 6
What structure is located at the tip of the arrow in Figure 18?
Explanation
Question 7
A patient undergoes the procedure shown in Figure 19. An important part of this procedure is preservation of what wrist ligament?
Explanation
Question 8
A 23-year-old woman reports right knee pain and fullness. The pain is worse with activity but also present at rest. Radiographs are shown in Figures 20a and 20b. What is the most likely diagnosis?
Explanation
Question 9
What is the structure indicated by the letter "A" in Figure 21?
Explanation
Question 10
A 16-year-old boy sustains a twisting injury to the left knee while wrestling. MRI scans are shown in Figures 22a through 22c. What is the most likely diagnosis?
Explanation
Question 11
A 48-year-old woman reports bilateral thigh pain that is limiting her function as a librarian. A radiograph and a bone scan are shown in Figures 23a and 23b. What is the most likely diagnosis?
Explanation
Question 12
At the level of tibial bone resection in total knee arthroplasty, where does the common peroneal nerve lie?
Explanation
Question 13
Figures 24a through 24c show the coronal T1-weighted, T2-weighted fat-saturated, and T1-weighted fat-saturated gadolinium MRI scans of the proximal thigh of a 52-year-old woman who reports a mass in the medial thigh and groin area. She notes that the fullness has grown in size over the course of many months. Based on these findings, what is the most likely diagnosis?
Explanation
Question 14
The arrows in the axial T1-weighted MRI scan shown in Figure 25 show which of the following structures?
Explanation
Question 15
An 82-year-old man has had episodic right thigh pain after undergoing a total hip arthroplasty 10 years ago. Initial postoperative radiographs are shown in Figures 26a and 26b, and current radiographs are shown in Figures 26c and 26d. What is the most likely cause of his pain?
Explanation
Question 16
A 37-year-old patient with type I diabetes mellitus has a flexor tenosynovitis of the thumb flexor tendon sheath following a kitchen knife puncture wound to the volar aspect of the thumb. Left unattended, this infection will likely first spread proximally creating an abscess in which of the following spaces of the palm?
Explanation
Question 17
What tendon is closest to an appropriately placed anterolateral portal for ankle arthroscopy?
Explanation
Question 18
A 52-year-old woman reports nagging shoulder pain that has been present for months and is slowly progressive in nature. The patient also reports nocturnal pain and notes that the pain is not activity related. Figures 27a and 27b show the radiograph and bone scan, and Figures 27c through 27e show T1-weighted, T2-weighted, and gadolinium MRI scans, respectively. Based on these findings, what is the most likely diagnosis?
Explanation
Question 19
Figure 28 shows an arthroscopic view of a right shoulder in the lateral position through a posterior portal. What is the area between structure B (biceps) and SS (subscapularis tendon)?
Explanation
Question 20
New painful paresthesias near the site of the incision after an ulnar nerve transposition is the result of injury to what nerve?
Explanation
Question 21
A 23-year-old man reports pain on the superior aspect of his right shoulder with repetitive overhead activities and when lying on his right side. Figure 29 shows an axial MRI scan. What is the most likely diagnosis based on the MRI findings?
Explanation
Question 22
Following a chevron bunionectomy performed through a dorsal approach, a patient has persistent numbness on the dorsal and medial aspect of the hallux. What nerve has most likely been injured?
Explanation
Question 23
A 74-year-old man reports progressive left hip pain with weight-bearing activities. A radiograph is shown in Figure 30. What is the most likely underlying diagnosis?
Explanation
Question 24
The anatomy of the sciatic nerve as it exits the pelvis is best described as exiting through the
Explanation
Question 25
What complication is more likely following excessive medial retraction of the anterior covering structures during the anterolateral (Watson-Jones) approach to the hip?
Explanation
Question 26
During a surgical dislocation of the hip, the surgeon must protect the deep branch of the medial femoral circumflex artery (MFCA). What is the anatomical path of this vessel as it courses toward the femoral head?
Explanation
Question 27
A patient sustains a midshaft radius fracture, and a volar (Henry) approach is chosen for fixation. What is the internervous plane for the proximal third of this approach?
Explanation
Question 28
A surgeon is performing an open Latarjet procedure. Which nerve is most at risk during the coracoid osteotomy and subsequent mobilization of the conjoined tendon?
Explanation
Question 29
During reconstruction of the posterolateral corner of the knee, the surgeon identifies the popliteofibular ligament. Which of the following accurately describes the origin and insertion of this structure?
Explanation
Question 30
When establishing the anterolateral portal for ankle arthroscopy, the surgeon must be careful to avoid injuring a nerve that supplies sensation to the dorsum of the foot. Which nerve is this?
Explanation
Question 31
Which pulleys in the flexor tendon sheath of the digits are most critical to preserve in order to prevent mechanical bowstringing?
Explanation
Question 32
A patient presents with weakness in elbow flexion and forearm supination, but normal shoulder abduction and normal wrist extension. Which neural structure is most likely injured?
Explanation
Question 33
Which two tendons cross at the anatomical landmark known as the Master Knot of Henry in the plantar aspect of the foot?
Explanation
Question 34
When placing lumbar pedicle screws using standard open anatomical landmarks, what is the accepted entry point?
Explanation
Question 35
The anterior bundle of the ulnar collateral ligament (UCL) of the elbow is the primary restraint to valgus stress. How do the distinct bands of the anterior bundle function during elbow range of motion?
Explanation
Question 36
In total hip arthroplasty, placement of a screw in the anteroinferior quadrant of the acetabulum puts which of the following structures at greatest risk?
Explanation
Question 37
During a posterior approach to the proximal humerus for a nonunion, you are identifying the axillary nerve in the quadrilateral space. Which of the following defines the superior border of this space when viewed posteriorly?
Explanation
Question 38
A 45-year-old man undergoes an open reduction and internal fixation of a midshaft clavicle fracture. Postoperatively, he notes numbness over the anterolateral aspect of his shoulder. Which nerve was most likely injured during the procedure?
Explanation
Question 39
A surgeon is performing an extensile lateral approach to the calcaneus. The sural nerve is at risk during this exposure. The sural nerve is typically formed by the junction of the medial sural cutaneous nerve and the communicating branch of which nerve?
Explanation
Question 40
When utilizing the standard anterolateral (Watson-Jones) approach to the hip, what is the intermuscular internervous interval?
Explanation
Question 41
A patient sustains a posterior shoulder dislocation, and MRI reveals an isolated tear of the teres minor. During a posterior surgical approach, the surgeon must identify the quadrangular space. Which of the following best describes the inferior boundary of this space?
Explanation
Question 42
During a pectoralis major tendon repair following a weightlifting injury, the surgeon must recreate its anatomic insertion. Which of the following best describes the insertion of the sternal head of the pectoralis major?
Explanation
Question 43
Where is the main arterial supply to the femoral head most vulnerable during a posterior approach to the hip (Kocher-Langenbeck)?
Explanation
Question 44
During an anterolateral approach to the distal tibia for plating a pilon fracture, the surgeon must protect the superficial peroneal nerve. At what average distance proximal to the tip of the lateral malleolus does this nerve typically pierce the deep fascia to become superficial?
Explanation
Question 45
A patient undergoes percutaneous repair of an acute Achilles tendon rupture. To avoid trapping the sural nerve with a lateral suture pass, the surgeon must be aware of its anatomic course. Where does the sural nerve typically cross the lateral border of the Achilles tendon?
Explanation
Question 46
A 45-year-old man presents with numbness in his ring and small fingers and weakness in his intrinsic hand muscles. EMG testing localizes compression of the ulnar nerve in the distal arm. Which of the following structures is most likely responsible for this compression?
Explanation
Question 47
A 30-year-old man sustains a closed tibial shaft fracture and develops compartment syndrome. During a four-compartment fasciotomy, the deep posterior compartment must be released. Which of the following muscles is NOT located in the deep posterior compartment of the leg?
Explanation
Question 48
A 25-year-old woman presents with dorsal wrist pain with extension. Examination reveals swelling and tenderness over the 4th dorsal extensor compartment. Which of the following structures are contained within this compartment?
Explanation
Question 49
During an anterior (Smith-Petersen) approach to the hip, an internervous plane is utilized. Which of the following best describes the innervation of the muscles defining the superficial boundary of this plane?
Explanation
Question 50
A 28-year-old athlete sustains a multi-ligament knee injury. Examination reveals a positive dial test at 30 degrees of flexion but normal at 90 degrees. Injury to the posterolateral corner (PLC) is suspected. Which of the following structures attaches to the anteromedial aspect of the fibular styloid?
Explanation
Question 51
A 32-year-old overhead throwing athlete presents with poorly localized posterior shoulder pain and deltoid weakness. MRI reveals atrophy of the teres minor. Which of the following defines the borders of the space where the affected neurovascular bundle is likely compressed?
Explanation
Question 52
While performing an ilioinguinal approach for an anterior column acetabular fracture, significant hemorrhage is encountered posterior to the superior pubic ramus. This is most likely due to an injury to the "corona mortis", which is an anastomosis between which two vessel systems?
Explanation
Question 53
A 12-year-old child presents with vague forearm pain and weakness in thumb flexion and forearm pronation. Radiographs reveal a bony spur on the anteromedial humerus, 5 cm proximal to the medial epicondyle. Which structure is most likely compressed by the ligament connecting this spur to the medial epicondyle?
Explanation
Question 54
During a transforaminal endoscopic lumbar discectomy, the surgeon navigates instruments through Kambin's triangle to safely access the disc space. Which of the following structures forms the anterior border of Kambin's triangle?
Explanation
Question 55
A cyclist presents with weakness in finger abduction and adduction, but normal sensation in the little and ring fingers. A lesion in Guyon's canal is suspected. At which specific zone of Guyon's canal is the compression most likely located?
Explanation
Question 56
A 28-year-old volleyball player has weakness in external rotation of the shoulder. Examination shows atrophy of the infraspinatus but normal bulk of the supraspinatus. Sensation is intact. Where is the most likely site of nerve compression?
Explanation
Question 57
During a surgical approach to the midfoot for an accessory navicular excision, the surgeon identifies a tendinous crossover beneath the navicular. At this location, known as the Master Knot of Henry, which anatomical relationship is correct?
Explanation
Question 58
The volar approach to the proximal radius (Henry approach) requires dissection between two muscles to expose the supinator. Which of the following nerves innervates the muscle forming the medial border of this proximal internervous plane?
Explanation
Question 59
A 45-year-old patient sustains a nondisplaced distal radius fracture and is treated in a cast. Six weeks later, she presents with sudden inability to extend her thumb interphalangeal joint. The ruptured tendon normally travels in which extensor compartment, and what is its radial boundary?
Explanation
Question 60
The lateral femoral cutaneous nerve (LFCN) is at risk during anterior pelvic approaches. In the most common anatomical variant, where does the LFCN pass in relation to the anterior superior iliac spine (ASIS) and inguinal ligament?
Explanation
Question 61
In a patient with tarsal tunnel syndrome, a release of the flexor retinaculum is planned. From anterior to posterior, what is the correct order of structures passing behind the medial malleolus?
Explanation
Question 62
During operative fixation of an ankle fracture, a surgeon evaluates the distal tibiofibular syndesmosis. The anterior inferior tibiofibular ligament (AITFL) originates from the Chaput tubercle. On which bone is the Chaput tubercle located, and where does the AITFL insert?
Explanation
Question 63
During the Smith-Petersen (anterior) approach to the hip, which internervous interval is utilized superficially?
Explanation
Question 64
Hypertrophy of the teres minor, teres major, long head of the triceps, and the surgical neck of the humerus creates a tight quadrangular space. Which of the following structures are at highest risk of compression?
Explanation
Question 65
Which of the following statements most accurately describes the primary blood supply to the scaphoid, predisposing it to proximal pole avascular necrosis?
Explanation
Question 66
The volar (Henry) approach to the proximal radius utilizes an internervous interval between which two muscles?
Explanation
Question 67
Within Guyon's canal, the ulnar nerve bifurcates into superficial and deep branches. The deep branch dives into the hand by passing between which two muscular structures?
Explanation
Question 68
What is the correct anatomic order of structures passing behind the medial malleolus within the tarsal tunnel, strictly from anterior to posterior?
Explanation
Question 69
The femoral attachment (footprint) of the anterior cruciate ligament (ACL) is anatomically located on the:
Explanation
Question 70
During a posterolateral approach to the ankle for fixation of a posterior malleolus fracture, the sural nerve is at risk. It typically courses distally in close proximity to which vascular structure?
Explanation
Question 71
The predominant blood supply to the adult femoral head is provided by the:
Explanation
Question 72
The roof of the cubital tunnel, which can become tightened and compress the ulnar nerve during elbow flexion, is formed by which structure?
Explanation
Question 73
When placing a pedicle screw in the lumbar spine, the anatomic starting point is best described as the intersection of the:
Explanation
Question 74
The rotator interval is a clinically important anatomical space in the shoulder. What are its superior and inferior borders?
Explanation
Question 75
Entrapment of the deep peroneal nerve beneath the inferior extensor retinaculum (anterior tarsal tunnel syndrome) typically causes isolated sensory loss in which anatomic area?
Explanation
Question 76
During a standard deltopectoral approach to the shoulder, the cephalic vein is typically identified and retracted in which direction to best preserve its primary venous drainage?
Explanation
Question 77
The flexor digitorum superficialis (FDS) tendon bifurcates at the level of the proximal phalanx to allow the flexor digitorum profundus (FDP) tendon to pass through. What is the anatomic term for this bifurcation structure?
Explanation
Question 78
During a posterolateral corner reconstruction of the knee, identifying the femoral footprints of the stabilizing structures is crucial. What is the anatomic relationship of the popliteus tendon (PT) insertion relative to the fibular collateral ligament (FCL) origin on the lateral femoral condyle?
Explanation
Question 79
The anterior approach to the hip (Smith-Petersen) utilizes a superficial internervous plane between two muscles. Which of the following nerves innervate these two muscles?
Explanation
Question 80
A 40-year-old patient undergoes a lymph node biopsy in the posterior cervical triangle. Postoperatively, she cannot abduct her shoulder beyond 90 degrees and has lateral scapular winging. Which of the following muscles is primarily denervated?
Explanation
Question 81
When performing an anterolateral approach to the distal humerus, the radial nerve is at risk. Approximately how far proximal to the radiocapitellar joint does the radial nerve piece the lateral intermuscular septum?
Explanation
Question 82
A 32-year-old male sustains a displaced talar neck fracture. Which of the following blood vessels provides the predominant blood supply to the talar body and is most at risk of disruption in this injury?
Explanation
Question 83
A 28-year-old volleyball player presents with posterior shoulder pain and deltoid weakness. MRI reveals isolated atrophy of the teres minor. Which of the following defines the superior boundary of the anatomic space where the affected nerve is compressed?
Explanation
Question 84
The extended volar approach to the radius (Henry approach) requires dissection between the flexor carpi radialis (FCR) and the brachioradialis. Which nerve innervates the muscle forming the lateral border of this interval?
Explanation
Question 85
During an anterior approach to the pelvis for a periacetabular osteotomy, the lateral femoral cutaneous nerve is at risk. What is its most common anatomic relationship to the anterior superior iliac spine (ASIS)?
Explanation
Question 86
A patient presents with isolated weakness in elbow flexion and decreased sensation over the lateral forearm following a traction injury. The affected nerve is formed by which cords of the brachial plexus?
Explanation
Question 87
Displaced scaphoid waist fractures have a high rate of avascular necrosis due to retrograde blood flow. What artery provides the primary blood supply to the proximal pole of the scaphoid?
Explanation
Question 88
During the ilioinguinal approach for an anterior column acetabular fracture, significant hemorrhage occurs behind the superior pubic ramus. This is most likely due to an injury to the "corona mortis", which represents an anastomosis between the:
Explanation
Question 89
The anterior inferior tibiofibular ligament (AITFL) is frequently injured in rotational ankle sprains. What is the eponym for the bony avulsion of the AITFL from its fibular attachment?
Explanation
Question 90
An extensile lateral approach is planned for an intra-articular calcaneus fracture. The sural nerve is at risk during the posterior limb of the incision. What venous structure accompanies the sural nerve posterior to the lateral malleolus?
Explanation
Question 91
When performing a posteromedial approach to the knee to repair the posterior horn of the medial meniscus, the sartorius fascia must be incised. Which of the following correctly identifies the anterior-to-posterior arrangement of the pes anserinus tendons?
Explanation
Question 92
During an in situ ulnar nerve decompression at the cubital tunnel, the first branch of the ulnar nerve identified just distal to the medial epicondyle provides motor innervation to which muscle?
Explanation
Question 93
A patient undergoing arthroscopic rotator cuff repair receives an interscalene nerve block and subsequently develops transient hemidiaphragmatic paresis. The affected nerve shares its primary segmental root origin with which of the following nerves?
Explanation
Question 94
During a dorsal approach to the wrist, the extensor pollicis longus (EPL) is released from its compartment and retracted radially. Around which bony landmark does the EPL normally pivot to change its mechanical line of pull?
Explanation
Question 95
In reconstructive hand surgery, preserving or reconstructing certain flexor pulleys is essential to prevent bowstringing of the flexor tendons. Which two annular pulleys are considered biomechanically most critical?
Explanation
None
