Anatomy Board Review MCQs (Set 4): Peripheral Nerves, Major Joints, & Muscle Anatomy | USMLE & ABOS Prep
Key Takeaway
This high-yield question set (Set 4) for anatomy board review focuses on essential peripheral neuroanatomy, covering nerve plexuses and their distributions. It also includes challenging questions on major joint structures and the functional anatomy of the musculoskeletal system, critical for medical board preparation.
Anatomy Board Review MCQs (Set 4): Peripheral Nerves, Major Joints, & Muscle Anatomy | USMLE & ABOS Prep
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Bleeding is encountered while developing the internervous plane between the tensor fascia lata and the sartorius during the anterior approach to the hip. The most likely cause is injury to what artery?
Explanation
Question 2
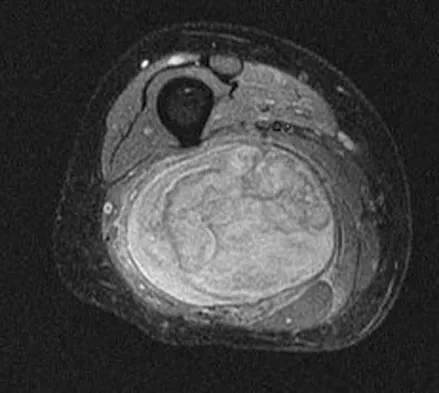
A 36-year-old woman with familial neurofibromatosis has an enlarging mass in the posterior thigh. The lesion has slowly increased in size and is now constantly painful. Pressure on the mass causes dysesthesias in the foot. Figures 44a through 44c show T1-weighted, STIR, and T1-weighted fat-saturated gadolinium scans, respectively. Figure 44d shows a PET scan. What does this lesion most likely represent?
Explanation
Question 3
In Dupuytren's disease, the retrovascular cord typically displaces the radial proper digital nerve of the ring finger in what direction?
Explanation
Question 4
Ganglion cysts about the wrist most commonly arise from what structure?
Explanation
Question 5
A 60-year-old woman has activity-related hip pain after undergoing arthroplasty 5 years ago. She has severe Parkinsonism and denies fevers or chills. Radiographs are shown in Figures 45a and 45b. What is the most likely cause of her pain?
Explanation
Question 6
A 15-year-old boy reports leg pain after being tackled during football practice. Radiographs and a CT scan are shown in Figures 46a through 46c. The patient has a pathologic fracture through what underlying lesion?
Explanation
Question 7
A 28-year-old man has left knee pain after a snow skiing accident. The MRI scan shown in Figure 47 reveals which of the following?
Explanation
Question 8
Following application of a short leg cast, a patient reports a complete foot drop. A compression injury of the peroneal nerve at the fibular neck is confirmed by electrical studies. Which of the following muscles is expected to be the last to recover function during the ensuing months?
Explanation
Question 9
A 28-year-old man reports knee stiffness, swelling, and a constant ache that is worse with activity. Examination reveals an effusion, global tenderness, and warmth to the touch. Flexion is limited to 110 degrees. Figures 48a through 48d show sagittal T1-weighted, sagittal T2-weighted, axial T1-weighted fat-saturated gadolinium, and axial gradient echo MRI scans. Based on these findings, what is the most likely diagnosis?
Explanation
Question 10
Figure 49 shows an acute axial MRI scan of a left knee. What is the most likely diagnosis?
Explanation
Question 11
Spontaneous entrapment of the posterior interosseous nerve most commonly occurs in which of the following locations?
Explanation
Question 12
A 72-year-old man has had persistent pain after undergoing a hemiarthroplasty 18 months ago. Radiographs are shown in Figures 50a and 50b. What is the most likely cause of his problem?
Explanation
Question 13
What fibers of the anterior cruciate ligament tighten with extension of the knee?
Explanation
Question 14
In an effort to reduce costs, a limited MRI sequence is planned to detect a possible occult hip fracture. What is the anticipated fracture signal?
Explanation
Question 15
When using the direct lateral (or Hardinge) approach for hip arthroplasty, three muscles are detached from the femur. In addition to the vastus lateralis, they include the
Explanation
Question 16
Figure 51 shows an arthroscopic view of the patellofemoral joint from an inferolateral portal. The arrow points to which of the following structures?
Explanation
Question 17
In a juvenile Tillaux ankle fracture, what ligament causes the displacement of the fracture fragment?
Explanation
Question 18
When harvesting an iliac crest bone graft from the posterior approach, what anatomic structure is at greatest risk for injury if a Cobb elevator is directed too caudal?
Explanation
Question 19
Figures 52a and 52b show the radiographs of a left proximal femoral lesion noted serendipitously following minor trauma to the left hip. The patient has no thigh pain and is fully active without limitation. What is the most likely diagnosis of this bony lesion?
Explanation
Question 20
Figure 53 shows the arteriogram of a 45-year-old man who has severe vasculitis. What do the findings show?
Explanation
Question 21
A patient with a left-sided C6-7 herniated nucleous pulposis would likely have which of the following constellation of findings?
Explanation
Question 22
Which of the following muscle tendons inserts just lateral to the long head of biceps tendon on the proximal humerus?
Explanation
Question 23
A 4-month-old infant is unable to flex her elbow as a result of an obstetrical brachial plexus palsy. This most likely illustrates a predominate injury to what structure?
Explanation
Question 24
Following a fall from a height of 5 feet, a patient reports pain along the lateral border of the foot. The CT scan shown in Figure 54 indicates what pathology?
Explanation
Question 25
The patient in Figure 55 is actively attempting to make a fist. This clinical scenario suggests which of the following anatomic lesions?
Explanation
Question 26
A patient presents with weakness in thumb and finger extension but normal wrist extension (with noticeable radial deviation) and no sensory deficits. Entrapment of the involved nerve most commonly occurs at which of the following structures?
Explanation
Question 27
During an open posterior approach to the shoulder, the internervous plane between the infraspinatus and teres minor is utilized. Which of the following nerve branches is most at risk if the dissection is carried too far medially?
Explanation
Question 28
An accessory head of the flexor pollicis longus (Ganzer's muscle) is implicated in the compression of a nerve that results in an inability to form a proper "OK" sign. Which of the following muscles is primarily innervated by the affected nerve?
Explanation
Question 29
A 45-year-old overhead athlete presents with deep posterior shoulder pain and weakness in external rotation. Abduction strength is symmetric. MRI reveals a paralabral cyst. The cyst is most likely located in which of the following anatomic locations?
Explanation
Question 30
During a minimally invasive anterolateral approach to the distal tibia, the surgeon identifies a nerve crossing the surgical field from posteromedial to anterolateral. This nerve typically pierces the deep crural fascia to become subcutaneous at what location?
Explanation
Question 31
A 24-year-old athlete sustains a posterolateral corner (PLC) knee injury. Surgical reconstruction involves repairing the structure that inserts onto the fibular head and is the primary restraint to varus opening at 30 degrees of knee flexion. What is this structure?
Explanation
Question 32
In the setting of a perilunate dislocation, a patient develops profound weakness of the interossei and the lumbricals to the ring and small fingers, alongside decreased sensation over the volar small finger. The affected nerve is most likely compressed in which anatomical zone of Guyon's canal?
Explanation
Question 33
During a direct anterior approach to the hip (Smith-Petersen), the surgeon develops an internervous plane between muscles innervated by which two nerves?
Explanation
Question 34
A 10-year-old boy sustains a supracondylar humerus fracture. After reduction, he is unable to flex the interphalangeal joint of his thumb and the distal interphalangeal joint of his index finger. If this specific nerve injury persists, which of the following muscles will also demonstrate denervation on electromyography?
Explanation
Question 35
A 28-year-old professional baseball pitcher complains of posterior shoulder pain and numbness over the lateral deltoid. MRI demonstrates isolated atrophy of the teres minor muscle. Which artery travels through the specific anatomic space implicated in this nerve entrapment syndrome?
Explanation
Question 36
During a submuscular ulnar nerve transposition, the surgeon must completely release the fascial roof of the cubital tunnel. After identifying the nerve, the surgeon notes the structures comprising the floor of the cubital tunnel. Which of the following forms the true floor of this anatomical space?
Explanation
Question 37
A surgeon is performing a posterolateral corner reconstruction of the knee and must drill tunnels for the anatomic femoral attachments of the fibular collateral ligament (FCL) and the popliteus tendon. What is the typical anatomic relationship of the popliteus femoral footprint relative to the FCL footprint?
Explanation
Question 38
A 65-year-old patient with a history of long-standing rheumatoid arthritis presents with a sudden inability to actively extend the interphalangeal joint of the thumb. The ruptured tendon implicated in this condition normally hooks around which bony prominence at the wrist?
Explanation
Question 39
While performing the anterior (Henry) approach to the middle third of the radius for an open reduction and internal fixation, the surgeon develops an internervous plane. Which two nerves supply the muscles that define the proximal portion of this surgical interval?
Explanation
Question 40
During a tarsal tunnel release for posterior tibial nerve entrapment, the surgeon meticulously dissects the structures passing posterior to the medial malleolus. What is the correct anatomic order of these structures from anterior to posterior?
Explanation
Question 41
A patient presents with a midshaft humerus fracture and an associated complete wrist drop. The injured nerve originally exits the axilla and enters the posterior compartment of the arm by traveling with the profunda brachii artery through which specific anatomic space?
Explanation
Question 42
During a posterior approach to the hip (Kocher-Langenbeck), the surgeon tags and releases the short external rotators. To preserve the primary blood supply to the adult femoral head, the surgeon must protect the ascending branch of the medial femoral circumflex artery. Where does this crucial vessel typically run?
Explanation
Question 43
A patient suffers a severe laceration to the volar wrist, resulting in a complete, high ulnar nerve transection. Which of the following best describes the origin and insertion of the functional lumbrical muscles that are spared in this injury?
Explanation
Question 44
A 25-year-old man presents with prominent medial scapular winging when asked to push against a wall, following a heavy traction injury to his shoulder. Electromyography confirms an isolated nerve palsy. From which specific nerve roots does the affected nerve originate?
Explanation
Question 45
A 28-year-old overhead athlete presents with isolated weakness in shoulder external rotation. Abduction is full and painless. Magnetic resonance imaging reveals a paralabral cyst. Compression of the nerve at which of the following locations is most likely responsible for this specific physical examination finding?
Explanation
Question 46
A 28-year-old overhead athlete presents with posterior shoulder pain and paresthesias over the lateral deltoid. MRI demonstrates isolated atrophy of the teres minor. Which of the following structures forms the inferior border of the anatomical space where the affected nerve is most likely compressed?
Explanation
Question 47
A 45-year-old man requires a sural nerve graft for a delayed brachial plexus reconstruction. During the harvest of the sural nerve in the distal posterior leg, which anatomical structure is located immediately adjacent to it and must be carefully protected?
Explanation
Question 48
A 32-year-old cyclist presents with numbness in the small finger and the ulnar half of the ring finger, along with weakness of the intrinsic hand muscles. Compression of the ulnar nerve in Guyon's canal is suspected. What structure forms the floor of this canal?
Explanation
Question 49
A thorough understanding of Hilton's Law is essential when performing diagnostic hip blocks or selective neurectomies for chronic hip pain. Which of the following nerves does NOT typically provide articular branches to the hip joint?
Explanation
Question 50
A 42-year-old mechanic presents with aching pain in the proximal lateral forearm and weakness in finger extension, but maintains normal strong wrist extension. The posterior interosseous nerve (PIN) is most commonly compressed by the proximal tendinous edge of which muscle?
Explanation
Question 51
During an anatomic posterolateral corner reconstruction of the knee, the surgeon identifies the normal femoral attachment of the fibular collateral ligament (FCL). Where is this specific attachment located relative to the lateral epicondyle?
Explanation
Question 52
A 60-year-old patient undergoes a lymph node biopsy in the posterior triangle of the neck and subsequently develops noticeable shoulder drooping and severe weakness with shoulder elevation. The nerve injured during this procedure exits the skull through which of the following foramina?
Explanation
Question 53
A 22-year-old man falls on an outstretched hand and sustains a scaphoid waist fracture, placing him at high risk for avascular necrosis of the proximal pole. The predominant intraosseous blood supply to the scaphoid enters at which specific location?
Explanation
Question 54
An anterolateral approach to the distal tibia and ankle joint is performed for a complex pilon fracture. During the superficial dissection, a specific nerve is identified crossing the surgical field and is protected. This nerve provides sensory innervation to which of the following areas?
Explanation
Question 55
Electromyography of a 35-year-old woman shows an anomalous neural connection in the forearm that carries motor fibers from the median nerve to the ulnar nerve. This normal variant is most likely to confound the clinical assessment of which of the following compressive neuropathies?
Explanation
Question 56
A 20-year-old collegiate baseball pitcher presents with medial elbow pain. Valgus stress testing reveals joint laxity at 30 degrees of elbow flexion. Which bundle of the ulnar collateral ligament (UCL) complex is the primary restraint to valgus stress at this angle, and what is its distal insertion site?
Explanation
Question 57
A 50-year-old woman undergoes arthroscopic shoulder stabilization for recurrent instability. The surgeon carefully evaluates and addresses pathology within the rotator interval. Which of the following structures is considered a standard normal content of the rotator interval?
Explanation
Question 58
A patient sustains a laceration to the flexor digitorum profundus (FDP) tendon of the middle finger, which is repaired primarily. Postoperatively, the patient experiences limited active flexion of the uninjured ring and small fingers. What anatomical feature primarily accounts for this phenomenon?
Explanation
Question 59
During a standard deltopectoral approach for a total shoulder arthroplasty, the internervous plane is developed to expose the anterior shoulder. What are the respective nerves supplying the two muscles that define this internervous plane?
Explanation
Question 60
A surgeon is performing a dorsal approach for the excision of a Morton's neuroma in the third web space of the foot. To fully decompress or resect the lesion, the surgeon must understand its relationship to the deep transverse metatarsal ligament. In normal anatomy, where does the common plantar digital nerve course relative to this ligament?
Explanation
Question 61
During a deltopectoral approach to the shoulder, the internervous plane is developed. This plane lies between muscles innervated by which of the following specific pairs of nerves?
Explanation
Question 62
A patient presents with progressive weakness in thumb adduction and finger abduction, but has intact sensation over the volar small finger and normal hypothenar muscle strength. A mass is suspected in Guyon's canal. Which anatomic zone is most likely affected?
Explanation
Question 63
During a deltopectoral approach to the shoulder, a nerve is encountered piercing the clavipectoral fascia medial to the coracoid process. This nerve primarily innervates which of the following structures?
Explanation
None
