Orthopedic Anatomy 2026 MCQs: Board Review Questions & Answers (Part 1)

Key Takeaway
Here are the crucial details you must know about Orthopedic Anatomy 2026 MCQs: Board Review Questions & Answers (Part 1). Top-rated Orthopedic Anatomy 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Anatomy 2026 MCQs: Board Review Questions & Answers (Part 1)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
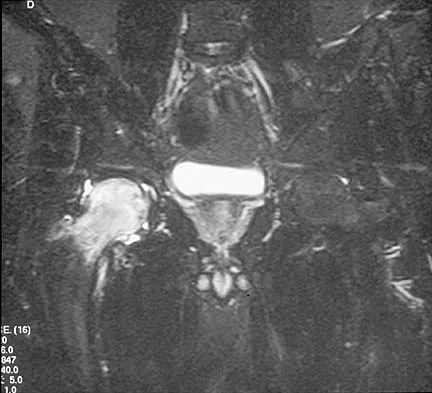
A 65-year-old man with ankylosing spondylitis sustains an extension injury to his cervical spine. Two days later, a progressive neurologic deficit develops at the C6 level. An MRI scan is shown in Figure 1. What is the most likely diagnosis?
Explanation
Question 2
What are the most common portals for arthroscopic surgery of the ankle?
Explanation
Question 3
A patient who underwent primary total hip arthroplasty 7 years ago that resulted in excellent pain relief and a normal gait now reports pain and a limp. Postoperative and current AP radiographs are shown in Figures 2a and 2b. What is the most likely cause of the pathology seen?
Explanation
Question 4
The safest surgical approach to the insertion of the tibial posterior cruciate ligament uses the interval between which of the following muscles?
Explanation
Question 5
A 50-year-old man with no history of trauma reports new-onset back pain after doing some yard work the previous day. He reports pain radiating down his leg posteriorly and into the first dorsal web space of his foot. MRI scans are shown in Figures 3a through 3c. What nerve root is affected?
Explanation
Question 6
A 19-year-old wrestler has numbness along the radial aspect of the forearm after undergoing an open Bankart repair through an anterior deltopectoral approach. Motor weakness would be expected along with what other finding?
Explanation
Question 7
A 19-year-old man has had intermittent progressive knee pain with ambulation and pain at night following a rodeo accident 4 weeks ago. Figures 4a through 4e show the radiographs, a bone scan, CT scan, and T2-weighted MRI scan. What is the most likely diagnosis?
Explanation
Question 8
Figures 5a and 5b show the radiographs of an active 52-year-old man who has increasing knee pain and progressive varus deformity after undergoing total knee arthroplasty 7 years ago. Examination reveals a small effusion, but he has good motion and stability. What is the most likely diagnosis?
Explanation
Question 9
Which of the following best describes the course of the median nerve at the elbow?
Explanation
Question 10
A 62-year-old woman with soft-tissue calcifications and telangiectasia has severe pain in the left index, middle, ring, and little fingers. History reveals that she does not smoke. The clinical history and arteriogram shown in Figure 6 are consistent with which of the following conditions?
Explanation
Question 11
During excision of a Baker cyst, the base or stalk is usually found between the
Explanation
Question 12
A direct lateral (Hardinge) approach is used during total hip arthroplasty. The structure labeled A in Figure 7 is the
Explanation
Question 13
The dorsal digital cutaneous nerve of the great toe shown in Figure 8 is a branch of what nerve?
Explanation
Question 14
In hip arthroplasty, the location of the medial femoral circumflex artery is best described as
Explanation
Question 15
A 47-year-old man has acute right shoulder pain after falling off a ladder. The MRI scan shown in Figure 9 reveals
Explanation
Question 16
The oblique radiograph of the foot and the CT scan shown in Figures 10a and 10b show a patient whose symptoms have failed to respond to rest and non-steroidal anti-inflammatory drugs. What is the best course of action?
Explanation
Question 17
What is the typical MRI signal intensity of bone marrow affected by acute osteomyelitis?
Explanation
Question 18
Based on the appearance of the imaging studies shown in Figures 11a through 11c, what structure has most likely been injured?
Explanation
Question 19
In the anterior forearm approach to the distal radius (Henry approach), the radial artery is located between what two structures?
Explanation
Question 20
Following a radial nerve neurapraxia at or above the elbow, return of muscle function can be expected to start at the brachioradialis and return along which of the following progressions?
Explanation
Question 21
To preserve blood supply to the fractured bone seen in Figures 12a and 12b, care should be taken when exposing which of the following areas?
Explanation
Question 22
An axial T1-weighted MRI scan of the pelvis is shown in Figure 13. The arrow is pointing to what muscle?
Explanation
Question 23
Which of the following radiographic views best depicts a Hill-Sachs defect?
Explanation
Question 24
What structure provides the major blood supply to the humeral head?
Explanation
Question 25
Figure 14 shows an intra-articular gadolinium-enhanced MRI scan of a 52-year-old woman who has stopped playing tennis because of pain in her left shoulder while serving. What is the most likely diagnosis?
Explanation
Question 26
A 35-year-old male presents with an inability to actively extend his fingers at the metacarpophalangeal joints following a proximal radius fracture. Wrist extension is preserved but deviates radially. Sensation in the hand is completely normal. Where is the most likely site of nerve compression or injury?
Explanation
Question 27
During an ilioinguinal approach for an anterior column acetabular fracture, the surgeon is exposing the posterior aspect of the superior pubic ramus. Massive hemorrhage is suddenly encountered. This bleeding is most likely due to an anomalous vascular connection between which two vessels?
Explanation
Question 28
A 28-year-old overhead athlete presents with insidious onset of poorly localized posterior shoulder pain and paresthesias over the lateral aspect of the deltoid. Examination reveals isolated atrophy of the teres minor. The structure responsible for the patient's symptoms passes through a space bounded by which of the following structures?
Explanation
Question 29
A 45-year-old female is undergoing an anterolateral approach to the distal tibia for a pilon fracture plating. To avoid iatrogenic injury to the superficial peroneal nerve, the surgeon must be aware of its typical anatomical course. At what approximate distance from the tip of the lateral malleolus does the superficial peroneal nerve typically pierce the crural fascia to become subcutaneous?
Explanation
Question 30
A 32-year-old elite volleyball player complains of right shoulder pain and weakness. An MRI demonstrates a large paralabral cyst causing isolated compression at the spinoglenoid notch. Physical examination is most likely to demonstrate weakness in which of the following motions, and normal strength in which?
Explanation
Question 31
Following a complete laceration of the median nerve at the level of the antecubital fossa, a patient retains some motor function of the intrinsic muscles of the hand normally innervated by the ulnar nerve. Electrodiagnostic testing confirms an anomalous nerve communication. The Martin-Gruber anastomosis most commonly involves nerve fibers crossing from the:
Explanation
Question 32
A surgeon is utilizing Schöttle's point on a true lateral fluoroscopic view of the knee to determine the precise femoral attachment for a medial patellofemoral ligament (MPFL) reconstruction graft. According to Schöttle's radiographic landmarks, the correct femoral attachment is located:
Explanation
Question 33
A 42-year-old distance runner presents with chronic, recalcitrant midfoot pain and paresthesias radiating into the plantar aspect of the medial toes. You suspect entrapment of the medial plantar nerve at the Master Knot of Henry. Anatomically, which two tendons cross at this specific location?
Explanation
Question 34
A 24-year-old rugby player sustains a severe contact injury to his knee, resulting in a grade 3 posterolateral corner (PLC) tear. The surgeon plans an anatomical reconstruction. Which of the following correctly describes the normal anatomical relationship of the fibular collateral ligament (FCL) and the popliteus tendon (PT) at their femoral insertions on the lateral epicondyle?
Explanation
Question 35
A 55-year-old woman undergoes a minimally invasive lateral transpsoas approach to the lumbar spine (LLIF) for an L4-L5 degenerative spondylolisthesis. Postoperatively, she experiences profound weakness in knee extension and numbness over the anterior aspect of her thigh. Which of the following nerves was most likely injured, and what is its normal anatomical location relative to the psoas major muscle at the L4-L5 disc level?
Explanation
Question 36
A 45-year-old female is undergoing a periacetabular osteotomy (PAO) via the anterior (Smith-Petersen) approach to the hip. The surgeon develops the superficial interval between the sartorius and the tensor fasciae latae. During this dissection, a significant vascular structure crossing the operative field must be identified and ligated to prevent hemorrhagic complications. Which of the following vessels is this?
Explanation
Question 37
A 25-year-old professional football player requires an anatomic posterolateral corner (PLC) reconstruction of the knee. During the preparation of the femoral tunnel for the popliteus tendon, the surgeon must be aware of its anatomic relationship to the origin of the lateral collateral ligament (LCL). What is the classic anatomic position of the popliteus insertion relative to the LCL femoral attachment?
Explanation
Question 38
A 32-year-old male sustains a distal-third oblique humerus fracture (Holstein-Lewis type). A posterior approach to the humerus is chosen for open reduction and internal fixation. To safely mobilize the radial nerve, the surgeon tracks it from the posterior compartment to the anterior compartment. At what approximate distance proximal to the lateral epicondyle does the radial nerve pierce the lateral intermuscular septum?
Explanation
Question 39
A 40-year-old male undergoes open reduction and internal fixation for a displaced anterior column acetabular fracture via the ilioinguinal approach. During dissection posterior to the superior pubic ramus, heavy arterial bleeding is encountered. This bleeding is most likely originating from an aberrant vascular connection between the external iliac system and which of the following arteries?
Explanation
Question 40
A 28-year-old avid cyclist presents with significant weakness of the interosseous muscles and adductor pollicis, but normal sensation over both the volar and dorsal aspects of the little finger. Compression of the ulnar nerve is suspected. At which of the following anatomic locations is the compression most likely occurring?
Explanation
Question 41
A 45-year-old female marathon runner with recalcitrant heel pain that is worst with the first steps in the morning has failed 9 months of conservative management. Tenderness is distinctly maximal at the medial aspect of the calcaneal tuberosity, and she describes radiating burning pain. A release of the first branch of the lateral plantar nerve (Baxter's nerve) is planned. Between which two muscular structures does this nerve typically become entrapped?
Explanation
Question 42
A 24-year-old competitive weightlifter presents with vague posterior shoulder pain and weakness in external rotation. MRI reveals isolated denervation edema and early atrophy of the teres minor. Examination demonstrates diminished pinprick sensation over the lateral deltoid. Entrapment of the affected nerve is most likely occurring in an anatomic space bounded superiorly by which of the following structures?
Explanation
Question 43
A 30-year-old man sustains a severe hyperdorsiflexion injury of the ankle resulting in a displaced talar neck fracture (Hawkins Type III). Which of the following arterial vessels is the predominant blood supply to the body of the talus, placing it at the highest risk for avascular necrosis if disrupted?
Explanation
Question 44
A 35-year-old woman requires a dorsal approach to the wrist for a proximal row carpectomy. The surgeon meticulously releases the extensor retinaculum over the third dorsal compartment to protect its contents. Which structure is contained entirely within this compartment, and around what bony landmark does it pivot?
Explanation
Question 45
A senior resident is utilizing the anterolateral (Watson-Jones) approach to the hip for a total hip arthroplasty. The superficial surgical interval is developed between the tensor fasciae latae and the gluteus medius. What is the true internervous plane utilized in this superficial dissection?
Explanation
Question 46
A 35-year-old male undergoes a Latarjet procedure for recurrent anterior shoulder instability. Postoperatively, he has weakness in elbow flexion and decreased sensation over the lateral forearm. Which of the following anatomic structures was most likely injured during the conjoint tendon retraction?
Explanation
Question 47
A 28-year-old male sustains a displaced talar neck fracture with subluxation of the subtalar joint (Hawkins type II). Which of the following arteries provides the predominant blood supply to the talar body, and is at greatest risk of disruption in this injury pattern?
Explanation
Question 48
A 40-year-old female presents with a deep space infection of the hand after a puncture wound to the palmar aspect of her index finger. The infection has spread proximally from the flexor tendon sheath. Which of the following anatomical structures serves as the primary conduit for this spread into the deep palmar spaces?
Explanation
Question 49
During a posterolateral approach to the hip for a total hip arthroplasty, the surgeon splits the gluteus maximus in line with its fibers. To access the short external rotators, which of the following nerves must be identified and protected as it courses anterior to the piriformis in normal anatomy, but can pierce the piriformis muscle in up to 15% of patients?
Explanation
Question 50
A spine surgeon is placing L4 pedicle screws using a freehand technique. According to standard anatomical landmarks (the intersection technique), what is the optimal starting point for the L4 pedicle screw?
Explanation
Question 51
A 22-year-old football player sustains a direct blow to the anteromedial aspect of his knee, resulting in a posterolateral corner (PLC) injury. During surgical reconstruction of the PLC, the surgeon dissects near the fibular head. Where is the common peroneal nerve most vulnerable to iatrogenic injury in this region?
Explanation
Question 52
A 31-year-old male presents with a suspected Essex-Lopresti injury after a fall on an outstretched hand. He has pain at the elbow and wrist. Which portion of the interosseous membrane of the forearm is the primary stabilizer against longitudinal radioulnar translation?
Explanation
Question 53
A 50-year-old female presents with stage II adult-acquired flatfoot deformity secondary to posterior tibial tendon dysfunction. Which of the following ligamentous structures, critically important for supporting the talar head, is most commonly attenuated alongside the posterior tibial tendon in this condition?
Explanation
Question 54
During an ilioinguinal approach for an anterior column acetabular fracture, significant hemorrhage is encountered behind the superior pubic ramus, approximately 5-6 cm from the pubic symphysis. Which of the following anatomical variants is the most likely source of the bleeding?
Explanation
Question 55
A 45-year-old tennis player complains of vague posterior shoulder pain and weakness in external rotation. An MRI reveals a multilobulated paralabral cyst at the spinoglenoid notch. Which of the following muscles is most likely to exhibit isolated atrophy on physical examination or imaging?
Explanation
Question 56
A 32-year-old bodybuilder presents with poorly localized posterior shoulder pain and numbness over the lateral aspect of the deltoid. Examination reveals weakness in external rotation and abduction. An MRI shows an isolated paralabral cyst compressing a nerve within a space bordered superiorly by the teres minor, inferiorly by the teres major, medially by the long head of the triceps, and laterally by the surgical neck of the humerus. Which of the following vessels accompanies the affected nerve in this space?
Explanation
Question 57
A 24-year-old man sustains a fall onto an outstretched hand. Radiographs demonstrate a fracture through the proximal pole of the scaphoid. He is informed that this specific fracture pattern is at a high risk for avascular necrosis due to the unique retrograde blood supply of the scaphoid. The predominant blood supply to the scaphoid enters at which location and originates from which artery?
Explanation
Question 58
A 28-year-old soccer player undergoes surgical reconstruction of the posterior cruciate ligament (PCL) after a dashboard injury. The surgeon plans a double-bundle reconstruction to restore the native biomechanics of the PCL. During graft tensioning, at which degree of knee flexion should the anterolateral (AL) bundle and posteromedial (PM) bundle be tensioned, respectively?
Explanation
Question 59
A surgeon is performing a posterolateral approach (Kocher) to the radial head for a comminuted fracture in a 40-year-old woman. To minimize the risk of iatrogenic injury to the posterior interosseous nerve (PIN), the forearm should be held in which position, and the PIN is located within which muscle?
Explanation
Question 60
A 45-year-old male laborer presents with a sudden pop and pain in his anterior elbow after lifting a heavy box. An MRI confirms a complete tear of the distal biceps tendon. The surgeon plans an anatomic repair. To properly recreate the native biomechanics for maximal supination strength, where should the biceps tendon be repaired on the radial tuberosity?
Explanation
Question 61
A 65-year-old woman sustains a displaced subcapital femoral neck fracture. The decision is made to perform a hemiarthroplasty due to the high risk of avascular necrosis. The predominant blood supply to the adult femoral head, which is disrupted in this injury, arises from the medial femoral circumflex artery (MFCA). The main branch of the MFCA supplying the femoral head is located between which two muscles before piercing the joint capsule?
Explanation
Question 62
A 25-year-old athlete is undergoing anterior ankle arthroscopy for an osteochondral lesion of the talus. The anteromedial portal is established first, followed by the anterolateral portal. Which structure is at greatest risk of iatrogenic injury during the establishment of the anterolateral portal?
Explanation
Question 63
A 55-year-old man undergoes a lateral transpsoas approach to the lumbar spine for interbody fusion at L4-L5. Postoperatively, he complains of profound weakness in extending the knee and numbness over the anteromedial thigh and medial calf. The injured nerve is formed by the ventral rami of which nerve roots, and where does it typically emerge in relation to the psoas major muscle?
Explanation
Question 64
A 30-year-old rock climber presents with a 'bowstringing' deformity of his right ring finger following a sudden pop while gripping a small hold. Examination reveals pain and loss of mechanical advantage during finger flexion. Rupture of which two annular pulleys is most likely responsible for clinical bowstringing of the flexor tendons?
Explanation
Question 65
A 42-year-old woman is evaluated for a 'frozen shoulder' (adhesive capsulitis). Surgical capsular release is considered after 6 months of failed conservative management. The surgeon plans to release the rotator cuff interval. Which of the following structures is NOT a boundary or content of the rotator cuff interval?
Explanation
Question 66
A 28-year-old overhead athlete presents with posterior shoulder pain and weakness in external rotation and abduction. An MRI shows an isolated paralabral cyst compressing the nerve within the quadrangular space. Which of the following describes the boundaries of the space where the compression occurs?
Explanation
Question 67
Following a closed reduction and percutaneous pinning of a displaced extension-type supracondylar humerus fracture, a 7-year-old child demonstrates an inability to flex the interphalangeal joint of the thumb and the distal interphalangeal joint of the index finger. Which of the following muscles is also most likely to be weakened due to this specific nerve injury?
Explanation
Question 68
A 25-year-old football player sustains a direct blow to the anteromedial aspect of the knee while hyperextended. Examination reveals increased external tibial rotation at 30 degrees of knee flexion but symmetrical external rotation at 90 degrees compared to the contralateral knee. Which of the following structures is most likely injured?
Explanation
Question 69
A 32-year-old man sustains a displaced Hawkins type III talar neck fracture. Which of the following best describes the primary blood supply to the body of the talus, which is at the highest risk of disruption leading to avascular necrosis (AVN)?
Explanation
Question 70
A surgeon is performing a minimally invasive percutaneous repair of an acute Achilles tendon rupture. To minimize the risk of iatrogenic injury to the sural nerve, the surgeon must be aware of its anatomical course. At what approximate level does the sural nerve typically cross the lateral border of the Achilles tendon?
Explanation
Question 71
A 45-year-old woman is undergoing total hip arthroplasty via a posterior approach. The surgeon identifies the piriformis tendon and prepares to release it. According to the Beaton and Anson classification, what is the most common anatomical relationship between the sciatic nerve and the piriformis muscle?
Explanation
Question 72
A 24-year-old man presents with a closed distal third diaphyseal humerus fracture (Holstein-Lewis fracture) and an associated wrist drop on presentation. During surgical exploration via a posterior approach, the radial nerve is identified. In the posterior compartment of the arm, the radial nerve travels in the spiral groove between which two muscles?
Explanation
Question 73
The semimembranosus tendon has a complex insertion at the posteromedial corner of the knee, providing dynamic stabilization. Which of the following is NOT a recognized major insertion arm of the semimembranosus tendon?
Explanation
Question 74
A surgeon is applying a fine wire circular external fixator for a complex tibial plateau fracture. When placing transfixion wires in the proximal third of the tibia, which anatomic structures dictate the safe zone boundary posteromedially to avoid iatrogenic neurovascular injury?
Explanation
Question 75
De Quervain's tenosynovitis involves the first dorsal extensor compartment of the wrist. During surgical release, the surgeon must carefully decompress all subcompartments. Which of the following describes the most common anatomical arrangement of the tendons within the first dorsal compartment?
Explanation
Question 76
A 24-year-old professional volleyball player presents with isolated weakness in external rotation of the shoulder. Electromyography reveals isolated denervation of the infraspinatus muscle with normal supraspinatus function. Entrapment of the affected nerve is most likely occurring at the spinoglenoid notch. Which of the following structures forms the roof of this anatomical space?
Explanation
Question 77
During an ilioinguinal approach for open reduction and internal fixation of an anterior column acetabular fracture, the surgeon dissects along the posterior aspect of the superior pubic ramus. Sudden, brisk arterial hemorrhage occurs. This is most likely due to an injury to the 'corona mortis', which is an anastomotic vessel connecting the obturator system with which of the following?
Explanation
Question 78
A 30-year-old male undergoes surgical reconstruction of the posterolateral corner (PLC) of the knee following a multiligamentous knee injury. To achieve anatomic reconstruction, the surgeon must identify the exact femoral footprint of the popliteus tendon. Which of the following describes the correct location of the popliteus tendon insertion relative to the lateral collateral ligament (LCL) femoral attachment?
Explanation
Question 79
A pediatric patient sustains a widely displaced supracondylar humerus fracture. Post-operatively, the patient presents with an inability to flex the interphalangeal joint of the thumb and the distal interphalangeal joint of the index finger.
The nerve responsible for this specific motor deficit branches from a major nerve trunk that classically travels between the two heads of which of the following muscles?
Explanation
Question 80
A foot and ankle surgeon is performing a plantar approach for the excision of a deep midfoot mass. During dissection, the surgeon encounters an anatomical landmark where the flexor digitorum longus (FDL) tendon crosses dorsal to the flexor hallucis longus (FHL) tendon. This intersection is known as the Master Knot of Henry. Where is this structure precisely located?
Explanation
Question 81
A 45-year-old avid cyclist reports progressive numbness in the volar aspect of the small finger and ulnar half of the ring finger, along with weakness in finger abduction. Suspecting compression of the ulnar nerve at the wrist, the surgeon plans a release of Guyon's canal. Which of the following structures forms the true floor of Guyon's canal?
Explanation
Question 82
A surgeon is utilizing a standard deltopectoral approach for open reduction and internal fixation of a 3-part proximal humerus fracture. If extending the incision laterally into the deltoid muscle is required, the surgeon must be highly cautious of the axillary nerve. The main trunk of the axillary nerve typically courses along the deep surface of the deltoid at approximately what distance distal to the lateral edge of the acromion?
Explanation
Question 83
A 12-year-old overweight boy is diagnosed with a severe slipped capital femoral epiphysis (SCFE). The treating orthopedic surgeon counsels the parents on the risk of avascular necrosis. The primary blood supply to the capital femoral epiphysis in this age group is derived from the lateral epiphyseal vessels. These vessels are terminal branches of which of the following arteries?
Explanation
Question 84
During a total hip arthroplasty via the anterior (Smith-Petersen) approach, the surgeon exploits an internervous plane to access the hip joint while minimizing denervation. Which two nerves supply the muscles that define the superficial surgical interval of this approach?
Explanation
Question 85
A spine surgeon is performing an anterior cervical discectomy and fusion (ACDF) for C5-C6 myelopathy.
When aggressively decompressing the lateral aspect of the uncovertebral joint, there is a distinct risk of iatrogenic injury to the vertebral artery. Ascending from the subclavian artery, the vertebral artery classically first enters the transverse foramen at which cervical level in the vast majority of patients?

Explanation
Question 86
A 32-year-old competitive cyclist presents with intrinsic muscle weakness in his right hand. He has noticeable clawing of the ring and small fingers but maintains intact sensation over the hypothenar eminence and the palmar aspect of the ulnar digits. At which anatomical zone of Guyon's canal is the ulnar nerve most likely compressed?
Explanation
Question 87
During an ilioinguinal approach for the internal fixation of an anterior column acetabular fracture, significant hemorrhage is encountered while dissecting over the posterior aspect of the superior pubic ramus. Which of the following is the most likely source of this bleeding?
Explanation
Question 88
When performing the volar (Henry) approach to the proximal radius for fracture fixation, the deep dissection requires careful positioning of the forearm to protect a major nerve. The forearm should be placed in full supination to protect which of the following structures?
Explanation
Question 89
A 45-year-old man presents with severe lower back pain radiating down the right leg. Physical examination reveals weakness in right great toe extension (extensor hallucis longus) and diminished sensation over the dorsal first web space. Deep tendon reflexes are symmetrical and intact. An MRI reveals a far-lateral (extraforaminal) disc herniation at the L5-S1 level. Which nerve root is most likely compressed?
Explanation
Question 90
A 68-year-old woman sustains a displaced femoral neck fracture. Which of the following vessels is the primary contributor to the blood supply of the femoral head in an adult and is most at risk of disruption in this injury?
Explanation
Question 91
During a deltopectoral approach for a total shoulder arthroplasty, the cephalic vein is identified. Which of the following correctly describes its anatomical relationship and the recommended method of retraction during this approach?
Explanation
Question 92
Anatomic reconstruction of the posterolateral corner (PLC) of the knee requires precise placement of tunnels. What is the correct anatomical attachment of the fibular collateral ligament (LCL) on the lateral femoral condyle?
Explanation
Question 93
A 28-year-old male is involved in a high-speed motor vehicle collision and sustains a displaced Hawkins Type III fracture of the talar neck. Which of the following arteries provides the dominant blood supply to the talar body and is most compromised in this injury?
Explanation
Question 94
The Triangular Fibrocartilage Complex (TFCC) is the major stabilizer of the distal radioulnar joint (DRUJ). Which specific component of the TFCC provides the primary restraint to dorsal translation of the distal radius relative to the ulna during active forearm pronation?
Explanation
Question 95
A 22-year-old football player sustains a hyperplantarflexion injury to his midfoot. Radiographs show a widening of the space between the first and second metatarsals. An MRI confirms a complete rupture of the Lisfranc ligament. Between which two specific osseous structures does the Lisfranc ligament course?
Explanation
Question 96
A 45-year-old female undergoes a posterior cervical lymph node biopsy. Several weeks postoperatively, she presents with persistent shoulder aching, weakness with overhead activities, and prominent lateral winging of her scapula on physical examination. Damage to which of the following anatomical structures is most likely responsible for these findings?
Explanation
Question 97
During an ilioinguinal approach for an anterior column acetabular fracture, the surgeon encounters massive, pulsatile hemorrhage while exposing the superior pubic ramus. This bleeding most likely originates from an anomalous vascular connection (corona mortis) bridging which two vascular systems?
Explanation
Question 98
A patient presents with recalcitrant tarsal tunnel syndrome. Surgical release of the flexor retinaculum is planned. From anteromedial to posterolateral, what is the anatomical arrangement of the contents within the tarsal tunnel posterior to the medial malleolus?
Explanation
Question 99
In performing an inside-out repair of the posterior horn of the medial meniscus, a postero-medial approach is often utilized to retrieve needles safely. To prevent iatrogenic nerve injury, the surgeon must be aware of the anatomic course of the saphenous nerve. At the level of the medial joint line, the main trunk of the saphenous nerve is typically located between which two tendons?
Explanation
Question 100
A 28-year-old carpenter sustains a volar laceration over his dominant index finger, resulting in complete transection of the flexor digitorum profundus (FDP) and flexor digitorum superficialis (FDS) tendons in Zone II. While retrieving the retracted FDP tendon, the surgeon visualizes the attached lumbrical muscle. Which of the following statements accurately describes the typical anatomy of the first lumbrical?
Explanation
None
