
Posterior Spinal Fusion for Idiopathic Scoliosis
DEFINITION
Idiopathic scoliosis is a progressive three-dimensional spinal deformity in the absence of any congenital spinal anomaly or associated musculoskeletal condition.
Categorized as early onset (before the age of 5 years) or late onset (after the age of 5 years).3
ANATOMY
The spinal deformity is divided into three areas: proximal thoracic, main thoracic, and thoracolumbar/lumbar.
A proximal thoracic curve has an apex between T2 and T5. A main thoracic curve has and apex between T5 and T12 and a thoracolumbar/lumbar curve has an apex between T12 and L4.
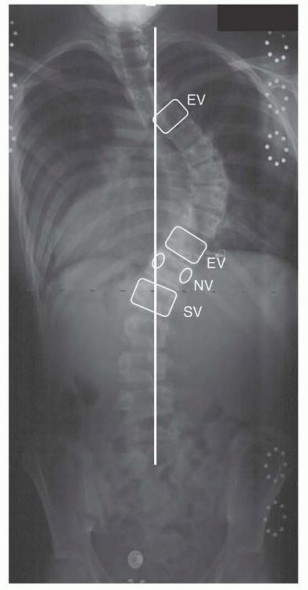
Vertebral definitions (FIG 1)
The end vertebrae define the extent of each curve and are most tilted from horizontal in the coronal plane. The stable vertebra is defined as the vertebra most closely bisected by the center sacral vertical line (CSVL).

FIG 1
• Vertebral definitions: The end vertebrae (EV) define the extent of each curve and are most tilted from horizontal in the coronal plane; the stable vertebra (SV) is defined as the vertebra most closely bisected by the CSVL; the neutral vertebra (NV) is defined as the least rotated vertebra in the axial plane based on the radiographic symmetry of its pedicles. (©SD PedsOrtho.)
The neutral vertebra is defined as the least rotated vertebra in the axial plane based on the radiographic symmetry of its pedicles.
PATHOGENESIS
Twin studies and observations of familial aggregation reveal significant genetic contributions to deformity progression.1, 13
Increased calmodulin (which regulates the contractile properties of muscles and platelets) and decreased melatonin (a calmodulin antagonist) levels have been found in patients with progressive scoliosis.7, 11
Differential growth rates in the anterior and posterior spinal column may cause imbalance in the sagittal plane with subsequent buckling of the vertebral column.5
NATURAL HISTORY
Risk factors for deformity progression include female gender, greater growth potential, thoracic curve location,
and larger curve magnitude.6, 15
Radiographic markers of skeletal maturity (state of the triradiate cartilage, Risser sign, carpal ossification, growth centers around the elbow) can be used to define a patient's remaining growth potential.
After skeletal maturity, curves less than 30 degrees tend not to progress, whereas curves greater than 50 degrees tend to progress about 1 to 2 degrees per year.19, 21
Thoracic lordosis and severe scoliosis (>80 degrees) result in restrictive lung disease and decreased pulmonary function.14, 22
PATIENT HISTORY AND PHYSICAL FINDINGS
Document medical history, developmental milestones, growth history, and family history.
Observation should assess for asymmetries of the neck, shoulders, ribs, waist, and hips. Cutaneous lesions such as hairy patches or sinuses may suggest spinal dysraphism, whereas café-au-lait spots or axillary freckling may suggest neurofibromatosis.
Adams forward bend test is used to identify a unilateral prominence of the thoracic rib cage or lumbar paraspinal muscles due to axial rotation of the spine.
Coronal decompensation can be identified as lateral translation of the C7 spinous process in relation to the gluteal cleft.
Clinical assessment of maturity based on Tanner stage. Peak growth velocity occurs approximately 6 to 12 months prior to the onset of menses in girls and the onset of axillary and facial hair in boys.17
Assessment of functional capacity is performed by analyzing gait, stance, motor and sensory function, and reflexes.


FIG 2 • Posteroanterior (A) and lateral (B) radiographs demonstrating a typical right thoracic deformity with apical lordosis. (©SD PedsOrtho.)
Abdominal reflexes should be assessed to rule out intramedullary lesions. Unilateral absence of the reflex suggests the need for a spine magnetic resonance imaging (MRI).
Limb length discrepancy can result in apparent scoliosis.



FIG 3 • Posteroanterior (A) and lateral (B) EOS images with representative coronal (C) and sagittal (D) three-dimensional (3-D) reconstructions. (©SD PedsOrtho.)
IMAGING AND OTHER DIAGNOSTIC STUDIES
Full-length, upright posteroanterior (FIG 2A), and lateral (FIG 2B) spinal radiographs are adequate for routine assessment.
Three-dimensional reconstructions using advanced, low-radiation imaging technology can provide important insights into the true scoliotic deformity (FIG 3).4
Lateral bending radiographs are important for preoperative planning to determine curve flexibility but are not required otherwise.
Advanced imaging studies including computed tomography and MRI can be used to identify neurologic or congenital abnormalities.
DIFFERENTIAL DIAGNOSIS
Congenital scoliosis (failure of vertebral formation or segmentation)
Neuromuscular scoliosis (cerebral palsy, spinal muscular atrophy, Duchenne muscular dystrophy) Syndromic scoliosis (osteochondrodystrophies, neurofibromatosis, Marfan syndrome)
NONOPERATIVE MANAGEMENT
Periodic observational monitoring is appropriate for skeletally immature patients with curves between 11 and 25 degrees. During periods of peak growth, more frequent evaluations (every 4 to 6 months) should be performed.
Skeletally immature patients (less than Risser 2) with documented curve progression to greater than 25 degrees
or 30 degrees on initial presentation can be treated with a rigid thoracolumbosacral orthosis.2
Bracing has been shown to successfully decrease the progression of high-risk curves during the adolescent growth spurt. A dose-dependent relationship between hours of brace wear and success with bracing has been identified.16, 20
A coordinated effort between the patient, the treating physician, and the orthotist is required to optimize success with bracing.
SURGICAL MANAGEMENT
Surgical goals are as follows:
Obtain three-dimensional and well-balanced deformity correction while fusing as few motion segments as possible.
Obtain a solid arthrodesis to prevent deformity progression.
Indications
The decision to proceed with surgical treatment is based on curve magnitude, the clinical deformity, and the risk for further progression.
In general, skeletally immature patients with progressive curves greater than 45 or 50 degrees or skeletally mature patients with curves greater than 50 degrees can be considered for surgical intervention.
Preoperative Planning: Fusion Levels
The primary driver of the scoliotic deformity is either the thoracic curve or the thoracolumbar/lumbar curve.
Compensatory curves occur adjacent to the primary deformity (major curve) seemingly in an attempt to maintain coronal or sagittal balance.
Thoracic Major Curves
The main decision is to selectively fuse the thoracic spine or fuse both the thoracic and lumbar spine. The Lenke classification system can be used to guide this decision.8
For 1AR curves (main thoracic curve with L4 tilt to the right), the lowest instrumented vertebra (LIV) should be the vertebral body whose concave pedicle is last touched by the CSVL (FIG 4A).
For 1AL/1B curves (main thoracic curves with L4 tilt to the left), the LIV should be the stable vertebra or one proximal to the stable vertebra but never short of the end vertebra (FIG 4B).
1C curves
For a selective thoracic fusion, the LIV should be the stable vertebra or one distal to the stable vertebra.
With a significantly rotated compensatory lumbar curve, an effort should be made to counter-rotate the distal vertebral body to allow for maximum spontaneous lumbar curve correction.
Upper instrumented vertebral (UIV) body selection in thoracic primary curves.
If the left shoulder is higher than the right shoulder, the UIV should be T1 or T2. If the shoulders are level, the UIV should be T3.
If the left shoulder is lower, the UIV should be T4 or T5.
The sagittal plane should also be analyzed when selecting the UIV. The instrumented fusion should include any proximal areas of focal hyperkyphosis.
Thoracolumbar/Lumbar Major Curves
For thoracolumbar/lumbar and structural thoracolumbar/lumbar curves with major thoracic curves (double major pattern), LIV should be the end vertebra.


FIG 4 • A. Lenke 1AR curve (L4 tilt to the right) with LIV of L2 (vertebral body whose pedicle is last touched by the CSVL). B. Lenke 1B curve (L4 tilt to the left) with LIV of L1 (stable vertebra). (©SD PedsOrtho.)
Main decision is to fuse to L3 or L4.
The LIV should be L3 if the L3-L4 disc is parallel or wedged open opposite to the side of the apex of the curve.
The LIV should be L4 if the L3-L4 disc is wedged open in the same direction as the apex of the curve (ie, L4 is the end vertebra) (FIG 5).
The UIV should be the end vertebra or more proximal if thoracolumbar junctional kyphosis is present. Use the thoracic curve UIV criteria if both thoracic and lumbar curves are being fused.


FIG 5 • Posteroanterior (A) and lateral (B) radiographs of a double major curve with the L3-L4 disc open toward the apex. (©SD PedsOrtho.)
TECHNIQUES
-
Posterior Spinal Exposure and Instrumentation
Standard posterior spinal exposure with segmental facetectomies and pedicle screw placement (detailed description in Chap. 84) (TECH FIG 1A-C).
Proximal foundation of four fixation points
We prefer to use hooks at the most proximal level to limit soft tissue dissection and provide a less rigid transition to the uninstrumented spine in an effort to minimize proximal junctional kyphosis.




TECH FIG 1 • A. Posterior spinal exposure. B. Ultrasonic bone scalpel (Misonix, Inc., Farmingdale, NY) used to perform facetectomies. C. Uniplanar pedicle screws placed segmentally using freehand technique. D. Posteroanterior radiograph of a Lenke 1AL curve (L4 tilt to the left). E. After posterior instrumented spinal fusion from T5 to T12. LIV is one proximal to stable. High-density fixation used on the concavity of the deformity and low density on the convexity. (A-C: ©SD PedsOrtho.)
High-density fixation on the concavity of the deformity to resist the posteriorly directed loads involved in correcting the lordotic thoracic spine.
Fewer fixation points are required on the convexity, as the deformity correction forces are anteriorly directed at the apex (TECH FIG 1D,E).
Distal foundation of four fixation points.
What if proximal pedicle screw fixation is limited secondary to anatomic deformity or missed screw placement?
Hooks can be used to create a claw construct on the right proximal end of construct (proximal transverse process hook and adjacent pedicle hook) and upgoing hooks can be used on the left proximal end (pedicle hooks).
1. ## Deformity Correction Technique
Posterior spinal releases (Ponte-type osteotomy) should be performed at the apex of the deformity based on the amount of sagittal plane correction required (TECH FIG 2).
Aggressive Differential Rod Contouring
Overbend kyphosis in concave rod and underbend kyphosis on convexity (TECH FIG 3A,B)
Change in rod shape (unbending during rod approximation) determines the force of correction (TECH FIG 3C).
Rod shape, material, and diameter are the primary determinants of correction (TECH FIG 3D): High-strength rods: stainless steel or cobalt chromium
Low-strength rods: titanium
Rod Insertion
Concave rod is inserted first and rotated into position to obtain initial deformity correction (TECH FIG 4A). Anteriorly directed counterforce applied to the convex rib hump to limit increasing rotational deformity (TECH FIG 4B).
Convex rod is inserted proximally and cantilevered into distal fixation points (TECH FIG 4C). This second rod applies anteriorly directed force on the convexity of the spine and results in axial derotation of the vertebral bodies (TECH FIG 4D).
Segmental Vertebral Manipulation and Completion
The rods are then locked into proper sagittal plane only at the neutral vertebra.


TECH FIG 2 • Ponte-type osteotomies with excision of the spinous process, intraspinous ligaments, superior articulating facet, capsule, and ligamentum flavum. (©SD PedsOrtho.)


 TECH FIG 3
•
A.
Aggressive differential rod contouring with overcontouring the concave rod.
B.
Intraoperative tracing of the two rods demonstrating difference between concave (left) and convex (right) rod contour.
C.
Change in rod shape (blue arrows) determines the force of correction (white arrow). An ultra-high-strength stainless steel rod is used to pull the concavity posteriorly in an attempt to correct the apical lordosis.
D.
Comparison of rod material properties and ability to withstand plastic deformation. (
A,C:
©SD PedsOrtho.)
TECH FIG 3
•
A.
Aggressive differential rod contouring with overcontouring the concave rod.
B.
Intraoperative tracing of the two rods demonstrating difference between concave (left) and convex (right) rod contour.
C.
Change in rod shape (blue arrows) determines the force of correction (white arrow). An ultra-high-strength stainless steel rod is used to pull the concavity posteriorly in an attempt to correct the apical lordosis.
D.
Comparison of rod material properties and ability to withstand plastic deformation. (
A,C:
©SD PedsOrtho.)
Starting at the neutral vertebra, each segment is then manipulated (moving proximal one level at a time up to the apex of the deformity) in three-dimensional space to assist the rod in regaining some of its original shape (TECH FIG 5).
Segmental distraction in the concavity and compression on the convexity are used to increase kyphosis and improve coronal plane deformity.
Decortication of the posterior elements is performed. Vancomycin powder, local bone autograft and allograft are placed to achieve a midline arthrodesis.



TECH FIG 4 • A. The concave, overcontoured rod is inserted first and rotated into position while applying
an anteriorly directed force on the contralateral ribs.
B.
Distraction is used to lengthen the posterior column, correct the apical lordosis, and allow the rod to spring back and regain some of its precontoured shape.
C.
The convex rod is then inserted and cantilevered into the distal fixation.
D.
Differential rod contouring indirectly enables vertebral derotation about a point in the posterior vertebral body (typical center of axial rotation). (©SD PedsOrtho.)




TECH FIG 5 • Segmental vertebral manipulation is performed starting at the neutral vertebra and working proximal one level at a time toward the apex of the deformity. A. Premanipulation at T11-T12 (neutral vertebra). B. Postmanipulation at T11-T12. C. Premanipulation at T10-T11. D. Post-manipulation at T10-T11. Simultaneous distraction in the concavity allows further three-dimensional deformity correction. (©SD PedsOrtho.)
PEARLS AND PITFALLS
| Perform a closing ▪ Final set screw tightening, decortication, bone graft and antibiotic timeout to ensure all powder placement, and post-deformity correction neuromonitoring. essential steps are
completed.
| Overcorrection of the thoracic curve
1. Iatrogenic elevation of the left shoulder can occur.
2. Nonstructural upper thoracic curves based on the Lenke classification guidelines (bend to <25 degrees) may need to be included in the instrumentation and fusion to control postoperative shoulder height.
Immature patients with open triradiate cartilage
1. Deformity progression and/or crankshaft may occur.
2. Consider concomitant anterior fusion procedures to avoid this complication.
Axial plane correction (vertebral derotation)
1. Iatrogenic thoracic flatback can occur without posterior column lengthening.
2. Ponte-type osteotomies allow correction of thoracic lordosis to achieve three-dimensional deformity correction.
Wide posterior releases (Ponte-type osteotomies)
3. Should be covered with long strips of autograft to protect the neural elements and avoid bone graft in the canal.
POSTOPERATIVE CARE
The patient is admitted to the orthopaedic floor postoperatively.
Patient-controlled analgesia used postoperatively and transitioned to oral narcotic medication once tolerating fluids.
Physical therapy begins on the first postoperative day to sit and stand with assistance. Progression to ambulation on subsequent days.
No postoperative bracing is required.
Upright postoperative radiographs can be used to assess three-dimensional deformity correction (FIG 6).
Axial plane correction can be approximated by assessing the position of bilateral pedicle screw tips in relation to the rods on a posteroanterior radiograph18 or the projection of the rods in relation to one another on the lateral radiograph.9

 FIG 6
• Posteroanterior (
A
) and lateral (
B
) radiographs after a T2-L4 posterior instrumented spinal fusion in the patient in FIG 5. (©SD PedsOrtho.)
FIG 6
• Posteroanterior (
A
) and lateral (
B
) radiographs after a T2-L4 posterior instrumented spinal fusion in the patient in FIG 5. (©SD PedsOrtho.)
OUTCOMES
Expect 50% to 70% correction of the coronal plane deformity. May consider undercorrection in a selective thoracic fusion to balance the lumbar coronal plane deformity.
Expect about 50% rib hump correction despite advanced techniques to axially derotate vertebral bodies (likely secondary to rib deformity).
Preservation of a greater number of vertebral motion segments allows for greater distribution of functional motion across the remaining unfused levels.12
Recent meta-analysis of mid- to long-term outcomes (average 14.9 year follow-up) after three commonly used posterior spinal instrumentation and fusion techniques demonstrated that Harrington rods had a
detrimental effect on the sagittal alignment. Cotrel-Dubousset constructs resulted in a greater degree of
correction in the coronal and sagittal planes; however, all-pedicle screw constructs showed lower risk of complications or need for revision surgery.10
COMPLICATIONS
Most common complications of posterior procedures for idiopathic scoliosis are instrumentation related (1.6%) and wound related (1.2%).
Instrumentation complications: broken rods/screws, misplaced screws, proximal junctional kyphosis, screw loosening, pseudarthrosis
Wound complications: erythema, hypertrophic scar, pain, dehiscence, hematoma, seroma, abscess/deep infection
Balance complications: deformity progression, adding-on, crankshaft
Medical complications: blindness, death, myocardial infarction, vocal cord paresis, gastrointestinal complications
Pulmonary complications: aspiration, atelectasis, hemithorax, pneumonia, pleural effusion
Neurologic complications: decreased neuromonitoring signals, paresthesias, femoral cutaneous neuralgia, lower extremity weakness, pain
Hematologic complications: require blood transfusion, excessive blood loss, transfusion reaction
Scientific References
- 1. Andersen MO, Thomsen K, Kyvik KO. Adolescent idiopathic scoliosis in twins: a population-based survey. Spine 2007;32:927-930. [View Source / PubMed]
- 2. Blount WP. Use of the Milwaukee brace. Orthop Clin North Am 1972;3:3-16. [View Source / PubMed]
- 3. Dickson RA. Conservative treatment for idiopathic scoliosis. J Bone Joint Surg Br 1985;67:176-181. [View Source / PubMed]
- 4. Glaser DA, Doan J, Newton PO. Comparison of 3-dimensional spinal reconstruction accuracy: biplanar radiographs with EOS versus computed tomography. Spine 2012;37:1391-1397. [View Source / PubMed]
- 5. Guo X, Chau WW, Chan YL, et al. Relative anterior spinal overgrowth in adolescent idiopathic scoliosis: results of disproportionate endochondral-membranous bone growth. J Bone Joint Surg Br 2003; 85:1026-1031. [View Source / PubMed]
- 6. Karol LA, Johnston CE II, Browne RH, et al. Progression of the curve in boys who have idiopathic scoliosis. J Bone Joint Surg Am 1993;75:1804-1810. [View Source / PubMed]
- 7. Kindsfater K, Lowe T, Lawellin D, et al. Levels of platelet calmodulin for the prediction of progression and severity of adolescent idiopathic scoliosis. J Bone Joint Surg Am 1994;76:1186-1192. [View Source / PubMed]
- 8. Lenke LG, Betz RR, Harms J, et al. Adolescent idiopathic scoliosis: a new classification to determine extent of spinal arthrodesis. J Bone Joint Surg Am 2001;83:1169-1181. [View Source / PubMed]
- 9. Liu RW, Yaszay B, Glaser D, et al. A method for assessing axial vertebral rotation based on differential rod curvature on the lateral radiograph. Spine 2012;37:E1120-E1125. [View Source / PubMed]
- 10. Lykissas MG, Jain VV, Nathan ST, et al. Mid- to long-term outcomes in adolescent idiopathic scoliosis after instrumented posterior spinal fusion: a meta-analysis. Spine 2013;38:E113-E119. [View Source / PubMed]
- 11. Machida M, Dubousset J, Imamura Y, et al. Melatonin. A possible role in pathogenesis of adolescent idiopathic scoliosis. Spine 1996;21: 1147-1152. [View Source / PubMed]
- 12. Marks M, Newton PO, Petcharaporn M, et al. Postoperative segmental motion of the unfused spine distal to the fusion in 100 patients with adolescent idiopathic scoliosis. Spine 2012;37:826-832. [View Source / PubMed]
- 13. Ogilvie JW, Braun J, Argyle V, et al. The search for idiopathic scoliosis genes. Spine 2006;31:679-681. [View Source / PubMed]
- 14. Pehrsson K, Bake B, Larsson S, et al. Lung function in adult idiopathic scoliosis: a 20 year follow up. Thorax 1991;46:474-478. [View Source / PubMed]
- 15. Peterson LE, Nachemson AL. Prediction of progression of the curve in girls who have adolescent idiopathic scoliosis of moderate severity. Logistic regression analysis based on data from The Brace Study of the Scoliosis Research Society. J Bone Joint Surg Am 1995;77:823-827. [View Source / PubMed]
- 16. Rowe DE, Bernstein SM, Riddick MF, et al. A meta-analysis of the efficacy of non-operative treatments for idiopathic scoliosis. J Bone Joint Surg Am 1997;79:664-674. [View Source / PubMed]
- 17. Sanders JO, Little DG, Richards BS. Prediction of the crankshaft phenomenon by peak height velocity. Spine 1997;22:1352-1356. [View Source / PubMed]
- 18. Upasani VV, Chambers RC, Dalal AH, et al. Grading apical vertebral rotation without a computed tomography scan: a clinically relevant system based on the radiographic appearance of bilateral pedicle screws. Spine 2009;34:1855-1862. [View Source / PubMed]
- 19. Weinstein SL. Idiopathic scoliosis. Natural history. Spine 1986;11: 780-783. [View Source / PubMed]
- 20. Weinstein SL, Dolan LA, Wright JG, et al. Effects of bracing in adolescents with idiopathic scoliosis. N Engl J Med 2013;369:1512-1521. [View Source / PubMed]
- 21. Weinstein SL, Ponseti IV. Curve progression in idiopathic scoliosis. J Bone Joint Surg Am 1983;65:447-455. [View Source / PubMed]
- 22. Winter RB, Lovell WW, Moe JH. Excessive thoracic lordosis and loss of pulmonary function in patients with idiopathic scoliosis. J Bone Joint Surg Am 1975;57:972-977. [View Source / PubMed]
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding posterior-spinal-fusion-for-idiopathic-scoliosis