Orthopedic Anatomy 2026 MCQs: Board Review Questions & Answers (Part 4)
Key Takeaway
This topic focuses on Orthopedic Anatomy 2026 MCQs: Board Review Questions & Answers (Part 4), Top-rated Orthopedic Anatomy 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Anatomy 2026 MCQs: Board Review Questions & Answers (Part 4)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figure 42 is a transverse MRI scan of the left shoulder. The arrow points to which of the following structures?
Explanation
Question 2
Within the menisci, the majority of the large collagen fiber bundles are oriented in what configuration?
Explanation
Question 3
For halo traction, what is the preferred site for anterior pin placement?
Explanation
Question 4
A 12-year-old boy has had progressive pain and flatfeet for the past year. Pain is increased with weight-bearing activities. Examination reveals that subtalar motion is absent. On standing, the patient has obvious hindfoot valgus and loss of the normal arch bilaterally. Plain radiographs are shown in Figures 43a through 43c, and a CT scan is shown in Figure 43d. What is the most likely diagnosis?
Explanation
Question 5
When performing ankle arthroscopy through the anterolateral portal, what anatomic structure is at greatest risk?
Explanation
Question 6
Figure 44 shows the AP radiograph of the hip of a patient who underwent screw fixation of the acetabulum. Which of the following structures is at least risk for injury during screw placement in the acetabular component?
Explanation
Question 7
Figure 45 shows the lateral radiograph of a 19-year-old swimmer who has had back pain for the past 2 months. What is the most likely diagnosis?
Explanation
Question 8
Figure 46 shows the AP radiograph of a patient with right shoulder pain. What is the most likely diagnosis?
Explanation
Question 9
The main arterial supply to the humeral head is provided by which of the following arteries?
Explanation
Question 10
Figure 47 shows a transverse MRI scan of a patient's left shoulder. The findings reveal which of the following abnormalities?
Explanation
Question 11
An 18-year-old man sustains an injury to the right brachial plexus after falling off his bicycle. Examination reveals no rhomboideus major or minor muscle function. This finding most likely indicates a preganglionic injury to which of the following nerve roots?
Explanation
Question 12
A 53-year-old man with a history of severe left hip pain has a significant limp that is the result of a 5-cm limb-length discrepancy. An AP radiograph is shown in Figure 48. The underlying etiology is most likely related to a history of
Explanation
Question 13
Where does the median nerve pass in the proximal forearm?
Explanation
Question 14
The vascularity of the digital flexor tendons is significantly richer in what cross-sectional region?
Explanation
Question 15
Figures 49a and 49b show MRI scans of the shoulder. What is the most likely diagnosis?
Explanation
Question 16
A fracture of the radial head is surgically exposed using a posterolateral approach to the elbow. Once the radial head is exposed, how should the arm be positioned to best protect the posterior interosseous nerve from injury?
Explanation
Question 17
Figure 50 shows the MRI scan of a 20-year-old female college soccer player with knee pain. What is the most likely diagnosis?
Explanation
Question 18
The tibiofibular overlap used to diagnose syndesmotic diastasis on an AP view is most commonly measured between the
Explanation
Question 19
Figures 51a and 51b show subluxation of the
Explanation
Question 20
The so-called high ankle sprain from an external rotation mechanism of injury typically involves injury to which of the following structures?
Explanation
Question 21
In the first dorsal compartment of the wrist, what tendon most frequently contains multiple slips?
Explanation
Question 22
The preferred surgical approach to the elbow of a child with an irreducible type III supracondylar distal humerus fracture and pulseless extremity is through which of the following muscle intervals?
Explanation
Question 23
A 48-year-old man has recurrent right knee pain. Figure 52a shows the sagittal proton density T2-weighted MRI scan, and Figure 52b shows the sagittal T2-weighted MRI scan at the same level. The arrow is pointing to a
Explanation
Question 24
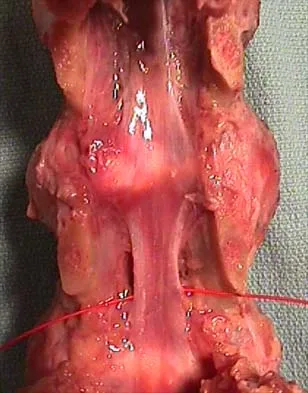
Figure 53 shows a thoracolumbar specimen as viewed from posterior to anterior following removal of all posterior elements. Which of the following structures does the red string pass under?
Explanation
Question 25
A 5-year-old girl sustained a comminuted Salter-Harris type IV fracture of the left distal tibia 2 years ago. The AP radiograph shown in Figure 54a reveals a growth arrest and a 1.4-cm limb-length discrepancy. The ankle is in approximately 20 degrees of varus. Figure 54b shows a coronal reconstruction image of the distal tibial physis, and Figure 54c shows a sagittal reconstruction image of the same area. On the sagittal reconstruction image, the bar extends from the 9-mm mark to the 24-mm mark in 3-mm increments. On the coronal image, the bar extends from the 9-mm mark to the 24-mm mark, also in 3-mm increments. A map of the physeal bar based on these measurements is shown in Figure 54d. Initial treatment should consist of
Explanation
Question 26
A 45-year-old male presents with an inability to extend his thumb and digits at the metacarpophalangeal joints. Wrist extension is preserved but deviates radially. He has no sensory deficits. The most likely site of nerve compression is:
Explanation
Question 27
What is the primary blood supply to the body of the talus?
Explanation
Question 28
During a posterior approach to the hip, preserving the insertion of which of the following muscles protects the deep branch of the medial femoral circumflex artery (MFCA)?
Explanation
Question 29
A 24-year-old man sustains a scaphoid waist fracture. He is at high risk for avascular necrosis of the proximal pole. The primary blood supply to the proximal pole of the scaphoid is derived from which of the following arteries?
Explanation
Question 30
A 28-year-old pitcher presents with vague posterior shoulder pain and isolated atrophy of the teres minor. An MRI demonstrates a paralabral cyst in the quadrilateral space. Which of the following borders the quadrilateral space superiorly?
Explanation
Question 31
A 32-year-old volleyball player has weakness in external rotation of the shoulder. Examination reveals isolated atrophy of the infraspinatus without supraspinatus involvement. Entrapment of the suprascapular nerve at the spinoglenoid notch is typically associated with which of the following?
Explanation
Question 32
A 45-year-old woman presents with vague forearm pain, weakness of the flexor pollicis longus, and numbness in the radial three and a half digits. Radiographs show a bony spur on the anteromedial distal humerus. Which structure is compressed as it passes under the Ligament of Struthers?
Explanation
Question 33
A spine surgeon is performing a posterior cervical foraminotomy at C6-C7. Understanding the vascular anatomy of the cervical spine is critical to prevent iatrogenic injury. Which of the following is true regarding the transverse foramen of the C7 vertebra?
Explanation
Question 34
A 20-year-old collegiate baseball pitcher reports medial elbow pain during the late cocking phase of throwing. He is diagnosed with a UCL injury. Which bundle of the ulnar collateral ligament is the primary restraint to valgus stress between 30 and 120 degrees of flexion?
Explanation
Question 35
A 30-year-old man falls from a height and sustains a displaced talar neck fracture (Hawkins Type III). He is at high risk for osteonecrosis. The major blood supply to the body of the talus is provided by the artery of the tarsal canal, which is a branch of which artery?
Explanation
Question 36
A 42-year-old bodybuilder hears a "pop" in his antecubital fossa while performing heavy deadlifts. He has a reverse Popeye sign and weakness in forearm supination. The distal biceps tendon inserts onto which of the following structures?
Explanation
Question 37
A 55-year-old diabetic woman presents with burning pain and tingling in the plantar aspect of her foot, which worsens at night. Tinel's sign is positive posterior to the medial malleolus. The structure responsible for compressing the nerve in this syndrome is the:
Explanation
Question 38
A 60-year-old woman presents with a progressive flatfoot deformity. Examination reveals a loss of the medial longitudinal arch and a positive too-many-toes sign. Which ligament is considered the primary static stabilizer of the talonavicular joint and medial longitudinal arch?
Explanation
Question 39
A 22-year-old football player sustains a non-contact pivoting injury to his knee. Radiographs reveal an avulsion fracture of the lateral tibial plateau (Segond fracture). This radiographic finding is considered pathognomonic for an anterior cruciate ligament tear and represents an avulsion of which structure?
Explanation
Question 40
A surgeon is performing a lateral compartment fasciotomy for chronic exertional compartment syndrome. To avoid injuring the superficial peroneal nerve, the surgeon must be aware that the nerve typically pierces the deep fascia to become subcutaneous at what location?
Explanation
Question 41
A 72-year-old woman sustains a displaced femoral neck fracture. She is counseled on the high risk of avascular necrosis and nonunion. The primary blood supply to the adult femoral head comes from the:
Explanation
Question 42
A 35-year-old man sustains a spiral fracture of the distal third of the humeral shaft. On presentation, he is unable to extend his wrist or fingers. Which structure is at highest risk of entrapment or injury in this specific fracture pattern?
Explanation
Question 43
A 45-year-old woman with rheumatoid arthritis presents with an inability to extend her thumb. She is diagnosed with a ruptured extensor pollicis longus (EPL) tendon. The EPL tendon travels through which extensor compartment of the wrist, and what bony landmark serves as a pulley for it?
Explanation
Question 44
A surgeon is utilizing the volar (Henry) approach to the proximal radius for open reduction and internal fixation of a radius fracture. Supination of the forearm during this approach protects which nerve by moving it radially and away from the surgical field?
Explanation
Question 45
A 30-year-old swimmer undergoes shoulder arthroscopy for instability. The surgeon evaluates the rotator interval, an anatomical space in the anterior shoulder. Which of the following tendons forms the inferior border of the rotator interval?
Explanation
Question 46
During a volar (Henry) approach to the proximal radius, what structure marks the proximal edge of the superficial layer of the supinator muscle where the posterior interosseous nerve enters?
Explanation
Question 47
In percutaneous or minimally invasive repairs of the Achilles tendon, sutures passed through the proximal-lateral aspect of the tendon are most likely to injure which nerve?
Explanation
Question 48
During an arthroscopic procedure for adhesive capsulitis, the surgeon releases the structures within the rotator interval. Which of the following anatomic structures forms the superior border of this interval?
Explanation
Question 49
During a lateral approach to the humerus, the radial nerve is at risk as it pierces the lateral intermuscular septum. At approximately what distance proximal to the lateral epicondyle does this occur?
Explanation
Question 50
The medial femoral circumflex artery (MFCA) provides the primary blood supply to the adult femoral head. The deep branch of the MFCA typically courses between which two muscles?
Explanation
Question 51
A patient presents with an isolated compression neuropathy of the posterior interosseous nerve (PIN). The most common site of compression is the arcade of Frohse, which is formed by the proximal tendinous edge of which muscle?
Explanation
Question 52
During knee flexion, what is the normal biomechanical tension pattern of the anteromedial (AM) and posterolateral (PL) bundles of the anterior cruciate ligament (ACL)?
Explanation
Question 53
A surgeon is performing an Achilles tendon repair and wishes to avoid injury to the sural nerve. The sural nerve typically crosses the lateral border of the Achilles tendon at approximately what distance proximal to the calcaneal insertion?
Explanation
Question 54
Within the medial retromalleolar space (tarsal tunnel), the posterior tibial artery and tibial nerve are located between the tendons of which two muscles?
Explanation
Question 55
Which component of the deltoid ligament complex is considered the strongest and serves as the primary restraint to external rotation and anterolateral displacement of the talus?
Explanation
Question 56
The proximal pole of the scaphoid is highly susceptible to avascular necrosis following a fracture due to its retrograde blood supply. The primary vascular contribution enters the scaphoid at which of the following locations?
Explanation
Question 57
During a lateral approach to the fibula for ORIF of an ankle fracture, the superficial peroneal nerve must be protected. This nerve typically pierces the deep fascia to become subcutaneous at what distance proximal to the tip of the lateral malleolus?
Explanation
Question 58
When performing an anterior cervical discectomy and fusion (ACDF), knowledge of the vertebral artery's course is crucial. Moving from proximal to distal, the vertebral artery typically first enters the foramen transversarium at which cervical level?
Explanation
Question 59
A patient presents with median nerve compression symptoms above the elbow. Imaging reveals a supracondylar process. The ligament of Struthers connects this process to which anatomical structure?
Explanation
Question 60
To prevent neurapraxia on a fracture table, the perineal post must be adequately padded to protect the pudendal nerve. The pudendal nerve exits the pelvis through the greater sciatic foramen and re-enters the perineum through the lesser sciatic foramen by wrapping around the:
Explanation
Question 61
The popliteal artery is at high risk of stretch injury or transection during high-energy knee dislocations. It is particularly vulnerable due to firm tethering proximally at the adductor hiatus and distally at the:
Explanation
Question 62
The ligaments of Humphry and Wrisberg are accessory meniscofemoral ligaments. The ligament of Wrisberg is characterized anatomically as running from the:
Explanation
Question 63
During the Latarjet procedure for recurrent anterior shoulder instability, the musculocutaneous nerve is at risk. It typically pierces the coracobrachialis muscle at what average distance distal to the tip of the coracoid process?
Explanation
Question 64
When preparing for pedicle screw instrumentation in the lumbar spine, understanding the transverse pedicle angulation is critical. How does the medial pedicle angulation in the transverse plane typically change from L1 to L5?
Explanation
Question 65
A patient presents with posterior shoulder pain and selective weakness of external rotation. MRI reveals a large paralabral ganglion cyst isolated to the spinoglenoid notch. Which muscle will exhibit denervation changes?
Explanation
Question 66
The quadrangular space transmits the axillary nerve and posterior circumflex humeral artery. Which muscle forms the inferior anatomical border of this space?
Explanation
Question 67
The pes anserinus insertion on the proximal medial tibia consists of three tendon insertions. From anterior to posterior, what is the correct anatomical order of these tendons?
Explanation
Question 68
During the ilioinguinal approach to the acetabulum, severe hemorrhage can occur if the corona mortis is inadvertently transected. This vascular structure is an anastomosis between the:
Explanation
Question 69
During a volar (Henry) approach to the radius, the surgeon develops the proximal internervous plane. Which of the following describes the correct muscles and their respective innervations for this plane?
Explanation
Question 70
The deltopectoral approach to the shoulder utilizes a true internervous plane. Between which two muscles is this plane located?
Explanation
Question 71
In an adult patient, which of the following vessels provides the predominant blood supply to the femoral head?
Explanation
Question 72
The meniscofemoral ligaments of the knee are anatomically associated with the posterior cruciate ligament (PCL). What is the specific anatomic course of the ligament of Wrisberg?
Explanation
Question 73
The anterior cruciate ligament (ACL) consists of two distinct functional bundles. Which bundle provides the primary restraint to anterior tibial translation when the knee is in 90 degrees of flexion?
Explanation
Question 74
A surgeon is performing a posterior approach to the popliteal fossa. Which of the following structures is located most deeply (closest to the joint capsule)?
Explanation
Question 75
Which of the following describes the correct anatomical pathway of the pudendal nerve as it navigates the pelvis?
Explanation
Question 76
During posterior cervical spine surgery, the suboccipital triangle must be carefully navigated. Which structures are primarily contained within this anatomical boundary?
Explanation
Question 77
In the anatomical layout of the tarsal tunnel at the medial malleolus, which of the following structures is positioned most posteriorly?
Explanation
Question 78
The rotator interval is a triangular anatomical space in the anterior shoulder. Which of the following sets of structures is contained within this interval?
Explanation
Question 79
When decompressing the ulnar nerve at the wrist in Guyon's canal, a precise understanding of the boundaries is essential. Which of the following accurately describes a boundary of Guyon's canal?
Explanation
Question 80
The radial nerve is highly susceptible to injury as it passes through the spiral groove of the humerus. Which vascular structure accompanies the radial nerve in this groove?
Explanation
Question 81
In evaluating a brachial plexus injury, knowledge of the cord formations is critical. The posterior cord is formed by the union of which of the following?
Explanation
Question 82
The lateral collateral ligament (LCL) of the knee is a critical structure for stability. What is its primary biomechanical function?
Explanation
Question 83
Which of the following defines the correct origins of the femoral nerve within the lumbar plexus?
Explanation
Question 84
During surgical approach to the medial elbow, the flexor-pronator mass is encountered originating from the medial epicondyle. Which muscle has the most proximal and lateral origin on the medial epicondyle?
Explanation
Question 85
Avascular necrosis of the scaphoid after fracture is highly dependent on its specific arterial supply. Which statement accurately describes the primary blood supply to the scaphoid?
Explanation
Question 86
In the setting of an ankle syndesmotic injury, which ligament provides the greatest resistance to lateral displacement of the fibula?
Explanation
Question 87
The sciatic nerve typically divides into the tibial and common peroneal nerves in the distal thigh. Which of the following describes the embryologic origins of these two divisions from the sacral plexus?
Explanation
Question 88
When utilizing the extensile lateral approach for open reduction internal fixation of a calcaneus fracture, where should the corner of the L-shaped incision be placed to minimize the risk of flap necrosis?
Explanation
Question 89
Which of the following accurately describes the primary blood supply to the scaphoid, predisposing its proximal pole to avascular necrosis following a fracture?
Explanation
Question 90
When placing a pedicle screw in the lumbar spine, violating the medial cortex of the pedicle places which of the following structures at greatest immediate risk?
Explanation
Question 91
A patient presents with groin pain exacerbated by resisted hip flexion following a total hip arthroplasty. If an oversized acetabular component is impinging on a soft tissue structure anteriorly, which structure is most likely involved?
Explanation
Question 92
During surgical reconstruction of the posterolateral corner of the knee, a surgeon isolates the fibular collateral ligament (FCL). What is the anatomic relationship of the FCL femoral attachment relative to the popliteus tendon femoral attachment?
Explanation
Question 93
A 28-year-old overhead athlete presents with insidious onset of posterior shoulder pain and weakness in external rotation. An MRI reveals isolated atrophy of the teres minor. Compression of which nerve in the quadrilateral space is most likely responsible?
Explanation
Question 94
In a patient with acquired adult flatfoot deformity, progressive failure of the posterior tibial tendon often leads to attenuation of the plantar calcaneonavicular (spring) ligament. Which of the following is the primary attachment site of the superomedial bundle of the spring ligament?
Explanation
Question 95
During a distal biceps tendon repair, the surgeon must reattach the tendon to its anatomical footprint on the radial tuberosity. In which portion of the radial tuberosity does the distal biceps predominantly insert?
Explanation
Question 96
During an anterior intrapelvic (modified Stoppa) approach to the acetabulum, brisk arterial bleeding is encountered near the superior pubic ramus. This is most likely due to injury to an anastomosis between which two vascular systems?
Explanation
Question 97
A rock climber presents with a "bowstringing" deformity of the ring finger flexor tendons following a sudden snap during a dynamic climbing move. Which two annular pulleys are biomechanically most critical to prevent this bowstringing?
Explanation
Question 98
Resection of a large soft tissue sarcoma in the popliteal fossa requires sacrifice of the tibial nerve. What specific post-operative functional deficit will this patient most likely demonstrate?
Explanation
Question 99
During posterior cervical instrumentation, the surgeon must be mindful of the vertebral artery. At which cervical level does the vertebral artery typically enter the transverse foramen?
Explanation
Question 100
To avoid injury to the medial femoral circumflex artery (MFCA) during a posterior approach to the hip, an essential anatomical landmark is the superior border of which muscle?
Explanation
None
