Thoracolumbar Spine Injuries: A Comprehensive Guide to Diagnosis, Surgical Anatomy, & Management Decisions
Key Takeaway
Surgical intervention for thoracolumbar spine injuries is typically indicated for unstable fractures requiring decompression of neural elements, restoration of spinal alignment, and stable fixation. Key factors include fracture morphology, neurological status, and especially disruption of the posterior ligamentous complex (PLC), which signifies mechanical instability predisposing to neurological deterioration and progressive kyphosis.
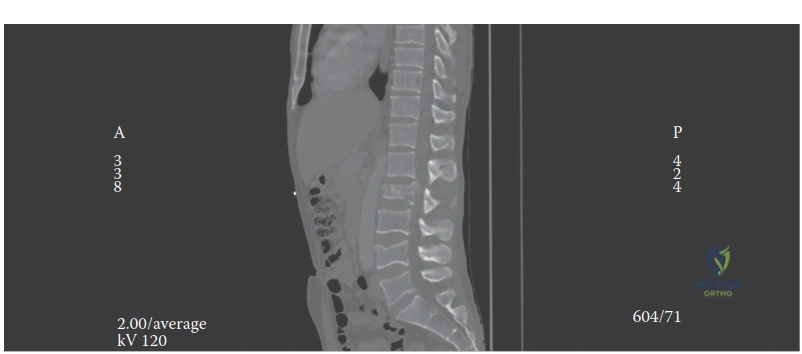
A 25-year-old male presents to the Emergency Department following a high-energy motorcycle accident. He complains of severe back pain. On neurological examination, he has preserved motor and sensory function in the lower extremities. You are provided with this imaging.
How do you approach the clinical assessment and classification of this injury to guide your management decision?
Candidate: I would start by stabilizing the patient using ATLS protocols. Clinically, I'll assess for neurological deficits. Radiographically, I need a CT scan to look at the fracture morphology, specifically the three columns described by Denis. I would then use the TLICS score to decide between surgery and non-operative management, and if it's a burst fracture, I’d check the McCormack Load-Sharing score to decide if I need anterior column support.
Failing to mention the integrity of the Posterior Ligamentous Complex (PLC). Candidates often focus only on the vertebral body (anterior/middle columns) and forget that MRI is the gold standard for evaluating the PLC, which is a major driver of the TLICS score and surgical decision-making.
A systematic approach: 1. Clinical: Confirm stability and perform a thorough neurological exam, noting the level of the conus (T12-L2). 2. Imaging: CT for bony morphology and sagittal/coronal alignment. MRI to evaluate the PLC, cord signal, and disc integrity. 3. Classification: Utilize the TLICS (Morphology + PLC status + Neuro status) and AOSpine systems. 4. Decision: If surgery is required, apply the Load-Sharing Classification. If score > 6, prioritize anterior column support (corpectomy) or long-segment posterior fixation to prevent hardware failure.
During your assessment of a complex burst fracture, you determine the patient needs surgical stabilization. You decide on a posterior approach. How do you assess the risk of hardware failure, and what technical steps can you take to mitigate this?
Candidate: Hardware failure risk is high if the anterior column is severely comminuted. I would use the McCormack Load-Sharing score. To mitigate failure, I can increase the length of the construct by instrumenting more levels, use transpedicular bone grafting, or, if the Load-Sharing score is too high, consider an anterior corpectomy and cage reconstruction.
Ignoring the biomechanics of the "index" level. Candidates often forget to mention "in-situ" fusion or the importance of screw placement at the fracture level to improve the rigidity of the construct, or failing to mention the role of patient positioning (Jackson table) in achieving postural reduction before instrumentation.
The candidate should explicitly state the three variables of the McCormack Load-Sharing Score (comminution, fragment apposition, and deformity correction). To mitigate failure: 1. Construct length: Extend fixation to levels above and below if the anterior column is deficient. 2. Pedicle screws: Utilize screws at the level of the fracture if morphology allows. 3. Alignment: Achieve stable, sagittal correction through cantilever or ligamentotaxis. 4. Support: If the anterior column is incompetent, add structural support rather than relying on a short-segment posterior construct.
