AAOS & ABOS Anatomy MCQs (Set 3): Skeletal, Joint, and Muscle Anatomy | Orthopedic Board Prep
Key Takeaway
This high-yield question set (Set 3) for AAOS, ABOS, and OITE exams covers essential musculoskeletal anatomy. Questions focus on the detailed structures of bones, joints, muscles, and their neurovascular supply, crucial for understanding orthopedic principles and surgical approaches. Ideal for comprehensive board preparation.
AAOS & ABOS Anatomy MCQs (Set 3): Skeletal, Joint, and Muscle Anatomy | Orthopedic Board Prep
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
In the most common condition causing a winged scapula, which of the following nerves is affected?
Explanation
Question 2
A 17-year-old woman seen in the emergency department reports right knee pain and swelling that has progressively worsened over the past several weeks. Radiographs are shown in Figures 31a and 31b. What is the most likely diagnosis?
Explanation
Question 3
A 26-year-old man has had hand pain and progressive swelling in the knuckle for the past several months. He denies any trauma to the hand. The ring finger metacarpophalangeal joint is tender, and there is loss of motion in the digit. Figure 32a shows the radiograph and Figures 32b through 32d show the T1-weighted, T2-weighted, and gadolinium MRI scans, respectively. What is the most likely diagnosis?
Explanation
Question 4
Which of the following best describes the relationship of the median nerve to the flexor carpi radialis tendon just proximal to the carpal canal?
Explanation
Question 5
Which of the following muscles has dual innervation?
Explanation
Question 6
Figure 33a shows a line drawing of a normal hemipelvis. The anterior acetabular rim is bold. Figure 33b illustrates a hemipelvis with a crossover sign, which is indicative of what acetabular pathology?
Explanation
Question 7
Which of the following structures is most vulnerable during a medial sesamoidectomy of the hallux?
Explanation
Question 8
What structure is most at risk for injury from a retractor against the tracheoesophageal junction during an anterior approach to the cervical spine?
Explanation
Question 9
A 40-year-old man has had hip pain with increased activity over the past year. Examination reveals restriction of motion and tenderness with combined hip flexion, adduction, and internal rotation. An AP radiograph is shown in Figure 34. What is the most likely diagnosis?
Explanation
Question 10
Figure 35 shows the radiograph of a 44-year-old woman with rheumatoid arthritis who reports neck pain. Below what threshold number is surgical stabilization warranted for the interval shown by the arrow?
Explanation
Question 11
An axillary nerve lesion may cause weakness in the deltoid and the
Explanation
Question 12
Figure 36 shows an AP radiograph of a 65-year-old man who reports activity-related groin pain. History reveals that he underwent total hip arthroplasty 12 years ago. What is the most likely diagnosis?
Explanation
Question 13
A 21-year-old man who was injured in a snowboarding accident 18 months ago now reports wrist pain. An MRI scan is shown in Figure 37. Based on the image findings, what is the most likely diagnosis?
Explanation
Question 14
An 82-year-old woman reports activity-related knee pain. History reveals that she underwent total knee arthroplasty 16 years ago. AP and lateral radiographs and a bone scan are shown in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
Question 15
Which of the following tendons is found in the same dorsal compartment of the wrist as the posterior interosseous nerve?
Explanation
Question 16
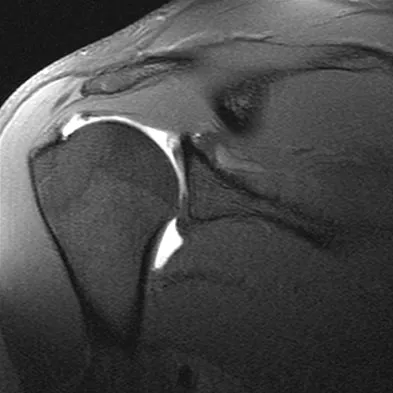
Figures 39a and 39b show the MRI scans of a 25-year-old man with right shoulder pain. Figure 39c shows the arthroscopic view from a posterior portal in the beach chair position. What is the most likely diagnosis?
Explanation
Question 17
The posterior horn of the medial meniscus receives its primary blood supply from what artery?
Explanation
Question 18
In recurrent posterior shoulder instability, what is the recommended approach to the posterior capsule?
Explanation
Question 19
Following ankle arthroscopy performed through a posterolateral portal, a patient notes numbness on the lateral half of the heel pad of the foot. What is the most likely injured structure?
Explanation
Question 20
Figure 40 shows the MRI scan of a 23-year-old man with a history of recurrent anterior shoulder instability. What is the most likely diagnosis?
Explanation
Question 21
Figure 41 shows the MRI scan of a 38-year-old weightlifter. What does the arrow on the MRI scan indicate?
Explanation
Question 22
Which of the following describes the correct proximal to distal progression of the annular and cruciform pulleys of the digits?
Explanation
Question 23
A 75-year-old woman began a walking program 2 months after undergoing right total knee arthroplasty. She had to stop the program after 4 weeks because of hindfoot pain and ankle swelling. Radiographs are shown in Figures 42a and 42b. What is the most likely diagnosis?
Explanation
Question 24
Figure 43 shows an arthroscopic view of a right shoulder through a lateral portal in the beach chair position. The arrow is pointing to what structure?
Explanation
Question 25
In Charcot-Marie-Tooth disease a progressive deformity develops in the foot. Which functional muscles predominate in deformity formation?
Explanation
Question 26
During a surgical approach to the proximal radius, the surgeon plans to expose the radial shaft. To protect the posterior interosseous nerve (PIN), which muscle should be carefully retracted, considering the PIN passes between its two heads?
Explanation
Question 27
During a surgical dislocation of the hip for femoroacetabular impingement, the surgeon must preserve the primary blood supply to the adult femoral head. Which of the following vessels is the most critical to protect?
Explanation
Question 28
The anteromedial (AM) bundle of the anterior cruciate ligament (ACL) is tightest in which of the following positions, and what is its primary function?
Explanation
Question 29
A patient presents with the inability to form a perfect "OK" sign, resulting in a pinch with extended distal interphalangeal (DIP) and interphalangeal (IP) joints. Which nerve is most likely compressed, and which muscle is consequently affected?
Explanation
Question 30
During a direct lateral (Hardinge) approach to the hip, extending the proximal split in the gluteus medius more than 3 to 5 cm proximal to the greater trochanter places which of the following structures at highest risk of injury?
Explanation
Question 31
In the deltopectoral approach to the shoulder, the axillary nerve can be identified at the inferior border of the subscapularis. What is the approximate distance of the axillary nerve from the inferior glenoid labrum at the 6 o'clock position?
Explanation
Question 32
The primary restraint to varus stress at the knee at 30 degrees of flexion is the fibular collateral ligament (FCL). What is the anatomical location of the FCL footprint on the femur relative to the lateral epicondyle?
Explanation
Question 33
During a minimally invasive lateral transpsoas approach to the lumbar spine, which nerve is at greatest risk of iatrogenic injury when working at the L4-L5 disc space?
Explanation
Question 34
In a patient with stage II acquired adult flatfoot deformity, the spring ligament is often attenuated. What are the primary bony attachments of the spring ligament?
Explanation
Question 35
During a posterior approach to the humerus for fracture plating, the radial nerve is identified in the spiral groove. At approximately what distance proximal to the olecranon fossa does the nerve cross the posterior humerus?
Explanation
Question 36
Which of the following ligaments is the strongest and provides the greatest biomechanical resistance to diastasis of the distal tibiofibular syndesmosis?
Explanation
Question 37
The distal biceps tendon normally inserts on the radial tuberosity. To maximize supination strength during a surgical repair of a ruptured tendon, it should be reattached to which specific footprint?
Explanation
Question 38
A cyclist presents with numbness in the little finger and weakness of finger abduction. The ulnar nerve is compressed in Guyon's canal. Which of the following structures forms the floor of Guyon's canal?
Explanation
Question 39
During an ilioinguinal approach to the acetabulum, the "corona mortis" is encountered and must be carefully ligated to prevent catastrophic bleeding. What vessels are connected by the corona mortis?
Explanation
Question 40
A patient presents with shoulder weakness and lateral winging of the scapula following a lymph node biopsy in the posterior triangle of the neck. Which nerve was injured, and which muscle is paralyzed?
Explanation
Question 41
The anterior bundle of the medial collateral ligament (AMCL) of the elbow is the primary restraint to valgus stress. Where is its primary insertion on the proximal ulna?
Explanation
Question 42
The ulnar nerve passes through the cubital tunnel at the elbow. The roof of the cubital tunnel is formed by Osborne's ligament, which anatomically spans between which two structures?
Explanation
Question 43
A professional volleyball player presents with isolated atrophy and weakness of the infraspinatus muscle, with normal supraspinatus strength and bulk. Where is the most likely site of nerve compression?
Explanation
Question 44
The popliteal artery is at risk of injury during a high tibial osteotomy (HTO) or total knee arthroplasty. At the level of the knee joint line, what is the anatomical relationship of the popliteal artery to the vein and nerve?
Explanation
Question 45
During an anterolateral approach to the distal tibia, the superficial peroneal nerve must be protected to prevent painful neuromas. Where does this nerve typically pierce the crural fascia to become subcutaneous?
Explanation
Question 46
A 45-year-old man undergoes a fasciotomy for chronic exertional compartment syndrome of the lateral leg. During the procedure, a nerve that pierces the deep fascia to become subcutaneous is at high risk of injury. Approximately where does this nerve typically exit the deep fascia?
Explanation
Question 47
A patient presents with an inability to form a valid "OK" sign, instead demonstrating a pinch with extended interphalangeal and distal interphalangeal joints of the thumb and index finger. Assuming an isolated anterior interosseous nerve (AIN) palsy, which of the following muscles will maintain intact innervation?
Explanation
Question 48
A 32-year-old woman sustains a displaced talar neck fracture. She is at high risk for avascular necrosis of the talar body due to retrograde blood supply. Which of the following arteries provides the predominant blood supply to the talar body?
Explanation
Question 49
A 35-year-old weightlifter presents with vague posterior shoulder pain and weakness in external rotation. An MRI reveals an isolated cyst compressing a nerve within the quadrangular space. Which of the following muscles forms the superior border of this anatomic space?
Explanation
Question 50
During a posterior approach to the hip for a total hip arthroplasty, the surgeon must be careful to protect the primary blood supply to the femoral head. Which of the following vessels provides the predominant blood supply to the adult femoral head?
Explanation
Question 51
A 24-year-old football player sustains a direct blow to the anteromedial aspect of his knee, resulting in a posterolateral corner (PLC) injury. Which of the following structures is considered one of the three primary static stabilizers of the PLC?
Explanation
Question 52
A rock climber presents with pain and a "bowstringing" deformity of the index finger after feeling a pop. Rupture of which of the following annular pulleys is most biomechanically detrimental to normal finger flexion?
Explanation
Question 53
When placing a pedicle screw in the lumbar spine, the surgeon identifies the starting point at the intersection of the pars interarticularis, the midpoint of the transverse process, and the superior articular facet. Medial breach of the pedicle screw at the L4 vertebral body most directly endangers the dural sac and which of the following nerve roots?
Explanation
Question 54
During a plantar approach for an excision of a plantar fibroma, the surgeon dissects near the Master Knot of Henry. Which two tendons cross at this specific anatomic landmark?
Explanation
Question 55
A 28-year-old gymnast sustains an elbow dislocation. After closed reduction, she has persistent posterolateral rotatory instability (PLRI). Deficiency of which of the following structures is the primary cause of this instability?
Explanation
Question 56
An orthopedic oncologist is performing a resection of a soft tissue sarcoma located within the femoral triangle. Which of the following defines the lateral border of this anatomic region?
Explanation
Question 57
A volar surgical approach to the proximal radius (Henry approach) requires developing an internervous plane. Which of the following muscles is a component of the "mobile wad of Henry" that is retracted laterally during this approach?
Explanation
Question 58
During an endoscopic carpal tunnel release, the surgeon must be aware of the motor branch of the median nerve. Through which of the following mechanisms does this recurrent motor branch most commonly exit the carpal tunnel?
Explanation
Question 59
During an ilioinguinal approach for an anterior column acetabular fracture, significant hemorrhage occurs just posterior to the superior pubic ramus. This is most likely due to an injury to the "corona mortis," which is an anastomosis between which two vascular systems?
Explanation
Question 60
A 25-year-old soccer player is diagnosed with a high ankle sprain. Which of the following ligaments is the strongest and provides the most stability to the distal tibiofibular syndesmosis?
Explanation
Question 61
A patient presents with isolated weakness of the infraspinatus muscle but normal supraspinatus strength. The suprascapular nerve is most likely compressed at which of the following anatomic locations?
Explanation
Question 62
A patient sustains a midshaft humerus fracture and subsequently presents with an inability to extend the wrist and digits, but retains the ability to extend the elbow. Sensation is decreased over the dorsal web space. The injured nerve originates from which cord(s) of the brachial plexus?
Explanation
Question 63
During an ilioinguinal approach to the acetabulum, massive bleeding occurs while dissecting over the superior pubic ramus. Which of the following represents the most likely anatomical source of this hemorrhage?
Explanation
Question 64
A patient sustains a posterior shoulder dislocation and subsequently demonstrates weakness in shoulder external rotation and a sensory deficit over the lateral deltoid. The affected nerve exits the axilla through a space bordered superiorly by which of the following structures?
Explanation
Question 65
A 24-year-old athlete sustains a knee injury resulting in increased external tibial rotation at both 30 and 90 degrees of knee flexion. Which of the following anatomical structures are most likely completely ruptured?
Explanation
Question 66
During flatfoot reconstruction, the surgeon evaluates the plantar calcaneonavicular ligament. This structure, which is a primary static stabilizer of the longitudinal arch, is directly supported plantarly by which of the following tendons?
Explanation
Question 67
To prevent bowstringing of the flexor tendons following a tenolysis procedure in zone II of the hand, the surgeon must preserve which of the following critical annular pulleys?
Explanation
Question 68
A 35-year-old man sustains a severe fall, leading to an Essex-Lopresti lesion. The central band of the interosseous membrane is torn. Which of the following best describes the normal anatomical orientation of the fibers of this central band?
Explanation
Question 69
During a posterior approach to the hip, protecting the primary blood supply to the femoral head is critical. The medial femoral circumflex artery (MFCA) courses deep to which of the following short external rotators?
Explanation
Question 70
A patient presents with weakness in wrist extension and altered sensation over the dorsal web space of the hand. An MRI reveals a herniated cervical disc. Between which two cervical vertebrae is the herniation most likely located?
Explanation
Question 71
The anterior cruciate ligament (ACL) is composed of two primary bundles. In full knee extension, what is the anatomical status of the anteromedial (AM) bundle compared to the posterolateral (PL) bundle?
Explanation
Question 72
A pitcher complains of right shoulder pain and weakness with overhead activities. Examination reveals isolated wasting of the supraspinatus and infraspinatus. Entrapment of the affected nerve is most likely to occur at which of the following anatomical sites?
Explanation
Question 73
A surgeon is performing an open anterior shoulder stabilization and identifies the rotator interval. Which of the following structures is NOT considered a normal anatomical border or content of the rotator interval?
Explanation
Question 74
During surgical release of the tarsal tunnel, the flexor retinaculum is divided. From anterior to posterior, what is the correct anatomical order of the structures passing behind the medial malleolus?
Explanation
Question 75
A patient presents with posterolateral rotatory instability (PLRI) of the elbow following a dislocation. This condition is primarily caused by insufficiency of the lateral ulnar collateral ligament (LUCL). Where does the LUCL anatomically insert?
Explanation
Question 76
A patient undergoes a four-compartment fasciotomy of the leg. The deep posterior compartment is released to decompress its contents. Which of the following neurovascular structures is contained within the deep posterior compartment?
Explanation
Question 77
A 25-year-old gymnast sustains a wrist injury, and an MRI reveals an avulsion of the triangular fibrocartilage complex (TFCC) from its foveal attachment. The fovea of the ulna lies anatomically between which two structures?
Explanation
Question 78
During a deltopectoral approach to the shoulder, the cephalic vein is typically retracted. Which of the following describes the correct internervous plane for this approach?
Explanation
Question 79
A surgeon is performing an anterior (Smith-Petersen) approach to the hip. The superficial surgical interval is between the sartorius and the tensor fasciae latae. What is the internervous plane of this superficial interval?
Explanation
Question 80
During a posterolateral approach to the ankle for fixation of a posterior malleolus fracture, the sural nerve is at risk of iatrogenic injury. What two nerves typically join to form the sural nerve?
Explanation
Question 81
An orthopedic resident is dissecting the posterior shoulder. The quadrangular space transmits the axillary nerve and posterior circumflex humeral artery. Which of the following forms the superior border of this space in a normal anatomic specimen?
Explanation
Question 82
The Thompson (posterolateral) approach to the proximal radius utilizes an internervous plane between which two muscles?
Explanation
Question 83
A 32-year-old man sustains a displaced talar neck fracture (Hawkins Type III). Which of the following provides the primary blood supply to the talar body, placing it at high risk for avascular necrosis?
Explanation
Question 84
During knee arthroscopy, the surgeon visualizes a ligamentous structure originating from the posterior horn of the lateral meniscus and inserting into the lateral aspect of the medial femoral condyle, passing anterior to the PCL. What is this structure?
Explanation
Question 85
Compression of the posterior interosseous nerve (PIN) at the elbow frequently occurs at the Arcade of Frohse. This fibrous arch is formed by the proximal edge of which muscle?
Explanation
Question 86
The blood supply to the scaphoid predominantly enters at which location, making proximal pole fractures particularly susceptible to nonunion?
Explanation
Question 87
During a medial approach to the knee for a medial collateral ligament repair, the infrapatellar branch of the saphenous nerve is transected. What clinical deficit will the patient experience?
Explanation
Question 88
An anterior approach to the humeral shaft utilizes the plane between the biceps brachii and brachialis. During deep dissection, the brachialis muscle is split longitudinally. Which aspect of the split brachialis is retracted laterally to protect the radial nerve?
Explanation
Question 89
During the ilioinguinal approach for an anterior column acetabular fracture, the surgeon develops three surgical "windows." What anatomical structure forms the boundary between the lateral and middle windows?
Explanation
Question 90
A patient sustains a high-energy distal tibia fracture. During a minimally invasive percutaneous plate osteosynthesis (MIPPO) via an anterolateral approach, which nerve is most at risk of iatrogenic injury as it pierces the deep fascia of the leg?
Explanation
Question 91
During the proximal portion of the volar (Henry) approach to the forearm, supination of the forearm is performed to protect a major nerve. Which muscle's insertion is stripped and elevated to expose the proximal radius, and what is the anatomical relationship of the at-risk nerve to this muscle?
Explanation
Question 92
A 28-year-old runner presents with chronic exertional compartment syndrome requiring fasciotomy of the lateral leg compartment. During the fascial release, which nerve is at greatest risk of iatrogenic injury as it exits the deep fascia to become subcutaneous in the distal third of the leg?
Explanation
Question 93
A spine surgeon is performing a lateral transpsoas approach (LLIF) for an L4-L5 interbody fusion. Which of the following nerves emerges on the anterior surface of the psoas major muscle and runs longitudinally, making it particularly vulnerable to injury during initial retractor placement?
Explanation
None
