Orthopedic Anatomy 2026 MCQs: Board Review Questions & Answers (Part 3)
Key Takeaway
Looking for accurate information on Orthopedic Anatomy 2026 MCQs: Board Review Questions & Answers (Part 3)? Top-rated Orthopedic Anatomy 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Anatomy 2026 MCQs: Board Review Questions & Answers (Part 3)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 41-year-old man who plays golf regularly has had ulnar-sided wrist pain for the past several days after striking a tree root with a golf club. Examination reveals significant pain with resisted flexion of the ring and small fingers and tenderness over the hook of the hamate. Which of the following radiographic views would be most helpful in identifying the pathology of this injury?
Explanation
Question 2
What is the primary limiting membrane and mechanical support for the periphery of the physis?
Explanation
Question 3
What normal tissue has a low signal intensity (appears black) on both T1- and T2-weighted images?
Explanation
Question 4
A positive Froment sign indicates weakness of which of the following muscles?
Explanation
Question 5
Figure 28 shows an AP radiograph of a 54-year-old woman who underwent lumbar laminectomy and fusion at the L4 and L5 levels with placement of a bone stimulator 8 years ago. She also underwent a left total hip arthroplasty 2 years ago; aspiration of that joint now reveals that it is infected with a gram-positive cocci organism. History is also significant for IV drug use and human immunodeficiency virus (HIV). The patient reports fever, chills, and left flank and abdominal pain. Examination reveals significant pain with resisted left hip flexion and passive hip extension. She also has lumbar hyperlordosis. Which of the following studies would best identify the underlying cause of her infection?
Explanation
Question 6
A 55-year-old woman who underwent a left total hip arthroplasty 8 months ago using a modified Hardinger approach reports a persistent painless limp. Examination reveals that when she is not using a cane, she lurches to the left during weight bearing on the left lower extremity. An AP radiograph is shown in Figure 29. Which of the following hip muscle groups should be strengthened to improve the gait abnormality?
Explanation
Question 7
Figure 30 shows an axial cross section of extensor tendon anatomy in zone 7 of the wrist. What letter best depicts the location of the posterior interosseous nerve?
Explanation
Question 8
Figures 31a and 31b show the T1- and T2-weighted MRI scans of a patient's knee joint. What is the most likely diagnosis?
Explanation
Question 9
A 15-year-old boy reports feeling a pop and notes sudden giving way of the left knee while playing basketball. He has immediate pain and swelling in the knee. An AP radiograph is shown in Figure 32. A small avulsion fragment from the lateral tibial margin is the only finding. What is the most likely diagnosis?
Explanation
Question 10
What neurovascular structure is most at risk when performing an inside-out repair of the posterior horn of the medial meniscus?
Explanation
Question 11
Figure 33 shows the AP and lateral radiographs of an obese 58-year-old man who underwent a cementless total hip arthroplasty 6 years ago. He reports no pain, and examination reveals a normal gait and painless hip range of motion. What is the most likely diagnosis?
Explanation
Question 12
Which of the following muscles attaches to the coracoid process of the scapula?
Explanation
Question 13
Turf toe typically involves injury to which of the following structures of the great toe?
Explanation
Question 14
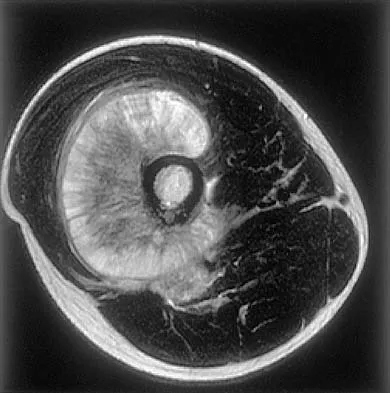
Figures 34a through 34c show an axial proton density (spin echo long TR, short TE) image, a sagittal inversion recovery (STIR) image, and a sagittal T1-weighted (short TR, short TE) image of the left thigh. What is the most likely diagnosis?
Explanation
Question 15
The artery located within the substance of the coracoacromial ligament is a branch of what artery?
Explanation
Question 16
Figures 35a and 35b show the axial T2-weighted and coronal T1-weighted MRI scans of a patient who has enlargement of the right thigh. What is the most likely diagnosis?
Explanation
Question 17
Figures 36a and 36b show the MRI scans of a patient who has shoulder weakness. What is the most likely diagnosis?
Explanation
Question 18
Figure 37 shows the T2-weighted MRI scan of the hip joint. What structure is labeled A?
Explanation
Question 19
The great medullary artery, also known as the Adamkiewicz artery, originates from which of the following arteries?
Explanation
Question 20
A patient who underwent total knee arthroplasty now reports a loss of sensation in the area circled in Figure 38. This area is innervated by which of the following nerves?
Explanation
Question 21
During an anterior approach to the shoulder, excessive traction on the conjoined tendon is most likely to result in loss of
Explanation
Question 22
Figure 39 shows the sagittal T1-weighted MRI scan of a 27-year-old man who twisted his knee 2 weeks ago. The arrow is pointing to
Explanation
Question 23
Figure 40 shows the AP radiograph of a 55-year-old man who reports left knee pain. Which of the following conditions is least likely to produce this radiographic presentation?
Explanation
Question 24
Figure 41 shows the MRI scan of a 39-year-old man who has severe left groin and anterior thigh pain. What is the most likely diagnosis?
Explanation
Question 25
Iliosacral screws placed for stabilization of posterior pelvic ring injuries (eg, sacroiliac dislocation) that exit the sacrum anteriorly are most likely to injure which of the following structures?
Explanation
Question 26
A 28-year-old weightlifter presents with right shoulder pain and weakness in external rotation. An MRI shows an isolated cyst compressing the nerve in the quadrangular space. Which of the following muscles is most likely denervated?
Explanation
Question 27
A 35-year-old sustains a displaced femoral neck fracture. Which of the following arteries provides the majority of the blood supply to the weight-bearing dome of the femoral head?
Explanation
Question 28
A 35-year-old male sustains a displaced talar neck fracture following a motor vehicle accident. Which of the following arteries provides the primary blood supply to the body of the talus, placing it at high risk for avascular necrosis if disrupted?
Explanation
Question 29
A 28-year-old overhead athlete presents with posterior shoulder pain and weakness in external rotation. An MRI shows atrophy of the teres minor. Entrapment of the axillary nerve in the quadrilateral space is suspected. Which of the following structures forms the superior boundary of this space?
Explanation
Question 30
A 6-year-old child presents with a painful elbow after falling from monkey bars. On the true anteroposterior (AP) radiograph of the elbow, which of the following secondary ossification centers should typically be visible?
Explanation
Question 31
During surgical repair of a zone II flexor tendon laceration in the index finger, preservation or reconstruction of specific pulleys is critical to prevent bowstringing. Which two pulleys are considered the most biomechanically essential?
Explanation
Question 32
A 22-year-old football player sustains a direct blow to the anteromedial tibia. Clinical examination reveals increased external tibial rotation at 30 degrees of knee flexion but symmetrical rotation at 90 degrees. Which of the following structures is the primary restraint to external tibial rotation at 30 degrees?
Explanation
Question 33
In a patient presenting with deep gluteal pain and suspected piriformis syndrome, anatomical variations in the sciatic nerve must be considered. What is the most common anatomical variant of the sciatic nerve relative to the piriformis muscle?
Explanation
Question 34
A patient develops acute compartment syndrome in the anterior compartment of the leg following a high-energy tibial shaft fracture. Which of the following sensory deficits would most likely be observed if the nerve traversing this compartment becomes ischemic?
Explanation
Question 35
A 30-year-old motorcyclist sustains a traction injury to the upper trunk of his brachial plexus (C5-C6). Which of the following terminal nerve branches is derived exclusively from the lateral cord?
Explanation
Question 36
A 24-year-old man falls on an outstretched hand and sustains a displaced fracture through the proximal pole of the scaphoid. What anatomical feature of the scaphoid's blood supply predisposes this specific fracture pattern to nonunion and osteonecrosis?
Explanation
Question 37
The intervertebral disc relies on its complex ultrastructure to dissipate axial loads. What is the predominant collagen type found in the healthy nucleus pulposus?
Explanation
Question 38
A microsurgeon is planning to harvest a sural nerve graft for a brachial plexus reconstruction. To safely and efficiently locate the nerve in the distal third of the leg, the surgeon should identify which of the following accompanying structures?
Explanation
Question 39
During a pectoralis major tendon repair following a complete rupture at the musculotendinous junction, the surgeon mobilizes the sternocostal and clavicular heads. What is the normal anatomical insertion pattern of these two heads onto the humerus?
Explanation
Question 40
A 65-year-old patient is undergoing a total hip arthroplasty via the anterior (Smith-Petersen) approach. Which of the following capsular ligaments is the strongest in the body and acts as the primary restraint to hip hyperextension?
Explanation
Question 41
While performing a volar approach to the proximal radius (Henry approach), the surgeon must carefully identify and protect the median nerve. Between which two muscle bellies does the median nerve typically pass as it exits the cubital fossa?
Explanation
Question 42
A 25-year-old motorcyclist sustains a traction injury to his right upper extremity. On examination, he has profound weakness of the intrinsic muscles of the hand and a noticeable ptosis and miosis on the right side of his face. Avulsion of which of the following nerve roots is most likely responsible for these facial findings?
Explanation
Question 43
A 32-year-old man sustains a displaced talar neck fracture (Hawkins type III). Which of the following vessels provides the predominant blood supply to the talar body and is at highest risk of disruption in this injury?
Explanation
Question 44
A 24-year-old pitcher experiences posterior shoulder pain and isolated weakness in external rotation. An MRI reveals a paralabral cyst compressing a nerve within the quadrangular space. Which of the following structures forms the superior border of this space?
Explanation
Question 45
During a knee reconstruction for a multi-ligamentous injury, the surgeon isolates the primary stabilizer to external tibial rotation at 30 degrees of knee flexion. Which of the following structures is being evaluated?
Explanation
Question 46
A 28-year-old professional volleyball player presents with progressive right shoulder weakness. Examination reveals normal shoulder abduction and internal rotation but weakness in external rotation. Atrophy is noted over the posterior scapula, but the supraspinatus fossa appears normal. Compression of the suprascapular nerve is most likely occurring at which location?
Explanation
Question 47
A 45-year-old mechanic presents with an inability to actively extend his fingers at the metacarpophalangeal joints, though he can extend his wrist with radial deviation. Sensation over the dorsum of the hand is completely intact. Where is the most likely site of neural compression?
Explanation
Question 48
In planning a surgical dislocation of the hip for femoroacetabular impingement, the surgeon must protect the primary blood supply to the femoral head. Which of the following represents the primary blood supply to the adult femoral head?
Explanation
Question 49
A patient cannot flex the interphalangeal joint of the thumb and the distal interphalangeal joint of the index finger. Which of the following muscles is also likely to be affected by this specific nerve palsy?
Explanation
Question 50
During a medial meniscal repair, a surgeon places a retractor posteromedially. Postoperatively, the patient reports numbness over the anteromedial aspect of the lower leg. Which of the following nerves was most likely injured as it exited the adductor canal?
Explanation
Question 51
A 30-year-old male sustains a closed midshaft humerus fracture. Examination reveals an inability to extend the wrist and fingers, with decreased sensation over the dorsal web space. The injured nerve penetrates which structure as it transitions from the posterior to the anterior compartment of the arm?
Explanation
Question 52
A patient undergoes fasciotomies for compartment syndrome of the foot following a crush injury. The surgeon plans to release the compartment that contains the quadratus plantae muscle. Which compartment is this?
Explanation
Question 53
In a patient presenting with buttock pain radiating down the posterior thigh, an MRI reveals an anatomic variant where the common peroneal division of the sciatic nerve passes directly through the piriformis muscle, while the tibial division passes below it. What is the approximate prevalence of this anatomic variant?
Explanation
Question 54
A 22-year-old athlete undergoes an arthroscopic medial meniscal repair. Healing is most favorable in the peripheral third of the meniscus. The vascular supply to this region is primarily derived from which of the following?
Explanation
Question 55
A patient presents with proximal median nerve compression. Radiographs reveal a bony exostosis on the anteromedial aspect of the distal humerus. Compression is likely occurring beneath a ligament connecting this exostosis to the medial epicondyle. What is this structure?
Explanation
Question 56
A 65-year-old man with cervical spondylosis sustains a hyperextension injury to his neck. He subsequently develops profound weakness in his upper extremities with relatively preserved motor function in his lower extremities. The pattern of weakness is due to the somatotopic organization of which of the following spinal cord tracts?
Explanation
Question 57
A patient presents with an inability to actively extend the knee and numbness over the anterior thigh and medial calf following a retroperitoneal hematoma. The affected nerve is formed by the posterior divisions of which anterior rami?
Explanation
Question 58
During a posterolateral approach to the distal humerus, the surgeon identifies the radial nerve as it pierces the lateral intermuscular septum. At approximately what distance proximal to the radiocapitellar joint does this occur?
Explanation
Question 59
Which of the following structures forms the medial border of the quadrangular space in the posterior shoulder?
Explanation
Question 60
In an anterior pelvic ring injury requiring internal fixation, the surgeon must be mindful of the "corona mortis". This vascular structure represents an anastomosis between the obturator vessels and branches of which of the following?
Explanation
Question 61
When evaluating a patient with a suspected posterolateral corner (PLC) knee injury, understanding the femoral attachments is crucial for reconstruction. Where does the fibular collateral ligament (FCL) attach on the lateral femoral condyle relative to the popliteus tendon insertion?
Explanation
Question 62
A patient presents with midfoot pain and instability following a fall from a horse. Radiographs show a widened space between the first and second metatarsals. The primary ligament injured in this scenario originates from which bone?
Explanation
Question 63
A 25-year-old male sustains a laceration over the thenar eminence. He demonstrates an inability to oppose the thumb but maintains normal thumb adduction. Which of the following muscles is primarily innervated by the deep branch of the ulnar nerve and remains functional?
Explanation
Question 64
During a far lateral approach to the L4-L5 lumbar spine for a foraminal disc herniation, the exiting nerve root is at risk. Where does the L4 nerve root travel in relation to the L4 pedicle?
Explanation
Question 65
A fracture of the talar neck places the blood supply to the talar body at significant risk. Which artery provides the predominant blood supply to the talar body?
Explanation
Question 66
During a volar Henry approach to the forearm, the surgeon needs to expose the proximal radius. Pronation of the forearm protects the posterior interosseous nerve (PIN). The PIN passes between the two heads of which muscle?
Explanation
Question 67
The superficial palmar arch provides the primary blood supply to the digits and is formed predominantly by the ulnar artery. In which anatomical plane does the superficial palmar arch lie?
Explanation
Question 68
A surgeon is evaluating a patient with recurrent lateral patellar instability and plans to reconstruct the medial patellofemoral ligament (MPFL). Where is the anatomic femoral origin of the MPFL located?
Explanation
Question 69
The alar ligaments play a critical role in stabilizing the craniocervical junction. What is their primary biomechanical function?
Explanation
Question 70
When performing an extensile lateral approach to the calcaneus, the sural nerve is at risk of iatrogenic injury. The sural nerve typically courses parallel and adjacent to which vascular structure in the posterolateral hindfoot?
Explanation
Question 71
A 45-year-old female presents with a distal radius fracture and concurrent severe median nerve neuropathy. During open carpal tunnel release, the surgeon must identify the precise boundaries of the tunnel. Which of the following forms the radial border of the carpal tunnel?
Explanation
Question 72
A patient undergoes a total hip arthroplasty via a direct anterior approach. The surgeon utilizes the true internervous plane between the tensor fasciae latae and the sartorius. Which nerve supplies the tensor fasciae latae?
Explanation
Question 73
A surgeon uses the Smith-Petersen approach for a periacetabular osteotomy. During the deep dissection, the internervous plane is developed between which two muscles?
Explanation
Question 74
A 25-year-old man sustains a proximal pole scaphoid fracture. The risk of avascular necrosis is high due to the retrograde blood supply. Which of the following arteries provides the primary blood supply to the proximal pole of the scaphoid?
Explanation
Question 75
A 32-year-old overhead throwing athlete presents with poorly localized posterior shoulder pain and deltoid weakness. MRI reveals a paralabral cyst in the quadrilateral space. What nerve and artery are most likely compressed?
Explanation
Question 76
Which of the following accurately describes the anatomy and biomechanical properties of the medial meniscus compared to the lateral meniscus?
Explanation
Question 77
In a growing child, most Salter-Harris fractures typically propagate through which specific histologic zone of the physis?
Explanation
Question 78
A surgeon is performing an arthroscopic rotator interval closure for shoulder instability. Which of the following structures form the superior and inferior borders of the rotator interval, respectively?
Explanation
Question 79
A 24-year-old man develops compartment syndrome of the forearm following a crush injury. The surgeon plans a volar release. Which of the following muscles is included in the mobile wad of Henry?
Explanation
Question 80
A 65-year-old woman sustains a displaced femoral neck fracture. Which of the following arteries provides the predominant blood supply to the weight-bearing dome of the femoral head in an adult?
Explanation
Question 81
Which ligament is anatomically the strongest component of the distal tibiofibular syndesmotic complex?
Explanation
Question 82
A baseball pitcher undergoes reconstruction of the ulnar collateral ligament (UCL) of the elbow. Which bundle of the UCL is the primary restraint to valgus stress at 90 degrees of elbow flexion?
Explanation
Question 83
During a pinch mechanism, the adductor pollicis muscle is tested (Froment's sign). This muscle is innervated by the deep branch of the ulnar nerve. Where does the transverse head of the adductor pollicis originate?
Explanation
Question 84
An 18-year-old gymnast complains of chronic lower back pain. Radiographs reveal a pars interarticularis defect (spondylolysis). Anatomically, the pars interarticularis is a bony bridge located between which two structures?
Explanation
Question 85
A 30-year-old man sustains a Hawkins Type III talar neck fracture. Which of the following arteries represents the major source of blood supply to the body of the talus?
Explanation
Question 86
A patient sustains a midshaft humerus fracture and presents with a wrist drop. The radial nerve is at highest risk where it pierces the lateral intermuscular septum. At what approximate distance proximal to the lateral epicondyle does the radial nerve pierce the septum?
Explanation
Question 87
A patient with De Quervain's tenosynovitis undergoes surgical release. The surgeon must be cautious of septal variations within the first dorsal extensor compartment. Which tendons reside in this compartment?
Explanation
Question 88
During an anterior surgical approach to the acetabulum (ilioinguinal approach), severe bleeding is encountered behind the superior pubic ramus. This is most likely due to an injury to the 'corona mortis.' The corona mortis is an anastomosis between which two vascular systems?
Explanation
Question 89
A 22-year-old soccer player ruptures her anterior cruciate ligament (ACL). The ACL is composed of two primary bundles. In which position is the anteromedial (AM) bundle of the ACL most taut?
Explanation
Question 90
The lumbrical muscles of the hand are unique because they originate from tendons and insert onto tendons. Which of the following accurately describes the typical innervation pattern of the lumbricals?
Explanation
Question 91
A 35-year-old runner sustains an inversion ankle injury resulting in an avulsion fracture of the base of the fifth metatarsal. The tendon responsible for this avulsion fragment belongs to which muscle?
Explanation
Question 92
A 45-year-old mechanic presents with weakness in extending his fingers and thumb, but normal wrist extension (with radial deviation). Sensation is entirely intact. He is diagnosed with Posterior Interosseous Nerve (PIN) syndrome. What is the most common anatomical site of PIN compression?
Explanation
Question 93
A 25-year-old professional rugby player undergoes posterolateral corner reconstruction of the knee. The surgeon identifies the popliteofibular ligament (PFL) as a critical structure to reconstruct for rotational stability. What is the correct anatomical origin and insertion of the native PFL?
Explanation
Question 94
During a dorsal approach to the wrist for a scaphoid nonunion repair, the surgeon uses Lister's tubercle as a landmark. Which of the following tendons utilizes this bony prominence as a mechanical pulley to redirect its line of pull?
Explanation
Question 95
A 30-year-old overhead throwing athlete presents with vague posterior shoulder pain. An MRI reveals isolated atrophy of the teres minor. Compression of the axillary nerve within the quadrilateral space is suspected. What are the true anatomical borders of this space?
Explanation
Question 96
During an anterior intrapelvic (modified Stoppa) approach for an acetabular fracture, massive hemorrhage can occur if a vascular anastomosis crossing over the superior pubic ramus is injured. This structure, known as the corona mortis, connects which two vascular systems?
Explanation
Question 97
A spine surgeon is planning freehand placement of thoracic pedicle screws for a severe scoliosis deformity. Understanding pedicle morphometry is critical to avoid spinal cord or vascular injury. In the normal thoracic spine, which level typically has the narrowest pedicle diameter in the transverse (mediolateral) plane?
Explanation
Question 98
A 45-year-old woman with stage IIb posterior tibial tendon dysfunction is undergoing flatfoot reconstruction. The surgeon plans a spring ligament reconstruction. Which of the following components of the spring ligament complex is the thickest and most critical for supporting the head of the talus?
Explanation
Question 99
A 28-year-old elite volleyball player presents with painless weakness in shoulder external rotation. Clinical examination demonstrates isolated atrophy of the infraspinatus, with normal bulk and strength of the supraspinatus. Entrapment of the suprascapular nerve is most likely occurring at which anatomical location?
Explanation
Question 100
A 32-year-old man develops acute compartment syndrome of the leg following a high-energy tibial shaft fracture. A dual-incision, four-compartment fasciotomy is performed. During release of the deep posterior compartment, which specific muscle is most frequently missed and inadequately decompressed?
Explanation
None
