AAOS Orthopedic Basic Science MCQs (Set 2): Musculoskeletal Anatomy, Biomechanics & Physiology | Board Review
Key Takeaway
This high-yield question set for the AAOS/ABOS Basic Science exams focuses on core foundational knowledge. Questions cover musculoskeletal anatomy, including nerve and muscle groups, principles of orthopedic biomechanics, and crucial aspects of bone and cartilage physiology, aiding in comprehensive board preparation.
AAOS Orthopedic Basic Science MCQs (Set 2): Musculoskeletal Anatomy, Biomechanics & Physiology | Board Review
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 58-year-old woman has a fracture through a metacarpal lesion after a motor vehicle accident. She denies any preinjury symptoms and the fracture heals uneventfully. Based on the radiograph and MRI scans shown in Figures 22a through 22c obtained following fracture healing, follow-up management should consist of

Explanation
Question 2
A 14-year-old girl reports bilateral patellofemoral symptoms. Based on the radiograph and MRI scans shown in Figures 23a through 23d, what is the next most appropriate step in management of the lesion?
Explanation
Question 3
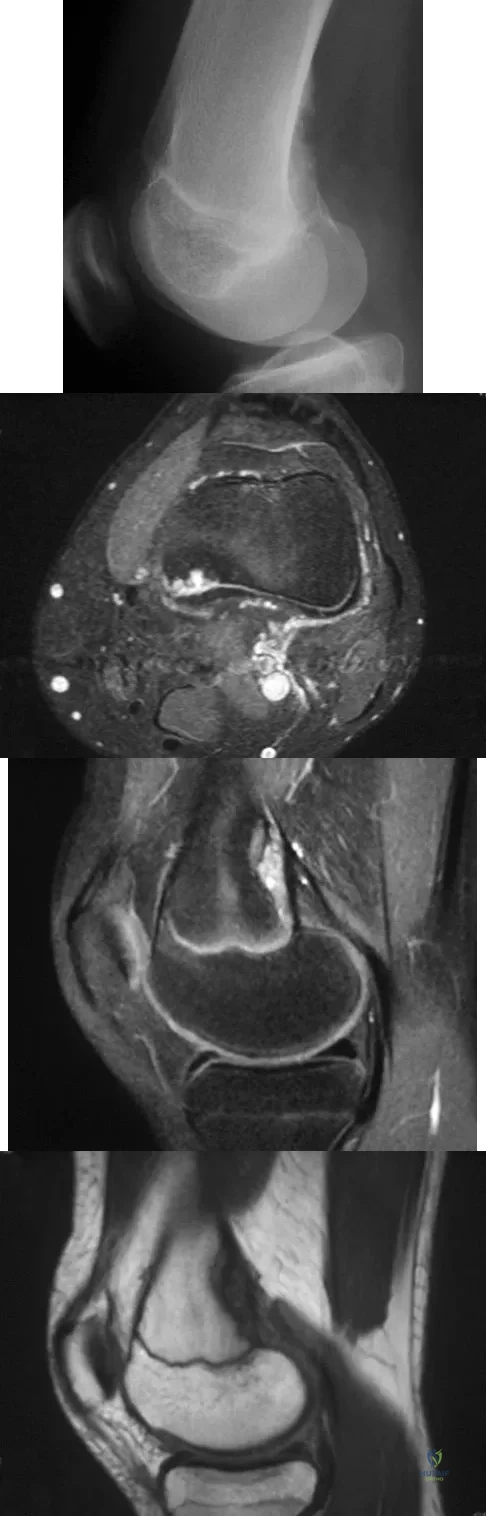
A 13-year-old boy has knee pain after sustaining a mild twisting injury while playing basketball 4 weeks ago. Radiographs and MRI scans are shown in Figures 24a through 24d, and biopsy specimens are shown in Figures 24e and 24f. Treatment should consist of
Explanation
Question 4
A 64-year-old man has had increasing pain in the left hip for the past 6 months. A radiograph and MRI scan are shown in Figures 25a and 25b. Biopsy specimens are shown in Figures 25c and 25d. What is the recommended treatment?
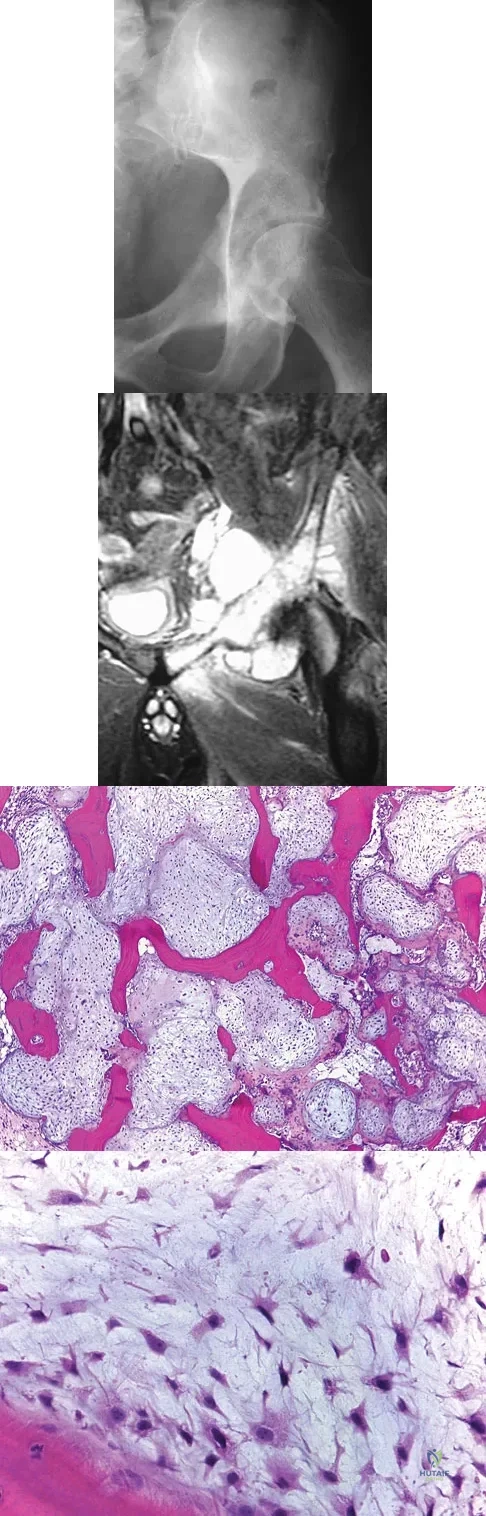
Explanation
Question 5
The scoring system for impending pathologic fractures devised by Mirels involves assessment of which of the following factors?

Explanation
Question 6
Figures 26a and 26b show the radiograph and MRI scan of a 22-year-old man with knee pain. What is the most likely diagnosis?

Explanation
Question 7
Which of the following malignant tumors most commonly contains soft-tissue calcifications seen on radiographs or CT?

Explanation
Question 8
Which of the following is most associated with local recurrence of the lesion seen in the radiograph and MRI scan shown in Figures 27a and 27b?

Explanation
Question 9
A 33-year-old woman reports a mass on the right hand that has been enlarging for 1 year. An intraoperative photograph is shown in Figure 28a, and a biopsy specimen is shown in Figure 28b. What is the most likely diagnosis?

Explanation
Question 10
A 15-year-old girl has had a painful mass on the medial aspect of her left thigh for the past 5 years. The pain is present only when she is performing athletic activities and is completely relieved with rest. A radiograph and MRI scan are shown in Figures 29a and 29b. The patient and her parents would like to have the mass removed. What further diagnostic studies are required prior to considering surgical resection?

Explanation
Question 11
A 22-year-old man has mild hip pain bilaterally and multiple skeletal lesions. Based on the pelvic radiograph shown in Figure 30, what is the inheritance pattern for his disorder?

Explanation
Question 12
An 80-year-old woman notes a painless mass posterior to her left knee. MRI scans are shown in Figures 31a and 31b. What is the best course of action?
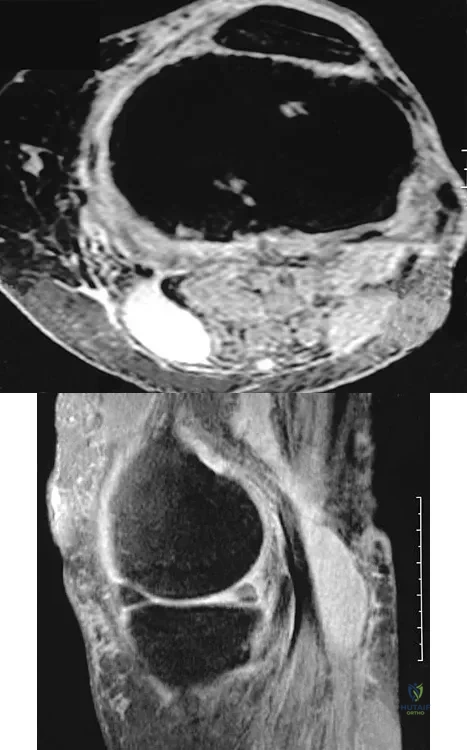
Explanation
Question 13
A 38-year-old man has an enlarging left paraspinal soft-tissue mass. Based on the MRI scans and biopsy specimens shown in Figures 32a through 32e, what is the most likely diagnosis?
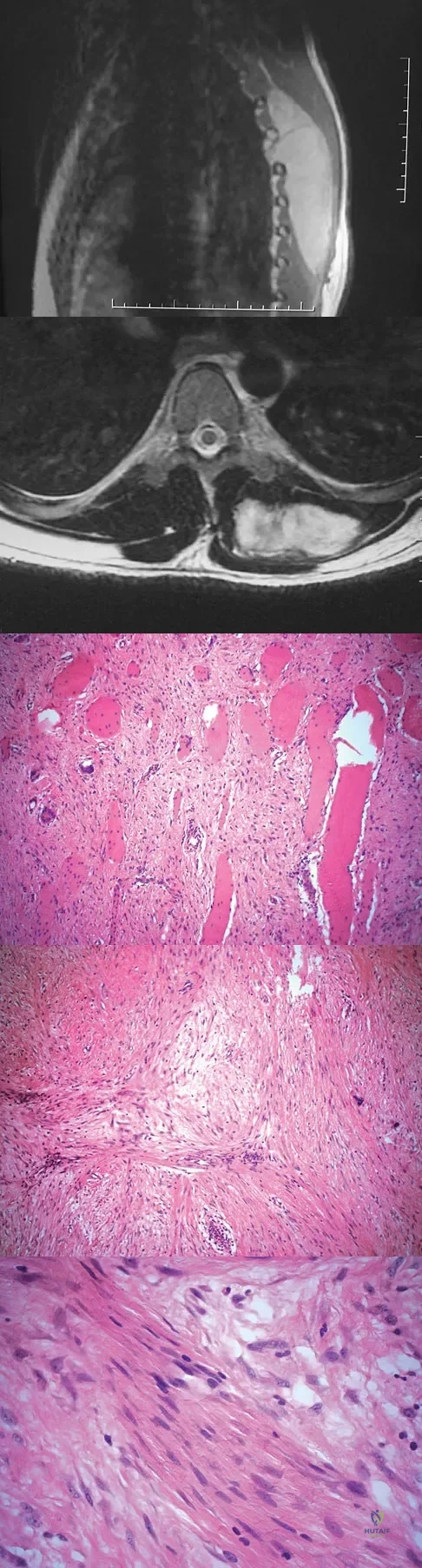
Explanation
Question 14
What is the most common malignancy involving the hand?

Explanation
Question 15
A 38-year-old man who is an avid runner reports a several month history of right hip pain. Based on the radiograph and cross-sectional CT scan shown in Figures 33a and 33b, what is the most likely diagnosis for the lesions seen on the femoral neck?

Explanation
Question 16
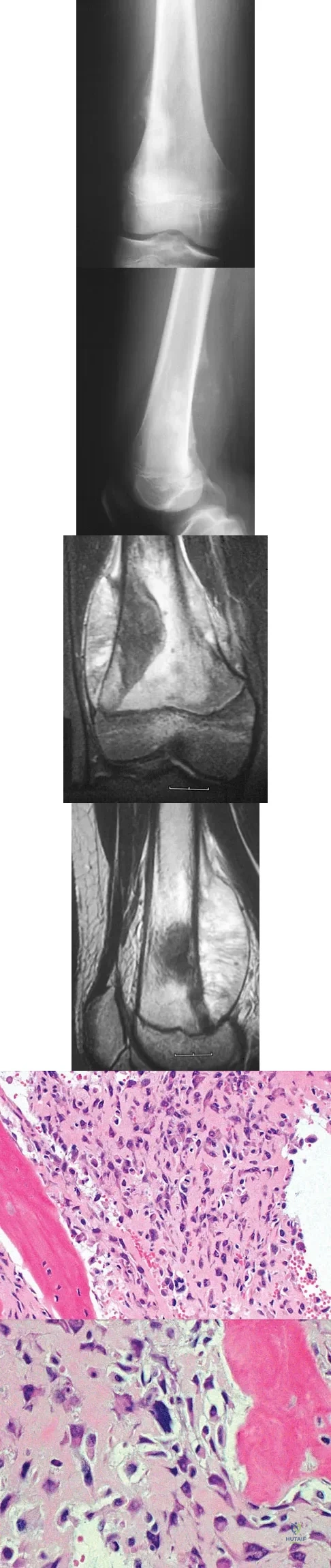
A 35-year-old man has had progressive right knee pain for the past 2 months. An AP radiograph, bone scan, MRI scan, and photomicrograph are shown in Figures 34a through 34d. What is the most appropriate treatment of this lesion?
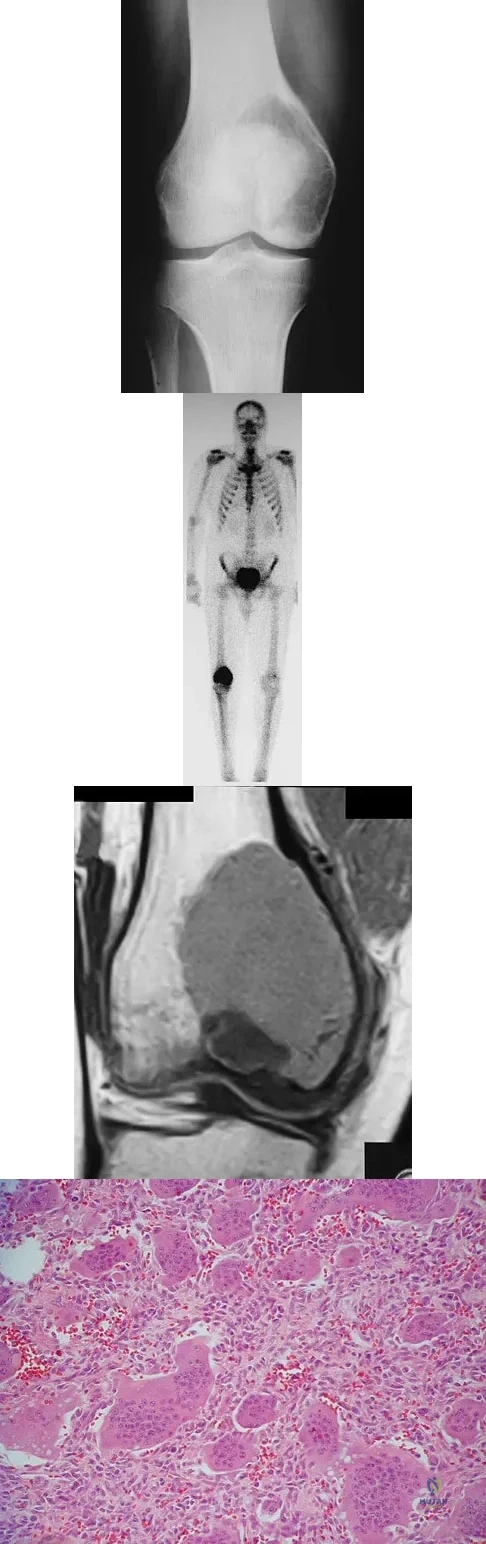
Explanation
Question 17
What is the most common bone tumor in the hand?

Explanation
Question 18
A 30-year-old woman has had pain in her right leg for the past 6 months. A lytic lesion is noted in the anterior cortex of the midtibia, extending 5 cm in length without a soft-tissue mass. A radiograph and a biopsy specimen are shown in Figures 35a and 35b. What is the preferred treatment?
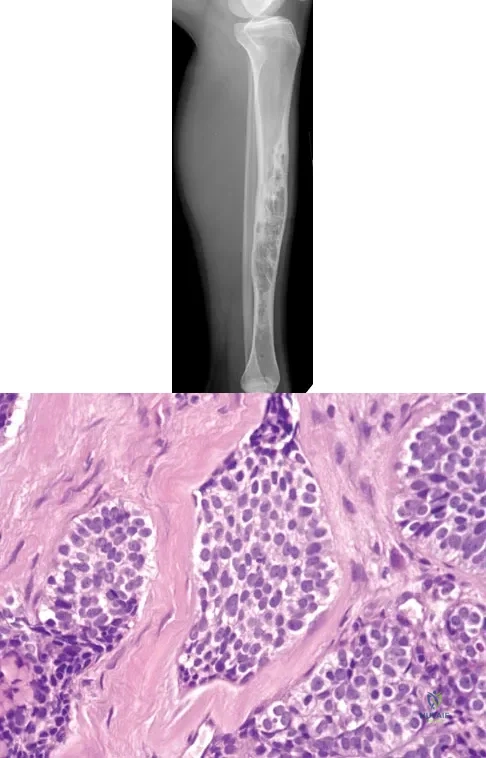
Explanation
Question 19
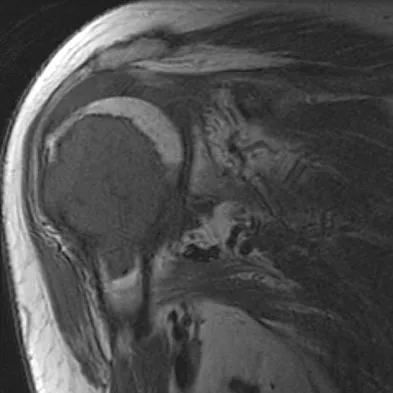
A 75-year-old woman has had severe shoulder pain for the past month. Her medical history includes hypertension and a total nephrectomy for renal cell carcinoma 7 years ago. Radiographs and sagittal MRI scans are shown in Figures 36a through 36d. A bone scan reveals this to be an isolated lesion. Biopsy findings are consistent with metastatic renal cell carcinoma. What is the most appropriate treatment for this patient?
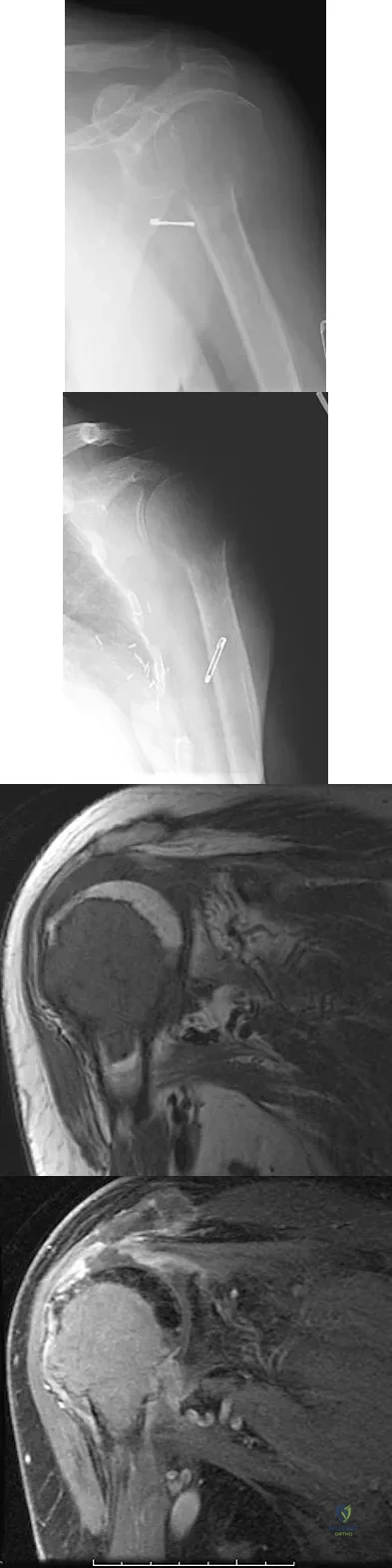
Explanation
Question 20
A patient undergoes a simple excision of a 3-cm superficial mass in the thigh at another institution. The final pathology reveals a leiomyosarcoma, without reference to the margins. What is the recommendation for definitive treatment?

Explanation
Question 21
A 14-year-old girl has had progressive heel pain for the past several months. Based on the radiograph, MRI scan, and biopsy specimens shown in Figures 37a through 37d, treatment should include
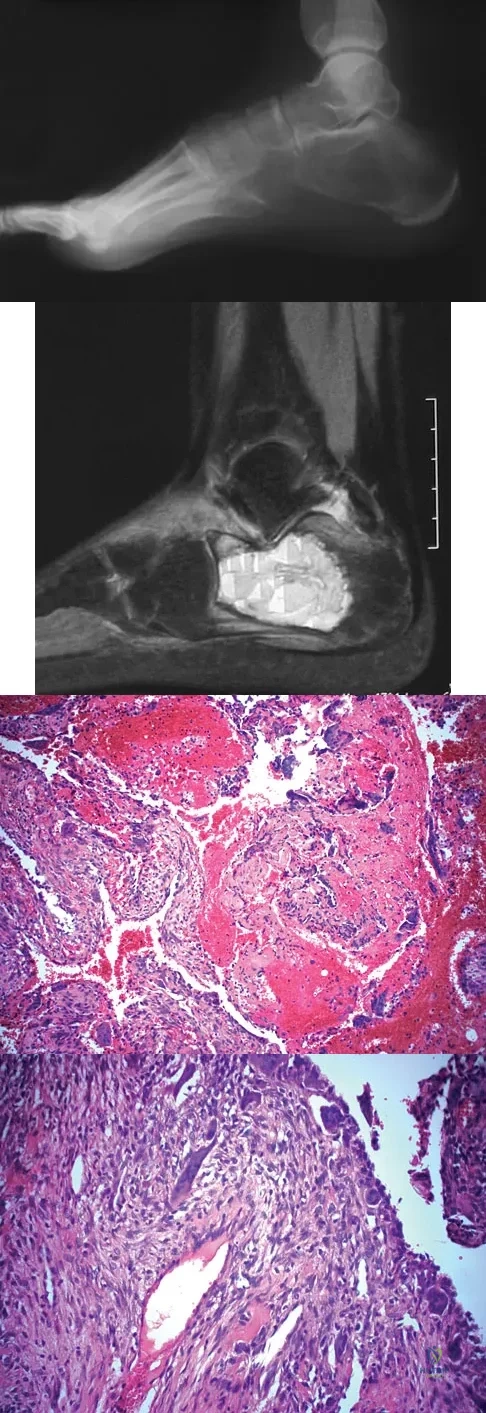
Explanation
Question 22
A 14-year-old boy has had knee pain for the past 2 months. He also has a low-grade fever of 101.3 degrees F (38.5 degrees C). Laboratory studies show a WBC count of 12,100/mm3 and an erythrocyte sedimentation rate of 58/h. A biopsy specimen of a lesion in the distal femoral metaphysis is shown in Figure 38. What is the most appropriate treatment?

Explanation
Question 23
A 14-year-old girl reports a 3-week history of anterior thigh pain and a palpable mass after sustaining a soccer-related injury. Examination reveals a tender, firm mass in the midportion of the rectus femoris. MRI scans are shown in Figures 39a through 39c. What is the most appropriate management?

Explanation
Question 24
A 40-year-old man reports an enlarging soft-tissue mass in his right shoulder. Based on the MRI scan and biopsy specimens shown in Figures 40a through 40c, what is the most likely diagnosis?
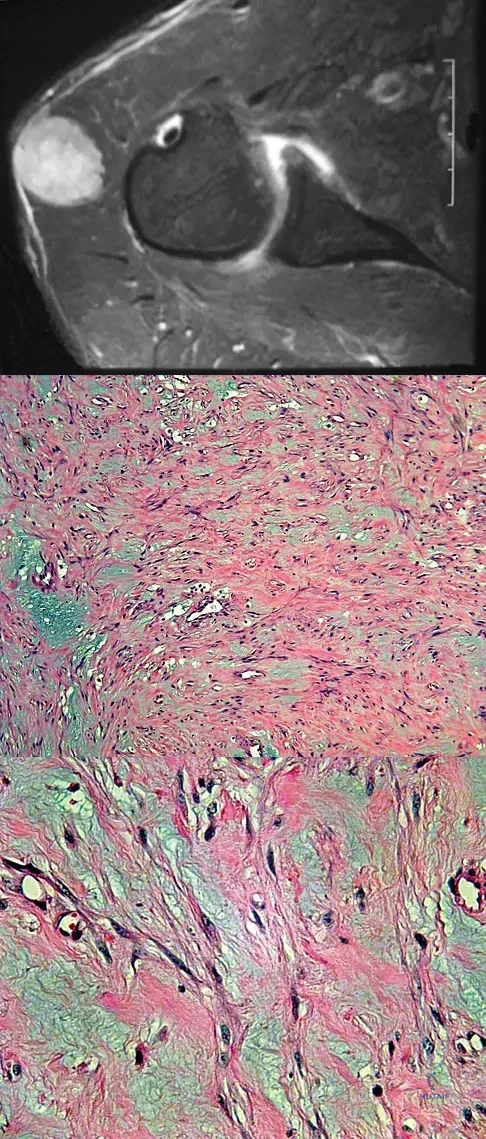
Explanation
Question 25
A 28-year-old woman has had pain in her hand and mild swelling of the little finger for the past 2 months. A radiograph is shown in Figure 41a, and the biopsy specimen is shown in Figures 41b and 41c. What is the most likely diagnosis?
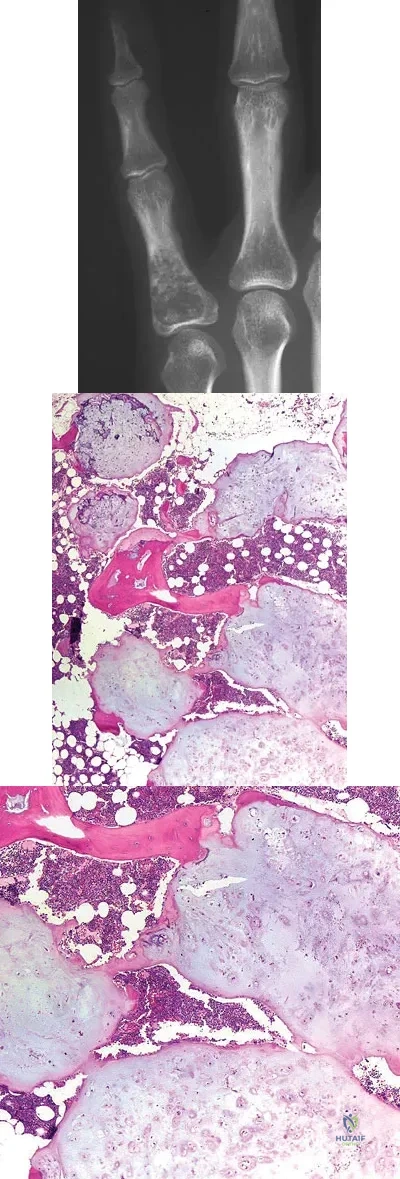
Explanation
Question 26
According to Perren's strain theory, what level of tissue strain optimally promotes the formation of woven bone during secondary fracture healing?
Explanation
Question 27
In articular cartilage, which zone is characterized by the highest concentration of water and collagen fibers oriented parallel to the joint surface?
Explanation
Question 28
During skeletal muscle contraction, maximum isometric tension is generated at optimal resting length. This length corresponds physiologically to which of the following states?
Explanation
Question 29
On a load-elongation (stress-strain) curve of a normal ligament, what structural change is responsible for the initial "toe region"?
Explanation
Question 30
Which particle size of polyethylene wear debris is most highly associated with macrophage activation and subsequent periprosthetic osteolysis?
Explanation
Question 31
Combining a 316L stainless steel plate with a titanium alloy screw in a fracture construct is most likely to result in which type of corrosion?
Explanation
Question 32
A patient sustains a closed midshaft humerus fracture and presents with a radial nerve palsy. An EMG at 4 weeks shows fibrillation potentials in the brachioradialis, but an MRI demonstrates an intact epineurium. Which Seddon classification describes this injury?
Explanation
Question 33
Which of the following bone graft substitutes is considered exclusively osteoconductive and lacks both osteoinductive and osteogenic properties?
Explanation
Question 34
Rigid plate fixation of a transverse diaphyseal fracture leading to absolute stability primarily heals via which biological process?
Explanation
Question 35
During the early stages of osteoarthritis, which of the following enzymes is primarily responsible for the aggressive cleavage of Type II collagen in the extracellular matrix?
Explanation
Question 36
The pullout strength of a cortical screw is most directly proportional to which of the following geometric parameters?
Explanation
Question 37
In myelinated peripheral nerves, saltatory conduction occurs rapidly due to the high concentration of which specific ion channels at the Nodes of Ranvier?
Explanation
Question 38
When analyzing an orthopedic implant's S-N (Stress-Number of cycles) curve, the "endurance limit" refers to the:
Explanation
Question 39
Parathyroid hormone (PTH) stimulates bone resorption primarily by binding to receptors on which of the following cell types?
Explanation
Question 40
The outer annulus fibrosus of the intervertebral disc is specialized to resist tensile hoop stresses. Which type of collagen predominantly provides this mechanical property?
Explanation
Question 41
During the remodeling phase of ligament healing, which biochemical transition characterizes the maturation of the scar tissue?
Explanation
Question 42
In the metabolic pathway of Vitamin D, the final hydroxylation step to produce the active form, 1,25-dihydroxyvitamin D3, occurs primarily in the:
Explanation
Question 43
During a normal human gait cycle, maximum muscle activity of the tibialis anterior occurs at which specific phase to prevent foot drop?
Explanation
Question 44
Which of the following characteristics is true regarding Type I (slow-twitch) skeletal muscle fibers compared to Type IIb fibers?
Explanation
Question 45
Which mechanism of joint lubrication is most critical for reducing friction between articular cartilage surfaces during high-load, low-speed activities, such as initiating standing from a chair?
Explanation
Question 46
In normal articular cartilage, which of the following best describes the structural composition and mechanical function of the superficial zone?
Explanation
Question 47
Which of the following biomechanical conditions is required for primary (strain-free) bone healing to occur, and what is the predominant mechanism of osteogenesis?
Explanation
Question 48
Which type of muscle contraction generates the highest maximum force, and what is its associated physiological energy characteristic?
Explanation
Question 49
A continuous, constant compressive load is applied to an intervertebral disc over several hours, resulting in progressive deformation over time. This specific viscoelastic property is defined as:
Explanation
Question 50
During the normal human gait cycle, which muscle group demonstrates peak activity during the initial contact (heel strike) to loading response phase to safely lower the foot?
Explanation
Question 51
Following a severe traction injury to the brachial plexus resulting in axonotmesis, Wallerian degeneration begins. Which of the following best describes this physiological process?
Explanation
Question 52
On the stress-strain curve of a normal tendon, the initial "toe region" represents which of the following structural events?
Explanation
Question 53
Under high-load, low-velocity conditions (such as standing from a seated position), which type of lubrication mechanism predominantly protects the articular cartilage surfaces?
Explanation
Question 54
Denosumab, a biological therapy used in the treatment of osteoporosis, exerts its effect by directly targeting which of the following molecular mechanisms?
Explanation
Question 55
In total hip arthroplasty, the incorporation of highly cross-linked polyethylene primarily improves wear resistance by mitigating which specific mechanism of wear?
Explanation
Question 56
Which of the following screw design alterations will most significantly increase the pullout strength of a cortical bone screw in diaphyseal bone?
Explanation
Question 57
The blood supply to the adult medial meniscus is primarily derived from the medial inferior genicular artery. Approximately what portion of the meniscus receives a direct vascular supply?
Explanation
Question 58
Demineralized bone matrix (DBM) is commonly used as a biological adjunct in spinal fusion. Which of the following best characterizes its bone healing properties?
Explanation
Question 59
Parathyroid hormone (PTH) regulates serum calcium levels through multiple systemic mechanisms. What is its direct physiological effect on the kidney?
Explanation
Question 60
When using a bridge plating technique for a comminuted diaphyseal fracture, increasing the "working length" of the plate has which of the following biomechanical effects?
Explanation
Question 61
Galvanic corrosion occurs when two dissimilar metals are placed in physical contact within a conductive fluid environment. Which of the following metal combinations is most likely to result in significant galvanic corrosion in orthopedic implants?
Explanation
Question 62
The anterior cruciate ligament (ACL) is composed of two main functional bundles. During deep knee flexion, which bundle is under the most tension, and what is its primary biomechanical role?
Explanation
Question 63
During the physiological flexion and extension of a normal healthy lower cervical spine segment, the instantaneous axis of rotation (IAR) is typically located in which anatomical structure?
Explanation
Question 64
Cigarette smoking strongly inhibits bone healing and significantly increases the rate of nonunion. Which of the following is the primary physiological mechanism driving this adverse effect?
Explanation
Question 65
Muscle strain injuries most commonly occur at the myotendinous junction. Biomechanically, what microscopic structural feature of this junction makes it uniquely susceptible to these injuries?
Explanation
Question 66
The deep zone of articular cartilage is best characterized by which of the following combinations of properties?
Explanation
Question 67
Which cytokine serves as the primary decoy receptor for RANKL, thereby inhibiting osteoclastogenesis and reducing bone resorption?
Explanation
Question 68
When a constant load is applied to a viscoelastic ligament over an extended period of time, the tissue gradually elongates. This biomechanical phenomenon is known as:
Explanation
Question 69
Which of the following geometric alterations to a cortical screw design will most significantly increase its pullout strength?
Explanation
Question 70
Type I (slow-twitch) skeletal muscle fibers are primarily characterized by which type of metabolism and fatigue resistance?
Explanation
Question 71
In the mechanism of periprosthetic osteolysis following total hip arthroplasty, ultra-high-molecular-weight polyethylene (UHMWPE) wear particles are primarily phagocytosed by which cell type?
Explanation
Question 72
According to Sunderland's classification of peripheral nerve injuries, a fourth-degree injury involves disruption of all the following structures EXCEPT the:
Explanation
Question 73
During secondary fracture healing, peak expression of Type II collagen occurs during which of the following stages?
Explanation
Question 74
In the biomechanics of bridge plating for a comminuted diaphyseal fracture, the "working length" of the construct is defined as the distance between:
Explanation
Question 75
Which of the following combinations of implant alloys placed in direct physical contact poses the highest risk of significant galvanic corrosion?
Explanation
Question 76
Which mechanism of joint lubrication is most critical for protecting articular surfaces under high-load, low-speed conditions, such as initial standing from a seated position?
Explanation
Question 77
A massive structural cortical allograft is utilized to reconstruct a large segmental bone defect. The graft is incorporated into the host primarily via which biologic process?
Explanation
Question 78
Regarding the gross anatomy and biomechanics of the knee menisci, the medial meniscus differs from the lateral meniscus in that the medial meniscus is:
Explanation
Question 79
Microscopically, which of the following is a primary structural difference between ligaments and tendons?
Explanation
Question 80
During the propagation of a typical neuronal action potential, the rapid depolarization phase is directly mediated by the influx of which of the following ions?
Explanation
Question 81
According to Wolff's Law, bone adapts its architecture in response to mechanical stress. The primary mechanosensory cell responsible for detecting fluid shear stress in the bone matrix is the:
Explanation
Question 82
During the normal process of tendon healing, the transition from disorganized Type III collagen synthesis to more aligned Type I collagen synthesis begins prominently during which phase?
Explanation
Question 83
The unique ability of articular cartilage to withstand massive compressive loads is primarily determined by the biomechanical interaction between:
Explanation
Question 84
Which of the following sterilization techniques for ultra-high-molecular-weight polyethylene (UHMWPE) joint components is most strongly associated with generating free radicals, leading to accelerated oxidative degradation?
Explanation
Question 85
A 12-year-old boy presents with a history of recurrent long bone fractures after minimal trauma, progressive hearing loss, and distinctly blue sclerae. This clinical phenotype is most likely due to a genetic mutation affecting which structural protein?
Explanation
Question 86
Which of the following combinations of orthopaedic implant materials is most susceptible to severe galvanic corrosion when placed in direct physical contact in vivo?
Explanation
Question 87
During the application of a dynamic splint to a contracted joint, a constant deformation is maintained over time. The observed decrease in peak force required to maintain this constant tissue length is an example of which viscoelastic property?
Explanation
Question 88
In which zone of normal articular cartilage are the type II collagen fibers oriented primarily perpendicular to the joint surface to maximize resistance to compressive loads?
Explanation
Question 89
Which of the following molecules acts as a soluble decoy receptor for RANKL, thereby inhibiting osteoclastogenesis and reducing bone resorption?
Explanation
Question 90
A physical therapy protocol specifies a muscle contraction where tension remains constant while the muscle actively lengthens to control a decelerating load. Which of the following best describes this type of muscle contraction?
Explanation
Question 91
Which of the following geometric structural properties most directly dictates a long bone's resistance to bending forces?
Explanation
Question 92
Absolute stability in fracture fixation with a fracture gap of less than 0.1 mm results in primary bone healing. Which of the following represents the predominant mechanism of healing under these strict biomechanical conditions?
Explanation
Question 93
During the normal gait cycle, maximum physiological dorsiflexion of the ankle occurs at which of the following phases?
Explanation
Question 94
What is the primary biomechanical function of the aggrecan molecule within the extracellular matrix of articular cartilage?
Explanation
Question 95
Following a complete rupture of the anterior cruciate ligament (ACL), the initial phase of biological healing features a hematoma. Which type of collagen is predominantly synthesized by fibroblasts during the early proliferative phase of ligament healing?
Explanation
Question 96
Fibroblast growth factor 23 (FGF23) is a critical endocrine regulator of phosphate homeostasis. Which of the following accurately describes the primary physiological mechanism of FGF23?
Explanation
Question 97
According to the Sunderland classification of peripheral nerve injuries, a third-degree injury is defined by the disruption of the axon and which of the following connective tissue structures?
Explanation
Question 98
Which of the following transcription factors serves as the essential master regulator required for the differentiation of mesenchymal stem cells into the osteoblast lineage?
Explanation
Question 99
Which specific mode of wear is characterized by the generation of particulate debris when micro-asperities between two articulating bearing surfaces bond together and are subsequently torn away from the softer material?
Explanation
Question 100
Which physiological mechanism of joint lubrication is most actively relied upon by the native knee under conditions of high compressive loading and extremely low velocity?
Explanation
None
