Orthopedic Anatomy MCQs (Set 3): Bone Structure, Joint Kinematics & Ligaments | ABOS & AAOS Review
Key Takeaway
This high-yield question set, Set 3, for the ABOS, AAOS, and OITE exams, thoroughly tests core orthopedic anatomical knowledge. It includes MCQs on detailed bone structure and histology, joint kinematics, ligament and tendon anatomy, and essential muscle origins and insertions.
Orthopedic Anatomy MCQs (Set 3): Bone Structure, Joint Kinematics & Ligaments | ABOS & AAOS Review
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 41-year-old man who plays golf regularly has had ulnar-sided wrist pain for the past several days after striking a tree root with a golf club. Examination reveals significant pain with resisted flexion of the ring and small fingers and tenderness over the hook of the hamate. Which of the following radiographic views would be most helpful in identifying the pathology of this injury?

Explanation
Question 2
What is the primary limiting membrane and mechanical support for the periphery of the physis?
Explanation
Question 3
What normal tissue has a low signal intensity (appears black) on both T1- and T2-weighted images?

Explanation
Question 4
A positive Froment sign indicates weakness of which of the following muscles?

Explanation
Question 5
Figure 28 shows an AP radiograph of a 54-year-old woman who underwent lumbar laminectomy and fusion at the L4 and L5 levels with placement of a bone stimulator 8 years ago. She also underwent a left total hip arthroplasty 2 years ago; aspiration of that joint now reveals that it is infected with a gram-positive cocci organism. History is also significant for IV drug use and human immunodeficiency virus (HIV). The patient reports fever, chills, and left flank and abdominal pain. Examination reveals significant pain with resisted left hip flexion and passive hip extension. She also has lumbar hyperlordosis. Which of the following studies would best identify the underlying cause of her infection?

Explanation
Question 6
A 55-year-old woman who underwent a left total hip arthroplasty 8 months ago using a modified Hardinger approach reports a persistent painless limp. Examination reveals that when she is not using a cane, she lurches to the left during weight bearing on the left lower extremity. An AP radiograph is shown in Figure 29. Which of the following hip muscle groups should be strengthened to improve the gait abnormality?

Explanation
Question 7
Figure 30 shows an axial cross section of extensor tendon anatomy in zone 7 of the wrist. What letter best depicts the location of the posterior interosseous nerve?

Explanation
Question 8
Figures 31a and 31b show the T1- and T2-weighted MRI scans of a patient's knee joint. What is the most likely diagnosis?

Explanation
Question 9
A 15-year-old boy reports feeling a pop and notes sudden giving way of the left knee while playing basketball. He has immediate pain and swelling in the knee. An AP radiograph is shown in Figure 32. A small avulsion fragment from the lateral tibial margin is the only finding. What is the most likely diagnosis?

Explanation
Question 10
What neurovascular structure is most at risk when performing an inside-out repair of the posterior horn of the medial meniscus?
Explanation
Question 11
Figure 33 shows the AP and lateral radiographs of an obese 58-year-old man who underwent a cementless total hip arthroplasty 6 years ago. He reports no pain, and examination reveals a normal gait and painless hip range of motion. What is the most likely diagnosis?

Explanation
Question 12
Which of the following muscles attaches to the coracoid process of the scapula?
Explanation
Question 13
Turf toe typically involves injury to which of the following structures of the great toe?
Explanation
Question 14
Figures 34a through 34c show an axial proton density (spin echo long TR, short TE) image, a sagittal inversion recovery (STIR) image, and a sagittal T1-weighted (short TR, short TE) image of the left thigh. What is the most likely diagnosis?
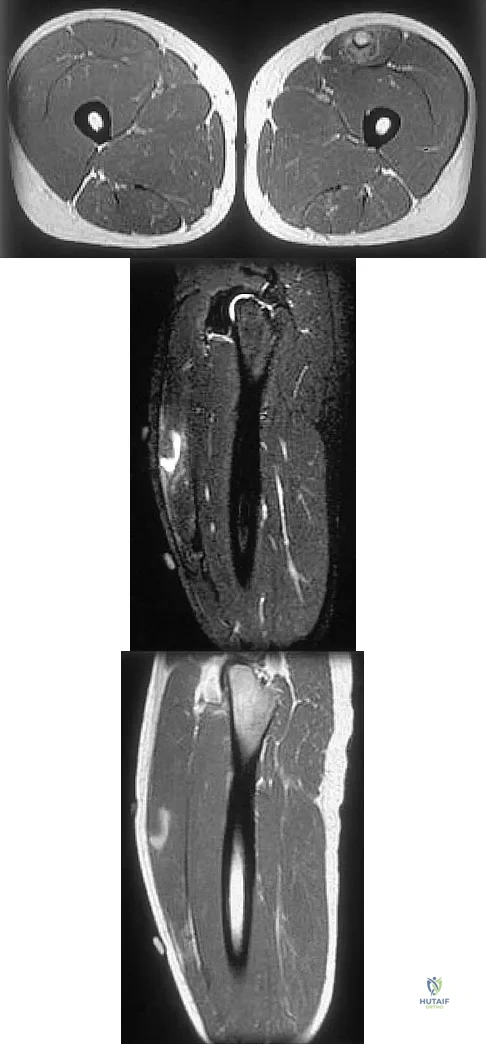
Explanation
Question 15
The artery located within the substance of the coracoacromial ligament is a branch of what artery?
Explanation
Question 16
Figures 35a and 35b show the axial T2-weighted and coronal T1-weighted MRI scans of a patient who has enlargement of the right thigh. What is the most likely diagnosis?
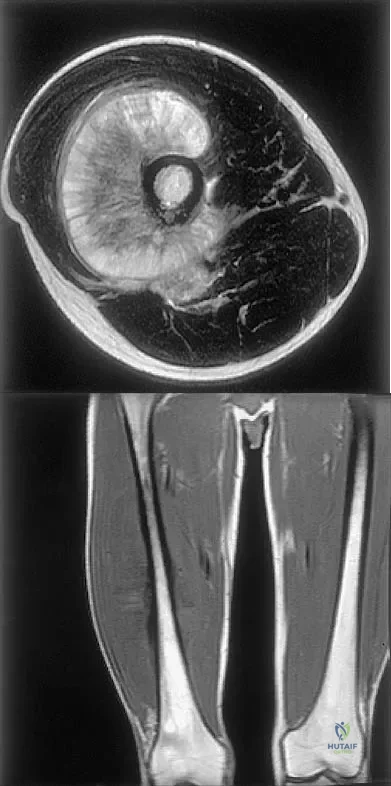
Explanation
Question 17
Figures 36a and 36b show the MRI scans of a patient who has shoulder weakness. What is the most likely diagnosis?
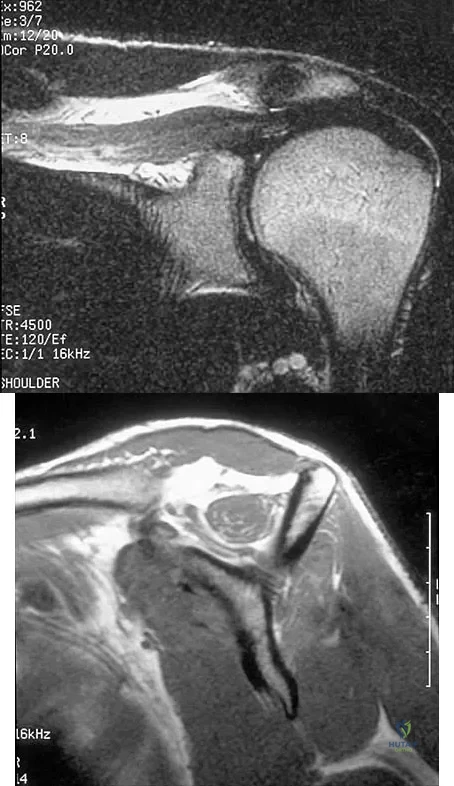
Explanation
Question 18
Figure 37 shows the T2-weighted MRI scan of the hip joint. What structure is labeled A?

Explanation
Question 19
The great medullary artery, also known as the Adamkiewicz artery, originates from which of the following arteries?
Explanation
Question 20
A patient who underwent total knee arthroplasty now reports a loss of sensation in the area circled in Figure 38. This area is innervated by which of the following nerves?

Explanation
Question 21
During an anterior approach to the shoulder, excessive traction on the conjoined tendon is most likely to result in loss of
Explanation
Question 22
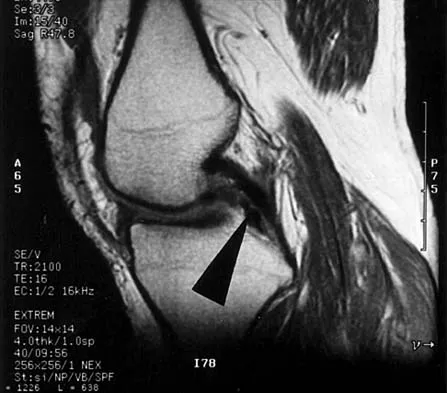
Figure 39 shows the sagittal T1-weighted MRI scan of a 27-year-old man who twisted his knee 2 weeks ago. The arrow is pointing to

Explanation
Question 23
Figure 40 shows the AP radiograph of a 55-year-old man who reports left knee pain. Which of the following conditions is least likely to produce this radiographic presentation?

Explanation
Question 24
Figure 41 shows the MRI scan of a 39-year-old man who has severe left groin and anterior thigh pain. What is the most likely diagnosis?

Explanation
Question 25
Iliosacral screws placed for stabilization of posterior pelvic ring injuries (eg, sacroiliac dislocation) that exit the sacrum anteriorly are most likely to injure which of the following structures?
Explanation
Question 26
In an anterior cruciate ligament (ACL)-deficient knee, which of the following structures acts as the primary secondary restraint to anterior tibial translation?
Explanation
Question 27
The coracoclavicular ligament complex is crucial for acromioclavicular joint stability. Which of the following describes the specific biomechanical function of the conoid ligament?
Explanation
Question 28
During the late cocking phase of throwing, the shoulder is maximally abducted and externally rotated. Which structural component is the primary restraint to anterior glenohumeral translation in this specific position?
Explanation
Question 29
A 24-year-old athlete sustains an inversion ankle sprain. Biomechanical studies indicate that the primary ligamentous restraint to inversion of the talus when the ankle is placed in maximal dorsiflexion is the:
Explanation
Question 30
Reconstruction of the medial ulnar collateral ligament (MUCL) of the elbow typically targets the anterior bundle. The anterior bundle is the primary restraint to valgus stress at which of the following elbow flexion angles?
Explanation
Question 31
In mature lamellar bone, osteons are bounded by a structurally distinct boundary that separates them from the surrounding interstitial lamellae. This histological structure is known as the:
Explanation
Question 32
Which of the following accurately describes the anatomy and function of Cleland's ligaments in the hand?
Explanation
Question 33
The dart-throwing motion of the wrist is clinically significant for rehabilitation after specific carpal injuries. Biomechanically, this functional motion occurs primarily at which of the following articulations?
Explanation
Question 34
During a lateral patellar dislocation, the medial patellofemoral ligament (MPFL) is typically ruptured. Biomechanically, the MPFL provides its greatest contribution to restraining lateral patellar translation at which knee flexion angle?
Explanation
Question 35
A patient with suspected anterior hip instability requires an assessment of the hip capsular ligaments. Which ligament is the thickest in the body and serves as the primary restraint to hip extension and external rotation?
Explanation
Question 36
The sternoclavicular (SC) joint relies heavily on ligamentous stabilizers due to poor bony congruity. Which ligament acts as the primary restraint to superior displacement of the medial clavicle?
Explanation
Question 37
Half of all cervical spine rotation occurs at the atlantoaxial (C1-C2) articulation. Which of the following ligaments is the primary restraint to anterior translation of the atlas on the axis?
Explanation
Question 38
The lateral meniscus is structurally and kinematically distinct from the medial meniscus. Which of the following is a defining anatomical feature of the lateral meniscus?
Explanation
Question 39
A pediatric patient sustains a distal radius fracture with apex volar angulation. Over a year, the bone straightens as formation occurs on the concave side and resorption on the convex side. This biomechanical response is described by:
Explanation
Question 40
A 55-year-old female presents with progressive flattening of her longitudinal arch. Pathology of the posterior tibial tendon is suspected. Which associated ligamentous structure is most commonly attenuated and primarily responsible for supporting the head of the talus?
Explanation
Question 41
In an anteroposterior compression (APC) pelvic ring injury, progressive disruption of ligaments leads to widening of the symphysis. Which sacroiliac (SI) ligament is the strongest and typically tears last, differentiating an APC-II from an APC-III injury?
Explanation
Question 42
The alar ligaments play a critical role in craniocervical stability. What is their primary biomechanical function?
Explanation
Question 43
A 28-year-old athlete undergoes knee arthroscopy. The surgeon identifies a ligamentous structure originating from the posterior horn of the lateral meniscus and inserting on the lateral aspect of the medial femoral condyle, passing anterior to the posterior cruciate ligament (PCL). What is this structure?
Explanation
Question 44
Regarding the microscopic structure of cortical bone, which of the following statements most accurately describes Volkmann's canals?
Explanation
Question 45
The screw-home mechanism of the knee is essential for locking the joint in terminal extension. Which of the following kinematic coupled motions occurs during the final 20 degrees of open-chain knee extension?
Explanation
Question 46
A 22-year-old baseball pitcher presents with anterior shoulder pain and apprehension. Biomechanical evaluation of the glenohumeral joint during the late cocking phase of throwing (90 degrees of abduction and maximal external rotation) demonstrates that anterior translation is primarily restrained by which structure?
Explanation
Question 47
A 34-year-old carpenter presents with wrist pain. Evaluation of his wrist kinematics reveals normal synchronous carpal motion. During active radial deviation of the wrist from a neutral position, what is the normal kinematic behavior of the scaphoid?
Explanation
Question 48
A 26-year-old football player sustains a direct blow to the proximal tibia with the knee flexed, resulting in a posterior cruciate ligament (PCL) tear. The PCL consists of two functional bundles. Which of the following best describes their tension patterns during knee range of motion?
Explanation
Question 49
In the process of bone remodeling, a distinct basophilic line is formed that marks the outer boundary of a newly created osteon. It is rich in osteopontin and deficient in collagen. What is this histological structure called?
Explanation
Question 50
A 19-year-old soccer player suffers an inversion ankle sprain. During the physical examination, the anterior drawer test is positive when the ankle is plantarflexed. Which ligament is primarily assessed, and what is its normal kinematic behavior?
Explanation
Question 51
In an acromioclavicular (AC) joint dislocation, the coracoclavicular (CC) ligaments are disrupted. Which of the following describes the correct anatomy and primary biomechanical function of the conoid ligament?
Explanation
Question 52
A 40-year-old man falls on an outstretched hand and develops radial-sided wrist pain. MRI reveals a complete rupture of the scapholunate interosseous ligament (SLIL). The SLIL has three distinct anatomic regions. Which region is the thickest, strongest, and primary restraint to abnormal scapholunate translation?
Explanation
Question 53
A 25-year-old professional javelin thrower presents with medial elbow pain. Valgus stress testing is positive at 30 degrees of elbow flexion. Which structure is the primary restraint to valgus instability in this position?
Explanation
Question 54
During the stance phase of normal human gait, the hip undergoes significant extension. Which capsuloligamentous structure is the primary restraint to hip hyperextension and external rotation, often referred to as the strongest ligament in the body?
Explanation
Question 55
A 60-year-old woman complains of anterior knee pain when descending stairs. Patellofemoral joint contact forces change dynamically with knee flexion. At what degree of knee flexion does the patella typically exhibit the maximum contact area with the femoral trochlea, distributing the highest joint reaction forces?
Explanation
Question 56
Fracture healing progresses through several overlapping phases. During the reparative phase, what type of bone is initially deposited by osteoblasts within the hard callus, characterized by a random, disorganized orientation of collagen fibers?
Explanation
Question 57
A clinician applies a constant deformation by placing a limb in a corrective cast. Over time, the internal tension within the constrained ligamentous structures gradually decreases. This viscoelastic property of ligaments is best defined as:
Explanation
Question 58
During the final 15 degrees of knee extension, the tibia must externally rotate relative to the femur to reach the fully locked position. Which anatomic feature is the primary driver of this 'screw-home' kinematic mechanism?
Explanation
Question 59
A 12-year-old is evaluated for osteopetrosis. A genetic defect affecting osteoclast function at the ruffled border is suspected. Which cell surface integrin is essential for the sealing zone of the osteoclast to adhere to the bone surface?
Explanation
Question 60
A 24-year-old overhead athlete presents with recurrent anterior shoulder instability. Biomechanical testing demonstrates maximum instability when the arm is positioned in 90 degrees of abduction and maximum external rotation. Which specific structure is the primary restraint to anterior translation in this position?
Explanation
Question 61
During rehabilitation of a scapholunate ligament repair, the therapist utilizes the 'dart thrower's motion' to minimize strain on the healing ligament. This motion primarily restricts movement at the midcarpal joint by linking which of the following coupled wrist positions?
Explanation
Question 62
A 13-year-old obese boy presents with groin pain and an obligatory external rotation of the hip with flexion. Radiographs confirm a slipped capital femoral epiphysis (SCFE). Through which specific histologic zone of the physis does this biomechanical failure primarily occur?
Explanation
Question 63
During an arthroscopic anterior cruciate ligament (ACL) reconstruction, careful attention is paid to the vascular supply of the notch. Which artery provides the primary blood supply to the native ACL?
Explanation
Question 64
In mature diaphyseal cortical bone, vascular channels that run transversely and connect the longitudinally oriented central canals of adjacent osteons are known as:
Explanation
Question 65
A 35-year-old runner complains of anterior knee pain during deep squats. Biomechanically, as the knee transitions from full extension to 90 degrees of flexion, how does the primary contact area on the articular surface of the patella migrate?
Explanation
Question 66
Following a grade II medial collateral ligament (MCL) sprain, the injured tissue undergoes a multiphase healing process. During the early remodeling phase, which type of collagen is most predominantly synthesized to bridge the defect before maturing into stronger tissue?
Explanation
Question 67
Normal kinematics of the subaxial cervical spine exhibit obligate coupled motions due to the spatial orientation of the facet joints. When a patient performs active lateral bending of the neck to the right, which obligate coupled motion naturally occurs?
Explanation
Question 68
A newborn is evaluated for delayed closure of the cranial sutures and absent clavicles. Genetic testing reveals a mutation in a master transcription factor essential for osteoblast differentiation. Which gene is most likely affected?
Explanation
Question 69
A patient is evaluated for chronic ankle instability. Clinical examination includes the anterior drawer test and talar tilt test. Regarding the kinematics of the lateral ankle ligaments, in which position is the calcaneofibular ligament (CFL) under the greatest tension?
Explanation
Question 70
When designing a hinged external fixator for a complex elbow fracture-dislocation, precise alignment of the fixator axis is critical. The instant center of rotation of the normal ulnohumeral joint is best described as:
Explanation
Question 71
Intramedullary nailing of a diaphyseal femur fracture profoundly affects local hemodynamics. In an intact long bone, the normal direction of arterial blood flow within the diaphyseal cortex is primarily:
Explanation
Question 72
During a pivot shift test for an ACL deficient knee, the tibia subluxates anteriorly in extension and reduces in flexion. Which specific anatomic bundle of the ACL is primarily responsible for resisting rotatory loads and anterior translation near full knee extension?
Explanation
Question 73
A military recruit develops a tibial stress fracture during week 4 of basic training. At a cellular level, fatigue failure in cortical bone under cyclical loading initially propagates through the formation of microcracks. What is the primary biological mechanism that attempts to repair this microdamage before macroscopic failure occurs?
Explanation
Question 74
A 22-year-old female presents with activity-related groin pain. Radiographic evaluation of her hip joint includes measurement of the lateral center-edge angle of Wiberg. This specific angle is utilized to evaluate the joint's biomechanical environment by quantifying:
Explanation
Question 75
When biomechanically testing a biological ligament, a cyclic loading and unloading curve demonstrates that the unloading path does not trace the same path as the loading curve. The area between these two curves represents energy lost as heat. This property is defined as:
Explanation
Question 76
Histological analysis of articular cartilage from a patient with early osteoarthritis reveals duplication of a specific boundary layer. What is the normal functional significance of the tidemark in articular cartilage?
Explanation
Question 77
A 25-year-old athlete undergoes ACL reconstruction. During graft tensioning, the surgeon considers the kinematics of the native ACL bundles. Which of the following statements correctly describes the tension patterns of the native ACL bundles during knee range of motion?
Explanation
Question 78
A 30-year-old mechanic falls onto an outstretched hand. Examination reveals tenderness over the dorsal wrist and a positive Watson scaphoid shift test. A complete tear of the scapholunate interosseous ligament (SLIL) is suspected. Which portion of this ligament is the most critical for maintaining carpal stability?
Explanation
Question 79
A 22-year-old rugby player sustains an acromioclavicular (AC) joint separation. During surgical reconstruction, the surgeon reconstructs the coracoclavicular (CC) ligaments. Which of the following accurately describes the anatomy of the native CC ligaments?
Explanation
Question 80
A 12-year-old boy presents with right hip pain and a limp. Radiographs demonstrate a slipped capital femoral epiphysis (SCFE). Through which specific zone of the growth plate does the failure primarily occur in this condition?
Explanation
Question 81
During clinical examination of knee kinematics, you observe the "screw-home" mechanism as the patient's knee reaches terminal extension. Which of the following best describes the osteokinematics and primary anatomical driver of this phenomenon?
Explanation
Question 82
A 24-year-old overhead throwing athlete presents with anterior shoulder instability. The physical examination reveals apprehension when the shoulder is placed in 90 degrees of abduction and maximum external rotation. Which ligamentous structure is the primary restraint to anterior translation in this specific position?
Explanation
Question 83
A bone biopsy from a patient with a suspected metabolic bone disorder is examined under microscopy. The pathologist identifies multiple vascular channels running longitudinally through the center of osteons, surrounded by concentric lamellae. What are these specific anatomical structures called?
Explanation
Question 84
A 28-year-old skier sustains an isolated medial collateral ligament (MCL) injury. To properly evaluate the integrity of the superficial MCL, the examiner applies a valgus stress test. At which degree of knee flexion does the superficial MCL provide the maximum percentage of the total restraining force against valgus stress?
Explanation
Question 85
A 32-year-old male dashboard injury victim undergoes a posterior cruciate ligament (PCL) reconstruction. The surgeon opts for a double-bundle technique to anatomically restore native kinematics. Which of the following accurately describes the behavior of the native PCL bundles?
Explanation
Question 86
A 26-year-old soccer player sustains a high ankle sprain with widening of the tibiofibular clear space on radiographs. Which of the following ligaments of the distal tibiofibular syndesmosis provides the greatest biomechanical strength and resistance to diastasis?
Explanation
Question 87
A patient is undergoing rehabilitation following a partial scapholunate ligament injury. The therapist emphasizes the "dart-thrower's motion" to allow functional wrist movement while minimizing stress on the healing scapholunate interval. Which of the following best describes the coupled motion and primary articulation of this kinematic pathway?
Explanation
Question 88
During a total hip arthroplasty, the surgeon uses a high-offset femoral stem to restore the patient's native anatomy. What is the primary biomechanical effect of increasing femoral offset on hip kinematics and joint reaction forces?
Explanation
Question 89
A 65-year-old man presents with neurogenic claudication. Lumbar MRI reveals severe central canal stenosis at L4-L5, largely secondary to hypertrophy of the posterior ligamentous structures. Which of the following extracellular matrix components is disproportionately high in the normal anatomy of the specific ligament contributing most to this compression?
Explanation
Question 90
A 45-year-old woman is being evaluated for a custom orthosis to correct a flexible pes planovalgus deformity. Understanding normal hindfoot kinematics is essential. The axis of rotation of the subtalar joint is best described by which of the following orientations?
Explanation
Question 91
A pathologist evaluates a bone biopsy from a healing fracture callus in a 19-year-old patient. The tissue is identified as primary woven bone. Compared to mature lamellar bone, which of the following histological or material properties is characteristic of woven bone?
Explanation
None
