Mastering Lumbar Interbody Fusion: TLIF & PLIF Techniques
Key Takeaway
This masterclass guides fellows through Transforaminal (TLIF) and Posterior (PLIF) Lumbar Interbody Fusion. We cover intricate surgical anatomy, detailed preoperative planning, and granular, real-time intraoperative execution. Learn precise instrument use, critical nerve root protection, and techniques for optimal fusion. Understand pearls, pitfalls, and comprehensive postoperative management to master these versatile spinal procedures.
Comprehensive Introduction and Patho-Epidemiology
The evolution of lumbar arthrodesis represents one of the most significant advancements in modern orthopedic spine surgery. Historically, posterolateral fusion (PLF) relying on intertransverse bone grafting was the gold standard for stabilizing the degenerated or unstable lumbar spine. However, the biomechanical limitations of isolated posterior column support—namely, the susceptibility to cantilever failure, pseudarthrosis, and inability to reliably restore sagittal alignment—necessitated a more robust, multidimensional approach. Enter the era of lumbar interbody fusion, specifically the Posterior Lumbar Interbody Fusion (PLIF) and its refined variant, the Transforaminal Lumbar Interbody Fusion (TLIF). These techniques have fundamentally shifted the paradigm, offering surgeons the ability to achieve circumferential (360-degree) arthrodesis through a single posterior approach, addressing pathology in the anterior, middle, and posterior columns simultaneously.
The epidemiological burden of lumbar spinal pathology is staggering, with degenerative disc disease, spondylolisthesis, and adult spinal deformity representing a massive proportion of global healthcare expenditure. As the population ages, the incidence of these conditions continues to rise, demanding surgical interventions that offer high fusion rates, durable clinical outcomes, and acceptable morbidity profiles. PLIF and TLIF have emerged as the workhorses of the spine surgeon's armamentarium to meet this demand. By replacing the degenerated intervertebral disc with a structural strut graft or cage, these procedures directly eliminate the discogenic pain generator, restore intervertebral height, indirectly decompress the neural foramina, and provide immediate anterior column load-sharing.

While the standard posterior midline approach serves as the gateway for both techniques, the critical distinction lies in the trajectory to the interbody space and the management of the neural elements. PLIF, pioneered by Cloward in the 1950s, utilizes a bilateral, medial approach. This necessitates significant bilateral retraction of the thecal sac and traversing nerve roots to safely access the disc space and insert dual cages. While highly effective for achieving fusion and direct bilateral decompression, the requisite neural retraction inherently increases the risk of iatrogenic neurapraxia, dural tears, and epidural fibrosis.
In contrast, the TLIF technique, popularized by Harms and Rolinger in the 1980s, utilizes a unilateral, transforaminal trajectory. By performing a unilateral facetectomy, the surgeon gains access to the disc space via a more lateral corridor. This ingenious modification allows for the insertion of a single, large interbody device while dramatically minimizing, and often eliminating, the need for medial retraction of the thecal sac and traversing root. The TLIF approach leverages the natural anatomical window between the exiting and traversing nerve roots, significantly enhancing the safety profile regarding neurologic injury while still delivering the biomechanical advantages of an interbody fusion.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of lumbar surgical anatomy is the absolute prerequisite for safely executing PLIF and TLIF procedures. The transition from the posterior muscular envelope to the intricate neurovascular topography of the spinal canal and neuroforamen requires meticulous dissection and unwavering spatial awareness.
Muscular Intervals and Posterior Exposure
The surgical journey commences with the standard posterior midline incision, centered over the spinous processes of the target levels. The initial dissection involves the subperiosteal elevation of the paraspinal musculature—comprising the multifidus, longissimus, and iliocostalis muscles of the erector spinae group. This elevation must be performed meticulously using Cobb elevators or electrocautery, staying strictly subperiosteal to minimize intramuscular bleeding, denervation, and subsequent ischemic necrosis. For a standard PLIF or TLIF combined with posterolateral fusion, the exposure is carried laterally to the tips of the transverse processes, exposing the pars interarticularis and the facet joint complexes.
However, the modern spine surgeon must also be cognizant of the iatrogenic morbidity associated with extensive muscle stripping. The multifidus muscle, in particular, is a critical dynamic stabilizer of the lumbar spine. Extensive retraction can lead to "fusion disease" or intractable postoperative axial back pain due to muscle atrophy and fatty infiltration. Consequently, many surgeons now advocate for utilizing a Wiltse paraspinal muscle-splitting approach for pedicle screw placement or minimally invasive (MIS) TLIF variations. The Wiltse interval, a natural cleavage plane between the multifidus medially and the longissimus laterally, provides direct access to the facet joint and transverse process with minimal muscle disruption, preserving the neurovascular supply to the medial muscular columns.
Regardless of the approach (open vs. MIS), achieving meticulous hemostasis of the muscular and osseous bleeding is paramount. The segmental arteries, which give rise to the posterior branches supplying the paraspinal muscles and osseous structures, must be respected. Aggressive lateral dissection beyond the transverse processes risks injury to these vessels, leading to significant hemorrhage. Furthermore, maintaining a clean, dry surgical field is not merely a matter of convenience; it is essential for the accurate identification of the delicate neural elements and the safe execution of the decompression and interbody preparation phases.
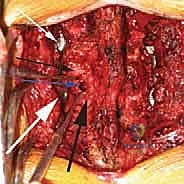
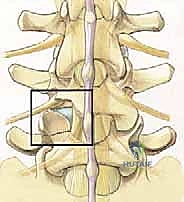
The Triangular Working Window and Neurovascular Topography
Accessing the interbody space safely requires navigating the "triangular working window," a critical anatomical concept analogous to Kambin's triangle but viewed from a direct posterior or posterolateral trajectory. This window represents the maximum safe corridor for instrument insertion and cage delivery without compromising the neural elements.
The medial border of this window is defined by the traversing nerve root and the lateral margin of the thecal sac. During a PLIF, these structures must be actively retracted medially, placing them under tension. During a TLIF, the medial border remains the traversing root, but the lateral trajectory reduces the need for active retraction. The lateral border of the window is formed by the exiting nerve root of the proximal vertebral level (e.g., the L4 root at the L4-L5 disc space), which courses inferolaterally beneath the pedicle. The base of the triangle is the superior aspect of the pedicle of the distal vertebra (e.g., the L5 pedicle at L4-L5).

Navigating this window is complicated by the presence of the epidural venous plexus (Batson's plexus). These thin-walled, valveless veins form a rich network surrounding the thecal sac and nerve roots, particularly concentrated in the anterior epidural space and the neuroforamina. Unintentional laceration of these veins during the initial annulotomy or lateral recess decompression can result in profuse, obscuring hemorrhage. Bipolar electrocautery, hemostatic matrix agents (e.g., Floseal, Surgiflo), and cottonoid pledgets are essential tools for managing this venous bleeding. Furthermore, the surgeon must remain vigilant for anatomical anomalies, such as conjoined nerve roots, which drastically alter the dimensions of the working window and significantly increase the risk of iatrogenic injury during retraction or cage insertion.
Osteology, Disc Space Dimensions, and Endplate Preparation
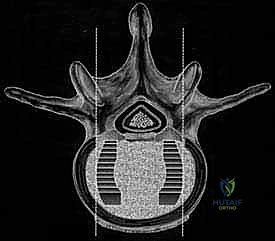
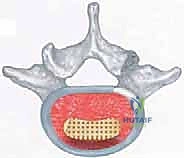
The osteological architecture of the lumbar motion segment dictates the biomechanical success of the fusion. The pedicles, robust cylinders of cortical bone with a cancellous core, serve as the foundational anchors for posterior instrumentation. Their entry points are reliably identified at the intersection of the pars interarticularis, the superior articular process, and the transverse process. The vertebral bodies themselves are designed to withstand massive compressive loads. The superior and inferior endplates, however, are not uniform structures. The peripheral apophyseal ring consists of dense, strong cortical bone, while the central endplate is thinner and overlies highly vascular cancellous bone.

A healthy adult lumbar disc space typically measures 12 to 14 mm in height and approximately 35 mm in anteroposterior diameter. When performing an interbody fusion, the goal is to restore this anatomical height to achieve indirect foraminal decompression and restore regional lordosis. However, the preparation of the endplates is perhaps the most critical, yet technically demanding, step of the entire procedure. The surgeon must meticulously remove the cartilaginous endplate to expose the underlying bleeding subchondral bone, creating an optimal biological milieu for osteogenesis.
If the subchondral bone is aggressively violated or removed (decortication that is too deep), the structural integrity of the endplate is compromised. This dramatically increases the risk of cage subsidence—where the interbody device sinks into the softer cancellous bone of the vertebral body. Subsidence leads to a loss of the restored disc height, recurrent foraminal stenosis, loss of lordosis, and ultimately, biomechanical failure and pseudarthrosis. Therefore, endplate preparation must be aggressive enough to stimulate bleeding but delicate enough to preserve the structural subchondral bone, a balance that requires significant surgical experience and tactile feedback.
Exhaustive Indications and Contraindications
Patient selection is the cornerstone of successful spine surgery. While PLIF and TLIF are powerful techniques, they are not panaceas for all lumbar pathologies. A rigorous evaluation of indications and contraindications is mandatory to optimize clinical outcomes and minimize the risk of failed back surgery syndrome.
Rationale for Interbody Fusion
The decision to add an interbody fusion to a posterior decompression and instrumentation construct is driven by several biomechanical and biological imperatives. First, the anterior column bears approximately 80% of the axial compressive load of the spine. Placing a structural graft in the interbody space directly shares this load, significantly reducing the cantilever bending forces exerted on the posterior pedicle screws and rods. This load-sharing phenomenon drastically lowers the risk of hardware failure (screw breakage or pullout) and creates a compressive environment highly conducive to bone healing, in accordance with Wolff's Law.
Furthermore, interbody fusion addresses the discogenic pain generator directly by performing a complete discectomy. In cases of severe disc degeneration or internal disc disruption, isolated posterior fusions often fail to alleviate axial back pain because the diseased disc continues to micro-motion and generate nociceptive signals. By excising the disc and fusing the space, this source of pain is eliminated. Additionally, the insertion of an appropriately sized interbody cage restores disc height, which tightens the redundant ligamentum flavum and posterior longitudinal ligament, effectively providing indirect decompression of the neural foramina without necessarily requiring aggressive bony resection of the pars or facets.
Patient Selection Criteria
The ideal candidate for a PLIF or TLIF presents with structural instability or deformity coupled with neurologic compression or intractable discogenic pain. Degenerative spondylolisthesis (Grade I or II) with concurrent central or foraminal stenosis is a classic indication. The interbody graft allows for the reduction of the slip, restoration of lordosis, and robust anterior column support to prevent recurrence. Similarly, in cases of recurrent disc herniation where a wide laminectomy and facetectomy are required for safe revision decompression, the resulting iatrogenic instability mandates a fusion, and the interbody route is highly favored.
Pseudarthrosis (failed prior fusion) is another strong indication. If a posterolateral fusion has failed, the posterior bony bed is often scarred, hypovascular, and biologically depleted. Approaching the anterior column via a PLIF or TLIF provides access to a virgin, highly vascularized fusion bed (the vertebral endplates), significantly increasing the likelihood of a successful salvage arthrodesis. Furthermore, TLIF and PLIF are invaluable tools in the correction of adult degenerative scoliosis, allowing for asymmetric disc space distraction to correct coronal plane deformities and the induction of lordosis to correct sagittal imbalance.
| Indication Category | Specific Pathologies | Rationale for PLIF/TLIF |
|---|---|---|
| Instability | Degenerative Spondylolisthesis, Isthmic Spondylolisthesis, Iatrogenic Instability | Provides immediate 3-column stabilization, allows for reduction of deformity, and prevents progression. |
| Discogenic Pain | Severe Degenerative Disc Disease, Internal Disc Disruption, Modic Changes | Directly removes the nociceptive source (the diseased disc) and immobilizes the painful segment. |
| Deformity | Adult Degenerative Scoliosis, Flatback Syndrome, Sagittal Imbalance | Allows for anterior column lengthening, restoration of lumbar lordosis, and coronal plane correction. |
| Revision Surgery | Pseudarthrosis (Failed Posterior Fusion), Recurrent Disc Herniation | Provides a fresh, vascularized fusion bed (endplates) when the posterior elements are compromised or absent. |
| Contraindication Category | Specific Conditions | Rationale / Alternative |
|---|---|---|
| Absolute | Active Spinal Infection (Osteomyelitis/Discitis) | Hardware placement in an actively infected field is contraindicated. Requires debridement and antibiotics first. |
| Absolute | Severe Osteoporosis (T-score < -2.5) | Extremely high risk of cage subsidence and pedicle screw pullout. Requires medical optimization prior to surgery. |
| Relative | Conjoined Nerve Root (on approach side) | Drastically increases the risk of iatrogenic nerve injury during retraction for cage insertion. Consider contralateral TLIF or ALIF. |
| Relative | Extensive Epidural Fibrosis | Increases the risk of dural tears and nerve root injury during mobilization. ALIF or LLIF may be safer alternatives. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the invisible foundation upon which surgical success is built. It requires a comprehensive synthesis of clinical examination findings, advanced neuroimaging, and precise biomechanical templating.
Advanced Imaging and Implant Templating
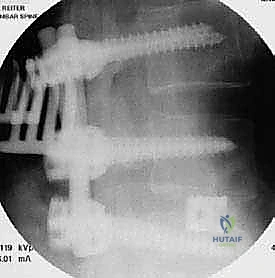
Standard evaluation begins with dynamic (flexion-extension) and standing orthogonal radiographs of the lumbar spine to assess gross instability, spondylolisthesis, and global spinopelvic parameters. Calculating the Pelvic Incidence (PI), Lumbar Lordosis (LL), and Pelvic Tilt (PT) is mandatory. The surgical goal is to achieve a PI-LL mismatch of less than 10 degrees to ensure harmonious sagittal balance. Failure to restore appropriate lordosis at the fused levels, particularly at L4-L5 and L5-S1, will inevitably lead to adjacent segment disease and sagittal decompensation.
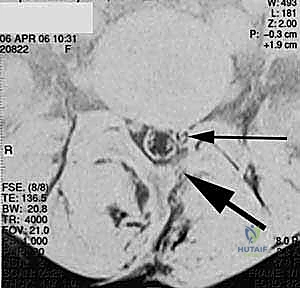
Magnetic Resonance Imaging (MRI) is the gold standard for evaluating the neural elements, assessing the degree of central, lateral recess, and foraminal stenosis, and evaluating disc hydration and Modic changes. Crucially, the MRI must be scrutinized for the presence of anatomical variants, such as conjoined nerve roots or synovial cysts, which dictate the surgical approach (e.g., choosing a right-sided TLIF to avoid a left-sided conjoined root).

Computed Tomography (CT) is invaluable for assessing bony anatomy. It provides high-resolution detail of the facet joints, pars interarticularis, and pedicle morphology. CT is essential for templating pedicle screw trajectories and diameters, particularly in cases of severe rotation or dysplastic pedicles. Furthermore, CT accurately assesses the presence of endplate sclerosis or large osteophytes that may complicate cage insertion or require aggressive intraoperative resection.
Anesthesia, Neuromonitoring, and Patient Positioning
PLIF and TLIF are performed under general endotracheal anesthesia. The utilization of intraoperative neuromonitoring (IONM)—including Somatosensory Evoked Potentials (SSEPs), Motor Evoked Potentials (MEPs), and spontaneous/triggered Electromyography (EMG)—has become standard of care in many institutions. IONM provides real-time feedback on the functional integrity of the spinal cord and nerve roots during critical steps such as pedicle screw placement, neural retraction, and cage insertion, allowing the surgeon to immediately alter their technique if impending neurologic injury is detected.
Patient positioning is a critical, yet often underappreciated, aspect of the procedure. The patient is typically positioned prone on a specialized radiolucent spine table, such as a Jackson table or an Andrews frame. The abdomen must hang completely free to prevent compression of the inferior vena cava. Abdominal compression increases venous pressure, which is directly transmitted to the epidural venous plexus (Batson's plexus), resulting in profuse, difficult-to-control intraoperative bleeding that obscures the surgical field.
Furthermore, positioning dictates the resting alignment of the spine. Using a Wilson frame, which flexes the lumbar spine, opens the posterior elements and facilitates decompression, but it artificially reduces lumbar lordosis. If pedicle screws and rods are locked in this flexed position, the patient will be fused in a flatback deformity. Therefore, if a Wilson frame is used, it must be cranked down (flattened) prior to final rod tightening to induce lordosis. Conversely, an open Jackson table inherently promotes lordosis, making it the preferred choice for deformity correction and multi-level fusions where restoring sagittal balance is paramount.
Step-by-Step Surgical Approach and Fixation Technique
The execution of a PLIF or TLIF is a highly choreographed sequence of anatomical dissection, neural decompression, meticulous endplate preparation, and rigid biomechanical fixation.
Soft Tissue Dissection and Bony Exposure
Following the standard midline incision and subperiosteal dissection of the paraspinal muscles, self-retaining retractors (e.g., cerebellar or specialized hinged retractors) are deployed to maintain exposure. The exposure must clearly define the spinous processes, laminae, facet joints, and transverse processes of the target levels. Meticulous hemostasis of the muscle bed is achieved using bipolar electrocautery.
At this stage, anatomical landmarks are verified, often utilizing intraoperative fluoroscopy to confirm the correct surgical level. The pars interarticularis is identified, and the joint capsule of the facet complex is excised using a Bovie or a specialized rongeur. Clear visualization of the bony anatomy is crucial before proceeding with any bone removal.
Decompression and Facetectomy (PLIF vs. TLIF)
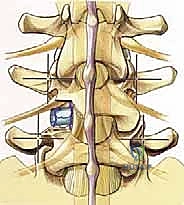
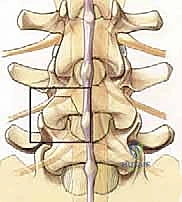
The decompression phase diverges significantly depending on whether a PLIF or TLIF is being performed. For a PLIF, a wide bilateral laminectomy and bilateral medial facetectomies are typically performed. The spinous process and interspinous ligaments are removed. A high-speed burr or Leksell rongeur is used to thin the lamina, followed by Kerrison rongeurs to remove the ligamentum flavum and expose the underlying thecal sac and bilateral traversing nerve roots. The medial aspect of the inferior articular process (IAP) and superior articular process (SAP) are resected to decompress the lateral recess and provide bilateral access to the disc space.
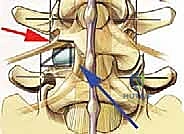
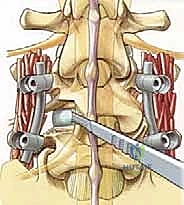
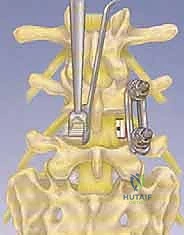
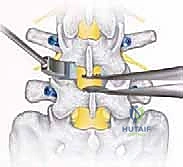
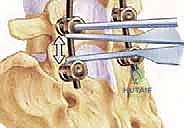
For a TLIF, the approach is unilateral and transforaminal. The surgeon selects the side of approach based on the patient's predominant radicular symptoms or the side of the most severe pathology. A unilateral complete facetectomy is performed. The IAP of the superior vertebra is removed, typically using an osteotome or a high-speed burr, exposing the underlying SAP of the inferior vertebra.
The SAP is then resected down to the level of the pedicle. This complete removal of the facet joint complex unroofs the neural foramen and exposes the lateral aspect of the ligamentum flavum. Resection of this lateral flavum reveals the exiting nerve root superiorly and the traversing nerve root medially. This creates the critical lateral corridor to the disc space, minimizing the need for medial retraction of the thecal sac.
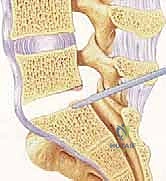
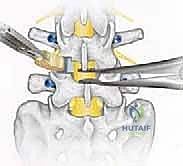
Disc Preparation and Endplate Decortication
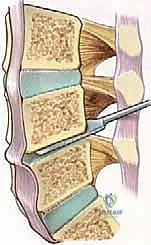
Once the posterior annulus is exposed, epidural veins are coagulated with bipolar cautery. A box annulotomy is performed using a long-handled scalpel (e.g.,
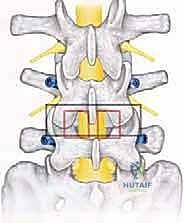
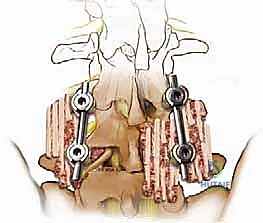
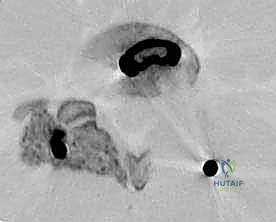
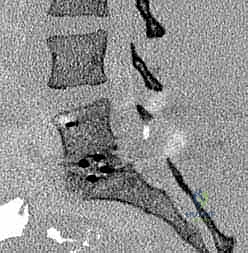
Clinical & Radiographic Imaging Archive