AAOS, ABOS & OITE Anatomy MCQs (Set 2): High-Yield Skeletal, Joint & Muscle Systems

Key Takeaway
This high-yield question set for AAOS/ABOS/OITE exams focuses on essential orthopedic anatomy. It covers detailed skeletal system components, joint structures and their biomechanics, and critical muscle origins, insertions, and functions. Additionally, it addresses key neurovascular pathways relevant to orthopedic practice.
AAOS, ABOS & OITE Anatomy MCQs (Set 2): High-Yield Skeletal, Joint & Muscle Systems
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
To adequately expose the volar plate of the proximal interphalangeal joint of the finger, which of following pulleys is typically incised?

Explanation
Question 2
A 42-year-old patient has had a fever and low back pain for several days. Laboratory studies show an elevated erythrocyte sedimentation rate and a WBC count of 9,500 mm3 with 75% neutrophils. A CT scan is shown in Figure 15. Examination will most likely reveal what other findings?

Explanation
Question 3
Based on the diagram shown in Figure 16, what muscle derives its innervation from the nerve identified by the letter "A"?

Explanation
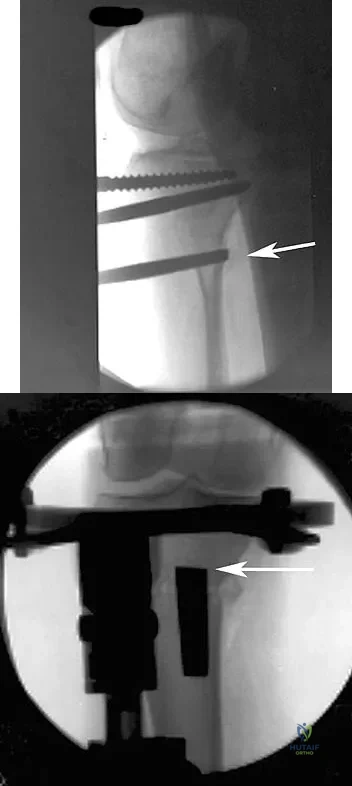
Question 4
In performing an opening wedge high tibial osteotomy at the tibial tubercle, the osteotome extends 5 mm posteriorly and centrally out of the bone as shown in Figures 17a and 17b. What is the first structure it enters?
Explanation
Question 5
The arrow in the axial T1-weighted MRI scan shown in Figure 18 is pointing to which of the following structures?

Explanation
Question 6
Osteonecrosis of the femoral head after intramedullary nailing in children is thought to be the result of injury to the

Explanation
Question 7
The illustration shown in Figure 19 shows a Chamberlain line. What is the most likely diagnosis?

Explanation
Question 8
Figures 20a and 20b show the sagittal and coronal T1-weighted MRI scans of a patient's left knee. Abnormal findings include

Explanation
Question 9
An ulnar nerve palsy at the level of the wrist is typically associated with deficits in the palmaris brevis, the hypothenar muscles, and what other groups of muscles?

Explanation
Question 10
Figures 21a and 21b show the radiographs of a 22-year-old man who has had progressive pain and swelling about the knee for the past 6 weeks. Examination reveals limited range of motion and fullness about the knee. What is the most likely diagnosis?

Explanation
Question 11
The anterolateral (Watson-Jones) approach to the hip exploits the intermuscular interval between the

Explanation
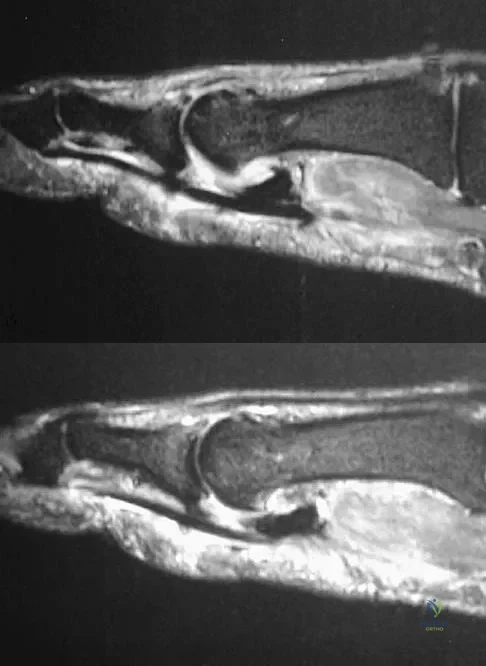
Question 12
An 8-month-old infant has an infection of the fingertip as shown in Figure 22. If neglected, the anticipated path of ascending infection is the fingertip, the flexor sheath, and the

Explanation
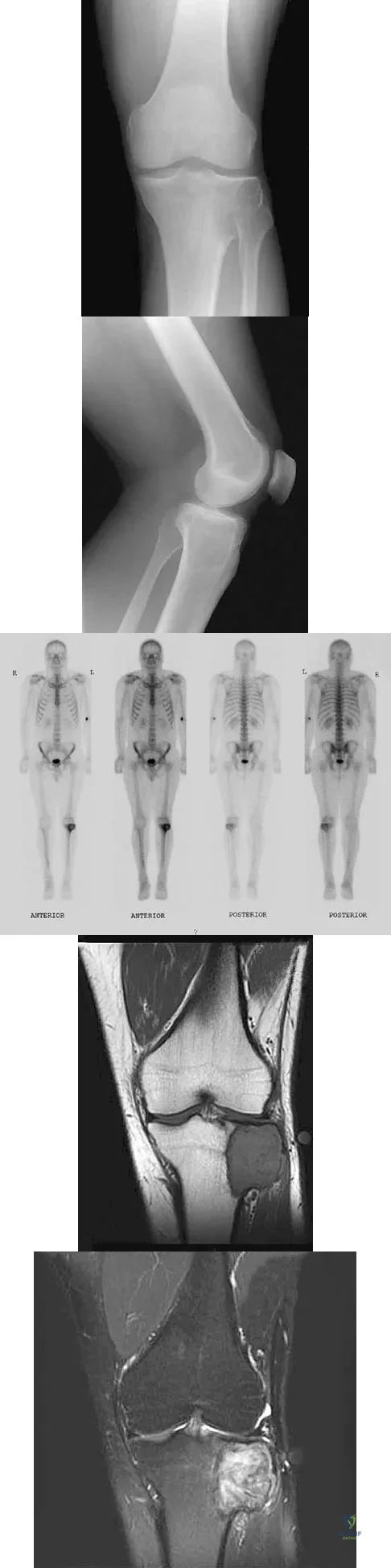
Question 13
A 24-year-old man has had pain in the left knee for the past several months. He reports that initially the pain was associated with weight-bearing activities, but it has now become more constant. He denies any swelling but reports a lateral fullness at the tibial plateau. Figures 23a through 23e show radiographs, a bone scan, and T1- and T2-weighted MRI scans. What is the most likely diagnosis?
Explanation
Question 14
Figure 24 shows an axial MRI scan of the ankle. The arrowhead is pointing to what structure?

Explanation
Question 15
During total hip arthroplasty, profuse bleeding is noted following predrilling for placement of an acetabular component screw. The drill most likely penetrated too deep in the

Explanation
Question 16
A posterolateral approach to the tibial plafond proceeds between what two muscles?

Explanation
Question 17
The brachialis muscle is innervated by what two nerves?

Explanation
Question 18
Figure 25 shows the CT scan of an adult patient who has neck pain following a motor vehicle accident. What is the most likely diagnosis?

Explanation
Question 19
Which of the following best describes the course of the ulnar nerve in the midforearm?

Explanation
Question 20
A 70-year-old former baseball catcher reports long-standing pain in the ring and little fingers. A gradient-echo MRI scan is shown in Figure 26. What is the most likely diagnosis?
Explanation
Question 21
In a postganglionic brachial plexus lesion at Erb's point (point of formation of the upper trunk by the C5 and C6 nerve roots), which of the following nerves will still function normally?

Explanation
Question 22
The posterior circumflex humeral artery and the axillary nerve usually lie in a space bordered superiorly by the

Explanation
Question 23
A patient notes pain under the first metatarsophalangeal joint following a soccer injury. The MRI scans shown in Figures 27a and 27b reveal what pathologic finding?
Explanation
Question 24
When performing the exposure for an anterior approach to the cervical spine, excessive retraction of the trachea and esophagus should be avoided to prevent injury of the

Explanation
Question 25
What is the first ossification center to appear radiographically in the pediatric elbow?

Explanation
Question 26
During the anterior (Henry) approach to the forearm, the surgeon must exploit a specific internervous plane to safely expose the radius. Which of the following correctly describes this proximal internervous plane?
Explanation
Question 27
The anterior (Smith-Petersen) approach to the hip provides excellent exposure for pelvic osteotomies and total hip arthroplasty. The superficial internervous plane for this approach utilizes which two muscles?
Explanation
Question 28
A posterior approach to the shoulder may place the axillary nerve at risk as it exits the quadrangular space. Which of the following structures forms the superior border of the quadrangular space?
Explanation
Question 29
During a posterolateral approach to the distal humerus, the radial nerve must be identified and protected. At approximately what distance proximal to the lateral epicondyle does the radial nerve pierce the lateral intermuscular septum?
Explanation
Question 30
Avascular necrosis of the proximal pole of the scaphoid is a known complication of scaphoid waist fractures due to its retrograde blood supply. The primary blood supply to the proximal pole enters via which of the following vessels?
Explanation
Question 31
In severe rotational ankle fractures, the deltoid ligament may be disrupted. Which component of the deltoid ligament complex is the primary static restraint to lateral displacement and external rotation of the talus?
Explanation
Question 32
During clinical assessment of the distal radioulnar joint (DRUJ) for instability, understanding the tensioning of the radioulnar ligaments is essential. Which ligamentous structure is under maximum tension when the forearm is placed in full supination?
Explanation
Question 33
Following a displaced femoral neck fracture in an adult, the femoral head is at high risk for osteonecrosis. The most significant contributor to the vascular supply of the adult femoral head is the:
Explanation
Question 34
Fractures of the talar neck frequently lead to avascular necrosis of the talar body. The body of the talus receives its major blood supply from the artery of the tarsal canal, which is a direct branch of the:
Explanation
Question 35
When evaluating a patient with recurrent anterior shoulder instability, the primary static restraint to anterior translation must be assessed. At 90 degrees of shoulder abduction and external rotation, which structure is the primary restraint?
Explanation
Question 36
The lumbrical muscles of the hand are unique in that they both originate from and insert onto tendons. Which of the following correctly describes the innervation of the lumbrical muscle associated with the ring finger?
Explanation
Question 37
The anterior cruciate ligament (ACL) is composed of two functional bundles named for their tibial insertion sites. Which of the following statements regarding the anteromedial (AM) bundle is correct?
Explanation
Question 38
The posterolateral (Kocher) approach to the elbow is frequently used for radial head fractures. This approach exploits an internervous plane between which two muscles?
Explanation
Question 39
When placing pedicle screws in the lumbar spine, understanding the changing regional anatomy is critical for safe trajectory. Compared to the T12 pedicle, the typical L5 pedicle is:
Explanation
Question 40
During a surgical release for a recalcitrant trigger finger, a specific annular pulley is incised. What is the location of this pulley relative to the digit's joints?
Explanation
Question 41
In the proximal forearm, the median nerve passes between the two heads of the pronator teres. Which of the following structures anatomically separates the median nerve from the ulnar artery at this level?
Explanation
Question 42
A surgeon is performing a posterolateral approach to the ankle for fixation of a posterior malleolus fracture. During the superficial dissection, the sural nerve must be protected. The sural nerve runs in close proximity to which structure?
Explanation
Question 43
During an anterolateral approach to the distal tibia, the superficial peroneal nerve must be identified and protected. At what approximate level does this nerve typically pierce the deep fascia to become subcutaneous?
Explanation
Question 44
The pes anserinus is frequently utilized as a harvest site for autograft in anterior cruciate ligament reconstruction. From anterior to posterior, what is the anatomical arrangement of these tendinous insertions on the proximal medial tibia?
Explanation
Question 45
During a radical axillary dissection, a nerve passing posterior to the axillary artery and innervating the latissimus dorsi is inadvertently injured. Which of the following describes the origin of this nerve?
Explanation
Question 46
The primary bony stabilizer of the Lisfranc joint complex is the base of the second metatarsal.
Which of the following accurately describes its articulation with the cuneiforms?
Explanation
Question 47
A patient sustains an injury to the posterolateral corner of the knee. The popliteofibular ligament is identified as a critical stabilizer. From which structure does it anatomically originate?
Explanation
Question 48
In the hand, the lumbrical muscles flex the metacarpophalangeal joints and extend the interphalangeal joints. What is the origin of the third lumbrical?
Explanation
Question 49
The rotator interval is a critical anatomical space in the anterior shoulder. Which of the following structures is NOT considered a border or content of the rotator interval?
Explanation
Question 50
An intracapsular femoral neck fracture frequently compromises the blood supply to the femoral head. Which artery provides the primary blood supply to the mature adult femoral head?
Explanation
Question 51
When performing a standard posterior approach to the lumbar spine, the surgeon exposes the pars interarticularis. Which neural structure lies immediately anterior to the pars interarticularis?
Explanation
Question 52
The central band of the forearm interosseous membrane is essential for longitudinal load transfer. What is the anatomical orientation of its fibers?
Explanation
Question 53
The anterior inferior tibiofibular ligament (AITFL) is commonly torn in syndesmotic ankle sprains. Where does this ligament primarily insert on the tibia?
Explanation
Question 54
During an ilioinguinal approach to the acetabulum, the surgeon must ligate the corona mortis to prevent massive hemorrhage. This structure is an anastomosis between which two vascular systems?
Explanation
Question 55
The triangular fibrocartilage complex (TFCC) stabilizes the distal radioulnar joint (DRUJ). Which component is the primary restraint to dorsal translation of the distal ulna when the forearm is in pronation?
Explanation
Question 56
The anterior bundle of the ulnar collateral ligament (UCL) of the elbow is the primary restraint to valgus stress. Where is its primary anatomical insertion on the ulna?
Explanation
Question 57
Entrapment of the suprascapular nerve at the spinoglenoid notch, often due to a paralabral cyst, typically results in isolated weakness of which muscle?
Explanation
Question 58
Following a proximal fibular fracture, a patient develops a deep peroneal nerve palsy. On physical examination, where would sensation most likely be decreased?
Explanation
Question 59
During anterior cervical spine surgery, aggressive dissection lateral to the uncovertebral joints puts the vertebral artery at risk. At which cervical level does the vertebral artery typically first enter the foramen transversarium?
Explanation
Question 60
When performing a lateral approach to the fibula, the superficial peroneal nerve is at risk as it exits the deep fascia to become subcutaneous. At approximately what distance proximal to the lateral malleolus does this typically occur?
Explanation
Question 61
The recurrent motor branch of the median nerve (the "million dollar nerve") provides critical motor function to the hand. Which of the following muscle combinations does it innervate?
Explanation
Question 62
The spring ligament is a critical static stabilizer of the longitudinal arch of the foot, often implicated in adult acquired flatfoot deformity. What are its precise anatomical attachments?
Explanation
Question 63
The quadrilateral space of the shoulder transmits the axillary nerve and the posterior circumflex humeral artery.
Which muscle defines the superior boundary of this space?

Explanation
Question 64
During a posterior approach to the hip (Kocher-Langenbeck), which of the following short external rotators should be preserved to protect the deep branch of the medial circumflex femoral artery?
Explanation
Question 65
When performing a deltoid-splitting surgical approach to the shoulder, the axillary nerve is typically found at what approximate distance distal to the lateral edge of the acromion?
Explanation
Question 66
During a volar (Henry) approach to the proximal radius, how should the forearm be positioned to best protect the posterior interosseous nerve (PIN)?
Explanation
Question 67
The popliteus tendon is a critical component of the posterolateral corner of the knee. In relation to the lateral collateral ligament (LCL) footprint, where does the popliteus tendon insert on the lateral femoral condyle?
Explanation
Question 68
During a percutaneous repair of an Achilles tendon rupture, the sural nerve is at highest risk of iatrogenic injury. At approximately what distance proximal to the calcaneal tuberosity does the sural nerve typically cross the lateral border of the Achilles tendon?
Explanation
Question 69
The "corona mortis" is a significant anatomic structure encountered during the ilioinguinal approach to the acetabulum. It represents a vascular anastomosis between which two systems?
Explanation
Question 70
During anterior cervical spine surgery, recognizing the course of the vertebral artery is vital. In the majority of individuals, the vertebral artery enters the transverse foramen at which cervical level?
Explanation
Question 71
Which of the following describes the typical motor innervation of the lumbrical muscles of the hand?
Explanation
Question 72
A 25-year-old athlete presents with medial winging of the scapula after a traction injury to the shoulder. Which nerve is most likely injured, and what are its contributing nerve roots?
Explanation
Question 73
The short head of the biceps femoris muscle plays a unique anatomical role in the posterior compartment of the thigh. It receives its motor innervation from which of the following nerves?
Explanation
Question 74
The subscapularis muscle is a crucial dynamic anterior stabilizer of the glenohumeral joint. What is its primary bony footprint insertion site?
Explanation
Question 75
Surgical decompression of the ulnar nerve at the elbow requires an understanding of the cubital tunnel boundaries. Which structure forms the true floor of the cubital tunnel?
Explanation
Question 76
During a carpal tunnel release, caution is required to avoid injuring the recurrent motor branch of the median nerve. In the majority of individuals, what is the anatomical relationship of this branch to the transverse carpal ligament?
Explanation
Question 77
The anterior cruciate ligament (ACL) consists of two main functional bundles. During knee flexion, which bundle is tightest and what is its primary stabilizing function?
Explanation
Question 78
The anterior inferior tibiofibular ligament (AITFL) is a critical stabilizer of the ankle syndesmosis. It originates from the Chaput tubercle on the tibia and inserts onto which bony landmark on the fibula?
Explanation
Question 79
In the normal lumbar spine anatomy, the exiting nerve root travels through the intervertebral foramen in what relation to the pedicle of the corresponding numbered vertebral body?
Explanation
Question 80
Vascular supply to the hand is provided by an extensive anastomotic network. The superficial palmar arch is primarily formed by the direct continuation of which vessel?
Explanation
Question 81
Talar neck fractures are notorious for causing avascular necrosis of the talar body. The dominant blood supply to the body of the talus is provided by the artery of the tarsal canal, which is a branch of which major artery?
Explanation
Question 82
During a deltopectoral approach for shoulder arthroplasty, the conjoined tendon is retracted medially. The nerve that pierces the coracobrachialis muscle typically enters it at what distance distal to the coracoid process?
Explanation
Question 83
During a direct lateral (Hardinge) approach to the hip, proximal extension of the gluteus medius split is typically limited to 3-5 cm superior to the greater trochanter to prevent injury to which nerve?
Explanation
Question 84
During a surgical exploration for radial tunnel syndrome, the surgeon identifies the most common site of compression of the posterior interosseous nerve. This structure is a fibrous band at the proximal edge of which of the following muscles?
Explanation
Question 85
An orthopedic surgeon is performing an anterior ilioinguinal approach for an acetabular fracture. Severe hemorrhage is encountered near the superior pubic ramus. This bleeding is most likely from an anastomotic vessel connecting which two arterial systems?
Explanation
Question 86
Following a radical mastectomy, a patient presents with a noticeable "winging" of the scapula with arm elevation. The injured nerve originates from which of the following brachial plexus segments?
Explanation
Question 87
The anterolateral (Watson-Jones) approach to the hip utilizes a superficial interval between the tensor fasciae latae and the gluteus medius. What is the innervation of these two muscles respectively?
Explanation
Question 88
A 28-year-old sustains a displaced talar neck fracture. The primary blood supply to the body of the talus, which is at highest risk of disruption in this injury, is provided by the artery of the tarsal canal. This artery is a direct branch of which of the following?
Explanation
Question 89
During a deltopectoral approach to the shoulder, the coracoid process may be osteotomized to improve exposure. The surgeon must be careful to avoid placing retractors too distally on the conjoined tendon to prevent injury to which nerve?
Explanation
Question 90
In reconstructing the posterolateral corner (PLC) of the knee, identifying anatomic landmarks is critical. On the lateral femoral condyle, where is the popliteus tendon attachment located relative to the fibular collateral ligament (FCL) origin?
Explanation
Question 91
A surgeon is performing an open reduction and internal fixation of a calcaneus fracture via an extensile lateral approach. Which nerve is at greatest risk of iatrogenic injury during the full-thickness subperiosteal dissection of the posterior vertical limb?
Explanation
Question 92
When performing the volar (Henry) approach to the proximal radius, the surgeon develops the interval between the pronator teres and the brachioradialis. Which vascular structure must be ligated and divided to fully mobilize the mobile wad laterally?
Explanation
Question 93
A patient develops weakness of the deltoid and teres minor following a posterior shoulder dislocation. The injured nerve passes through the quadrangular space. What muscle forms the superior border of this anatomic space?
Explanation
Question 94
A hamstring autograft is being harvested for an ACL reconstruction. The surgeon isolates the gracilis and semitendinosus tendons. What is the respective nerve supply to the individual muscles comprising the pes anserinus (Sartorius, Gracilis, Semitendinosus)?
Explanation
Question 95
Avascular necrosis of the proximal pole of the scaphoid is a known complication following a waist fracture. This occurs because the primary arterial supply to the scaphoid enters at which location?
Explanation
Question 96
During a lateral transpsoas approach to the lumbar spine (LLIF), the surgeon must navigate the lumbar plexus carefully to avoid neurologic deficit. Which nerve is classically found emerging directly from the anterior surface of the psoas major muscle?
Explanation
Question 97
A deep laceration to the hypothenar eminence severs the deep branch of the ulnar nerve. Assuming isolated injury to this branch, which of the following intrinsic hand muscles would most likely retain normal function?
Explanation
Question 98
The anterior (Smith-Petersen) approach to the hip exploits a true internervous plane. Which two nerves supply the respective muscles that form the superficial interval of this approach?
Explanation
None
