Posterior Spinal Exposure for Scoliosis Correction: An Intraoperative Masterclass
Key Takeaway
This masterclass provides an immersive, granular guide to posterior spinal exposure for scoliosis. Fellows will learn intricate surgical anatomy, meticulous patient positioning, and step-by-step intraoperative execution from incision to deep subperiosteal dissection. Emphasis is placed on neurovascular preservation, precise instrument use, and critical pearls for managing potential pitfalls, ensuring a comprehensive understanding of this foundational procedure.
Comprehensive Introduction and Patho-Epidemiology
The surgical management of scoliosis represents one of the most formidable challenges and rewarding endeavors in orthopedic surgery. As spine surgeons, we are tasked with correcting a complex, dynamic deformity while simultaneously safeguarding the delicate neural elements housed within the spinal canal. The posterior spinal exposure is the foundational gateway to this correction. It is not merely a rote series of incisions; it is a meticulously orchestrated dissection that must respect the intricate three-dimensional pathoanatomy of the scoliotic spine. A masterful exposure provides the necessary visualization for safe instrumentation, facilitates a robust arthrodesis bed, and minimizes intraoperative blood loss, thereby setting the stage for optimal coronal and sagittal realignment.
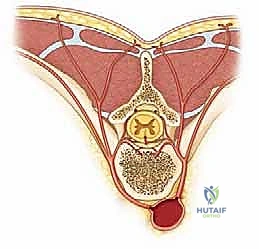
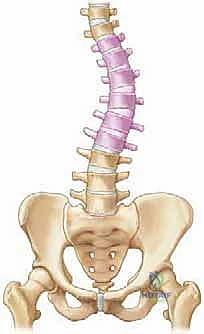
To execute this exposure flawlessly, one must first possess an intimate understanding of the underlying patho-epidemiology. Scoliosis is fundamentally a three-dimensional torsional deformity of the spine and rib cage. It is characterized by lateral deviation in the coronal plane, abnormal alignment in the sagittal plane (frequently presenting as thoracic lordoscoliosis in adolescent idiopathic variants), and, most critically, vertebral rotation in the transverse plane. This axial rotation dictates the spatial orientation of the posterior elements. In a scoliotic spine, the vertebral bodies rotate toward the convexity of the curve, which paradoxically drives the spinous processes toward the concavity. Consequently, the dural sac is often displaced toward the concavity, and the aorta may migrate posterolaterally relative to its normal anatomical position. These spatial alterations must be at the forefront of the surgeon’s mind during deep subperiosteal dissection and subsequent pedicle cannulation.
The Three-Dimensional Nature of Scoliosis
The complexity of scoliosis cannot be overstated when viewing the spine purely through an anteroposterior or lateral radiographic lens. The true deformity is a helical distortion. The apical vertebrae exhibit the most profound morphological changes, including wedging of the vertebral bodies and distortion of the pedicles. On the concavity of the curve, the pedicles are often sclerotic, narrowed, and dysmorphic, presenting a significant challenge for screw placement. The posterior elements, including the laminae and facets, are thickened and foreshortened on the concavity, while they are stretched and thinned on the convexity.
Furthermore, the rib cage undergoes secondary deformation. The ribs on the convex side are pushed posteriorly, creating the characteristic rib hump observed during the Adams forward bend test. Conversely, the ribs on the concave side are crowded and pushed anteriorly, reducing intrathoracic volume and potentially leading to restrictive pulmonary disease in severe cases. When performing our posterior exposure, recognizing this rotational asymmetry is crucial. The surgeon will encounter the convex transverse processes much more superficially than the concave transverse processes, which dive deep into the surgical field and are often obscured by contracted paraspinal musculature.
Etiological Classification and Progression Dynamics
We broadly categorize scoliosis by its etiology, as the underlying diagnosis heavily influences curve progression, flexibility, and surgical strategy. Idiopathic scoliosis remains the most prevalent, with Adolescent Idiopathic Scoliosis (AIS) constituting the vast majority of cases presenting to the operative theater. AIS typically manifests between 10 and 18 years of age. While its exact pathogenesis remains elusive—likely a multifactorial interplay of genetic, biomechanical, and neuro-hormonal factors—a positive family history is present in approximately 30% of patients. Crucially, the risk of curve progression is inextricably linked to the patient's remaining skeletal growth. Females are disproportionately affected by progressive curves requiring surgery, with a 5:1 female-to-male ratio for curves exceeding 20 degrees.
Congenital scoliosis, conversely, arises from embryological failures of vertebral formation (e.g., hemivertebrae) or segmentation (e.g., unsegmented bars), occurring during the first six weeks of gestation. These curves are often rigid and possess a highly variable natural history. The highest risk of relentless progression—approaching 100%—is associated with a unilateral unsegmented bar paired with a contralateral hemivertebra. Congenital deformities require heightened vigilance during posterior exposure due to the high incidence of associated intraspinal anomalies, such as tethered cord, diastematomyelia, or syringomyelia, which necessitate preoperative MRI evaluation.
Neuromuscular scoliosis develops secondary to underlying myopathic or neuropathic conditions, such as cerebral palsy, Duchenne muscular dystrophy, or spinal muscular atrophy. These curves are typically long, sweeping, and often involve the pelvis, leading to significant pelvic obliquity. The posterior paraspinal musculature in these patients is frequently atrophic, fibrotic, or spastic, altering the tactile feedback during surgical dissection. Furthermore, these patients often present with significant medical comorbidities, osteopenia, and impaired nutritional status, demanding a highly efficient surgical exposure to minimize blood loss and physiological stress.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of posterior spinal anatomy is the sine qua non of safe and effective scoliosis surgery. The posterior approach exploits the segmental innervation and vascular supply of the paraspinal musculature, allowing the surgeon to develop an internervous and intermuscular plane directly down the midline raphe. By adhering strictly to the subperiosteal plane, we can expose the posterior elements from the spinous processes out to the tips of the transverse processes while minimizing muscular trauma and hemorrhagic complications.
The biomechanical rationale for a wide posterior exposure is twofold. First, it provides the necessary anatomical footprint for the placement of segmental instrumentation (pedicle screws, hooks, or sublaminar wires), which act as anchors to apply corrective forces—such as derotation, translation, and compression/distraction—to the scoliotic spine. Second, and equally important, it exposes a massive surface area of decorticated host bone (laminae, facets, and transverse processes) essential for achieving a robust, contiguous posterior or posterolateral arthrodesis. Without a solid fusion, any instrumentation construct will inevitably fail due to metal fatigue.
Surface Landmarks and Topographical Anatomy
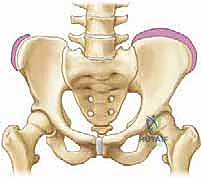
Accurate intraoperative navigation begins with the identification of palpable surface landmarks, assessed once the patient is carefully positioned prone. The vertebra prominens (C7) serves as the most reliable cephalad landmark at the cervicothoracic junction. Moving caudally, the superior angle of the scapula generally aligns with the T3 spinous process, the scapular spine with T4, and the inferior angle of the scapula with T7. These scapular landmarks provide an excellent rapid reference for thoracic levels, though they can be slightly altered by severe thoracic deformity.
In the lumbar spine, the iliac crests are the paramount landmarks. A line drawn connecting the highest points of the iliac crests (Tuffier's line) typically intersects the L4-L5 interspace or the L4 spinous process. The posterior superior iliac spines (PSIS) are palpable as distinct bony prominences, usually corresponding to the L5-S1 interspace. While these surface landmarks provide a reliable initial roadmap, the profound rotational deformity and coronal translation inherent to severe scoliosis can distort these relationships. Therefore, intraoperative fluoroscopy remains the definitive method for confirming vertebral levels prior to making the definitive fascial incision.
Musculotendinous Layers and the Internervous Plane
The posterior spinal musculature is arranged in distinct layers, all of which are segmentally innervated by the dorsal rami of the exiting spinal nerves. The superficial layer, the erector spinae, consists of the iliocostalis (lateral), longissimus (intermediate), and spinalis (medial) muscles. These powerful extensor muscles are enveloped by the robust thoracolumbar fascia. Beneath the erector spinae lies the deep, intrinsic layer, collectively known as the transversospinalis group, which includes the multifidus, rotatores, intertransversarii, and interspinous muscles. These shorter muscles are intimately attached to the laminae, facet capsules, and transverse processes.
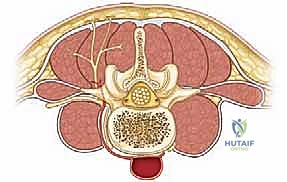
The surgical approach utilizes the avascular midline raphe, where the bilateral fascial sleeves of the erector spinae converge at the apices of the spinous processes. By incising precisely down this midline and maintaining a strict subperiosteal dissection technique, the surgeon reflects these muscle masses laterally as a single, continuous sleeve. This technique preserves the segmental innervation of the muscles, which enters from the lateral aspect, thereby preventing postoperative muscle denervation, atrophy, and subsequent junctional kyphosis or chronic axial back pain.
Neurovascular Considerations and Segmental Arterial Supply
Vigilance regarding the vascular anatomy is paramount during the lateral extent of the posterior exposure. The spinal cord receives its blood supply from the anterior spinal artery and paired posterior spinal arteries, which are fed by segmental medullary arteries. In the thoracic spine, these originate from the posterior intercostal arteries (branches of the descending aorta), and in the lumbar spine, from the segmental lumbar arteries.

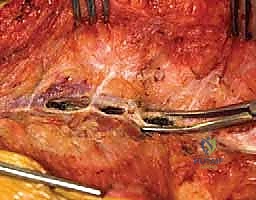
As the segmental artery courses posteriorly along the vertebral body, it sends a crucial branch through the neural foramen to supply the spinal cord. The dorsal branch then continues posteriorly to supply the paraspinal musculature. During the surgical approach, particularly as the dissection proceeds laterally over the facet joints and toward the transverse processes, these dorsal branches are highly vulnerable. They typically emerge between the transverse processes and run adjacent to the lateral aspect of the pars interarticularis.
Aggressive or careless lateral dissection, especially with monopolar electrocautery or sharp Cobb elevators, can easily avulse or transect these vessels. Bleeding from these segmental dorsal branches can be profuse and difficult to control, as the vessels tend to retract into the intertransverse space. Meticulous technique involves anticipating these vessels, utilizing bipolar electrocautery, and carefully packing the lateral gutters with laparotomy sponges to achieve hemostasis through tamponade while the exposure proceeds at adjacent levels.
Exhaustive Indications and Contraindications
The decision to proceed with posterior spinal fusion for scoliosis is a complex calculus involving the patient's chronological and skeletal age, the magnitude and progression of the deformity, the underlying etiology, and the patient's overall physiological status. The primary goals of surgery are to halt curve progression, achieve a balanced spine in both the coronal and sagittal planes, preserve as many motion segments as safely possible, and prevent long-term cardiopulmonary compromise.
Surgical intervention is rarely an emergency in the context of idiopathic scoliosis, allowing for thorough preoperative optimization. However, in cases of rapidly progressive congenital curves or severe neuromuscular deformities with impending pulmonary failure, the timing of surgery becomes critical. The surgeon must weigh the risks of major spinal reconstruction against the natural history of the untreated deformity. The indications are generally well-established, guided by decades of longitudinal outcome data.
Defining the Parameters for Surgical Intervention
For Adolescent Idiopathic Scoliosis (AIS), the classic indication for posterior spinal fusion is a curve magnitude exceeding 45 to 50 degrees in a growing child, or a curve exceeding 50 degrees in a skeletally mature patient. Curves of this magnitude have a documented natural history of continued progression into adulthood, typically at a rate of 1 to 2 degrees per year, eventually leading to severe cosmetic deformity, axial back pain, and, if the thoracic curve exceeds 80-90 degrees, restrictive pulmonary disease.
In juvenile and infantile idiopathic scoliosis, the indications are more nuanced. Bracing and serial casting are utilized to delay surgery as long as possible to allow for maximal truncal height and alveolar lung development. However, curves that progress relentlessly despite maximal conservative management, often exceeding 50 degrees, require surgical intervention, frequently utilizing growth-friendly constructs (e.g., growing rods or tethering) before a definitive posterior spinal fusion is performed near skeletal maturity.
For congenital scoliosis, prophylactic surgery is often indicated for specific anomalies with a known high risk of progression, such as a fully segmented hemivertebra or an unsegmented bar. The goal here is often a short, targeted fusion in situ or hemivertebra excision before a severe, rigid secondary compensatory curve develops. In neuromuscular scoliosis, surgery is indicated to maintain sitting balance in non-ambulatory patients, correct severe pelvic obliquity, and halt curves that are interfering with respiratory function or nursing care.
Absolute and Relative Contraindications
While the indications for surgery are broad, specific contraindications must be rigorously respected to prevent catastrophic outcomes.
| Category | Contraindication | Rationale / Clinical Consequence |
|---|---|---|
| Absolute | Active Systemic Infection or Osteomyelitis | High risk of seeding the massive hardware construct, leading to intractable deep surgical site infection requiring hardware removal. |
| Absolute | Severe, Uncorrectable Coagulopathy | The posterior exposure involves extensive decortication and muscle stripping. Uncontrolled bleeding will lead to hemorrhagic shock and death. |
| Absolute | Medically Unstable Patient | Patients with severe, unoptimized cardiopulmonary failure (e.g., severe cor pulmonale) cannot tolerate the physiological stress of prolonged prone positioning and major blood loss. |
| Relative | Extreme Skeletal Immaturity (Age < 8-10) | Definitive fusion too early results in severe truncal shortening (crankshaft phenomenon) and restricts thoracic volume, leading to thoracic insufficiency syndrome. Growth-sparing techniques are preferred. |
| Relative | Poor Soft Tissue Coverage | Previous radiation, severe scarring, or burns over the planned incision site significantly increase the risk of wound dehiscence and hardware exposure. |
| Relative | Unrecognized Intraspinal Anomaly | Performing major deformity correction in the presence of an untethered cord or severe syringomyelia carries an unacceptably high risk of irreversible neurological deficit. |
Pre-Operative Planning, Templating, and Patient Positioning
The success of a posterior spinal exposure and subsequent correction is largely dictated before the patient ever enters the operating room. Meticulous preoperative planning is the foundation of deformity surgery. This involves a comprehensive radiographic analysis to define the curve type, identify the primary and compensatory curves, determine the flexibility of the deformity, and select the appropriate upper and lower instrumented vertebrae (UIV and LIV).
The surgeon must construct a detailed mental and physical template of the planned construct. This includes selecting the type of fixation (screws vs. hooks), planning the rod contouring, and anticipating potential anatomical challenges, such as dysmorphic pedicles at the apex of the concavity. Furthermore, the positioning of the patient on the operating table is a critical operative step in itself; improper positioning can exacerbate bleeding, cause pressure necrosis, or lead to devastating peripheral nerve or brachial plexus injuries.
Radiographic Assessment and the Cobb Angle
The cornerstone of preoperative imaging is the standing high-quality posteroanterior (PA) and lateral radiograph of the entire spine on a single cassette (typically a 36-inch film). The PA radiograph is utilized to measure the Cobb angle, which quantifies the magnitude of the coronal deformity. To measure the Cobb angle, the surgeon identifies the most tilted end vertebrae at the cephalad and caudal ends of the curve. Lines are drawn parallel to the superior endplate of the cephalad vertebra and the inferior endplate of the caudal vertebra. Perpendicular lines are then drawn from these, and the intersecting angle is the Cobb angle.
Determining the distal extent of the fusion relies heavily on identifying the stable vertebra. This is assessed using the Center Sacral Vertical Line (CSVL), a vertical plumb line drawn superiorly from the exact geometric center of the S1 superior endplate. The stable vertebra is defined as the most cephalad vertebra that is bisected by the CSVL. In Lenke Type 1 (main thoracic) curves, the lower instrumented vertebra is typically chosen as the stable vertebra or one level cephalad to it, provided the disc below is horizontal and the rotation is neutral.

Assessment of skeletal maturity is equally critical, primarily evaluated via the Risser staging system on the PA radiograph. The Risser sign grades the ossification of the iliac apophysis, which progresses from anterolateral to posteromedial. Risser 0 indicates no ossification (high growth potential), while Risser 5 indicates complete fusion of the apophysis to the ilium (skeletal maturity). This staging helps predict the risk of curve progression and informs the timing of surgical intervention.
Advanced Imaging Modalities and Preoperative MRI
While standing radiographs provide the static architectural blueprint, dynamic imaging is essential to assess curve flexibility. Supine lateral side-bending radiographs are the gold standard for differentiating between structural (inflexible) and non-structural (flexible compensatory) curves. A structural curve is typically defined as one that fails to correct to less than 25 degrees on maximal side-bending efforts. In severe, rigid deformities (e.g., >80 degrees), supine traction radiographs under general anesthesia or halo-gravity traction may provide a more accurate assessment of true flexibility than active side-bending.
Magnetic Resonance Imaging (MRI) of the entire neural axis is mandatory in specific clinical scenarios to rule out neuroaxis abnormalities such as Chiari malformations, syringomyelia, tethered cord syndrome, or diastematomyelia. Routine MRI is indicated for patients with early-onset scoliosis (age < 10 years), atypical curve patterns (e.g., left thoracic curves, which are highly suspicious for syrinx), rapid curve progression, severe pain, abnormal neurological examination findings (e.g., asymmetric abdominal reflexes, cavus feet), or any cutaneous stigmata of dysraphism.

Operating Room Setup and Patient Positioning
Patient positioning is a meticulous process that requires the coordinated effort of the surgical, anesthesia, and nursing teams. Following induction of general anesthesia and intubation on the transport stretcher, neuromonitoring baseline signals (Somatosensory Evoked Potentials - SSEPs, and Motor Evoked Potentials - MEPs) are obtained. The patient is then carefully log-rolled onto the operating table. An open Jackson frame or a specialized radiolucent spinal table with individual chest and hip pads is strongly preferred.

The primary goal of prone positioning on a Jackson frame is to allow the abdomen to hang completely free. Any external compression on the abdomen increases intra-abdominal pressure, which is directly transmitted to the inferior vena cava. This venous hypertension forces blood to bypass the IVC and return to the heart via the valveless epidural venous plexus (Batson's plexus). Engorgement of Batson's plexus leads to catastrophic, uncontrollable epidural bleeding during the surgical exposure and decompression.
All bony prominences must be meticulously padded. The arms are typically positioned on arm boards in a "superman" position, ensuring the shoulders are abducted less than 90 degrees and forward flexed less than 90 degrees to prevent traction injuries to the brachial plexus. The breasts in females and genitalia in males must be checked to ensure they are free from compression. Finally, the table is adjusted to optimize sagittal alignment; slight hip extension can be used to induce lumbar lordosis, while hip flexion can reduce it, depending on the specific goals of the reconstruction.

Step-by-Step Surgical Approach and Fixation Technique
The execution of the posterior spinal exposure demands a rhythmic, methodical approach. The surgeon must balance the need for speed—to minimize blood loss and operative time—with the absolute requirement for meticulous hemostasis and anatomical precision. The exposure is typically performed sequentially, exposing a few levels at a time, packing them with sponges for hemostasis, and moving to the next segment.
A poorly executed exposure, characterized by wandering off the midline, violating the muscle bellies, or aggressively avulsing segmental vessels, will transform a routine deformity correction into a bloody, chaotic struggle. Conversely, a masterfully executed subperiosteal dissection provides a pristine, bloodless field where the intricate bony anatomy is clearly delineated, facilitating rapid and accurate pedicle screw placement and ensuring a massive surface area for the fusion mass.
Incision Strategy and Subcutaneous Dissection
Following rigorous skin preparation and sterile draping, the planned incision is marked, utilizing fluoroscopy to confirm the upper and lower instrumented vertebrae. The skin is infiltrated with a dilute epinephrine solution (e.g., 1:500,000) to minimize dermal bleeding. A straight midline longitudinal incision is made with a scalpel, extending precisely from the spinous process of the UIV to the spinous process of the LIV.

The subcutaneous tissue is sharply divided down to the glistening white thoracolumbar fascia. It is critical to maintain the dissection strictly in the midline avascular plane. Wandering laterally into the subcutaneous fat will result in unnecessary bleeding and create dead space that predisposes the patient to postoperative seroma or hematoma formation. Self-retaining retractors (e.g., Weitlaner or Cerebellar retractors) are placed to maintain tension on the tissues, aiding in the identification of the true midline raphe.

Subperiosteal Exposure of the Posterior Elements
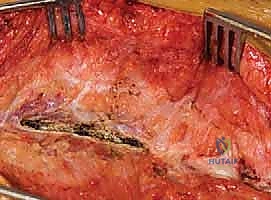
The thoracolumbar fascia and the cartilaginous apophyses of the spinous processes are incised longitudinally using needle-tip electrocautery. The subperiosteal dissection begins at the lowest level of the planned construct and proceeds cephalad. Using a Cobb elevator and electrocautery, the paraspinal muscles are stripped from the spinous processes and laminae. The key to a bloodless exposure is staying strictly beneath the periosteum. The Cobb elevator should scrape firmly against the bone, peeling the periosteum and attached muscle fibers as a single contiguous sheet.

As the dissection proceeds laterally over the facet joints, the surgeon must be acutely aware of the altered anatomy dictated by the scoliotic rotation. On the convex side, the transverse processes are prominent and superficial. On the concave side, they are deeply recessed. The dissection must extend laterally to the tips of the transverse processes in the thoracic spine and to the base of the transverse processes/pars interarticularis in the lumbar spine to provide adequate exposure for pedicle screw entry points and the posterolateral fusion bed.
During this lateral exposure, the segmental vessels (dorsal branches) will be encountered as they emerge between the transverse processes. These must be anticipated and meticulously coagulated with bipolar electrocautery before they are torn by the Cobb elevator. Once a segment is exposed, a radiopaque laparotomy sponge is tightly packed into the lateral gutter to provide hemostatic tamponade while the surgeon moves to the contralateral side or the next cephalad level.
Facetectomy and Preparation for Arthrodesis
Once the entire spine is exposed and hemostasis is achieved, the self-retaining retractors are repositioned deep within the muscle mass to provide wide, unobstructed visualization. The next critical step is the preparation of the fusion bed, which begins with meticulous facetectomies. Complete excision of the facet joint cartilage is mandatory for achieving a solid posterior arthrodesis.
Using a combination of osteotomes, rongeurs (Leksell or Kerrison), and high-speed burrs, the inferior articular process of the cephalad vertebra and the superior articular process of the caudal vertebra are aggressively decorticated. The articular cartilage is completely removed down to bleeding cancellous bone. In the thoracic spine, complete facetectomies also significantly increase the flexibility of the spine, facilitating easier deformity correction during rod reduction.

Crucially, the facet capsules at the upper and lower extremes of the planned fusion construct (the UIV+1 and LIV-1 levels) must be meticulously preserved. Violating the capsule of an adjacent, unfused segment will inevitably lead to accelerated adjacent segment degeneration, instability, and the potential need for future extension of the fusion. Following facetectomy, the entire posterior bony surface (laminae, spinous processes, and transverse processes) is aggressively decorticated to create a massive, bleeding bed of host bone, ready to receive the autograft and allograft bone matrix.
Complications, Incidence Rates, and Salvage Management
Despite meticulous technique
