Spondylolysis and Spondylolisthesis: Comprehensive Surgical Management
Key Takeaway
Spondylolisthesis involves the anterior or posterior translation of one spinal segment over another, often secondary to a pars interarticularis defect or dysplastic anatomy. This comprehensive guide details the biomechanical etiology, advanced radiographic evaluation, and step-by-step surgical management of developmental and acquired spondylolisthesis. Emphasizing evidence-based techniques, it covers decompression, instrumentation, and fusion strategies essential for orthopedic residents and practicing spine surgeons.
Comprehensive Introduction and Patho-Epidemiology
The anatomical anomaly of spondylolisthesis was first noted by Herbiniaux, a Belgian obstetrician, who observed a bony prominence anterior to the sacrum that obstructed the birth canal and complicated delivery. He is widely credited with the first clinical description of the condition. The formal medical terminology, however, was coined by Kilian in 1854. The term spondylolisthesis is derived from the Greek spondylos (meaning "vertebra") and olisthenein (meaning "to slip"). Clinically, spondylolisthesis is defined as the anterior or posterior translation of one segment of the spine over the adjacent lower segment. While the condition can occur anywhere in the spine, it is overwhelmingly most common at the L5-S1 junction, followed by L4-L5. Understanding the intricate biomechanics, natural history, and precise surgical indications is paramount for the practicing orthopedic surgeon and neurosurgeon.
The prevalence of spondylolisthesis in the general population is approximately 5%, with an equal distribution between men and women. However, distinct genetic and biomechanical factors drive its development. Developmental spondylolisthesis with lysis typically manifests as a stress fracture in children possessing a genetic predisposition. Notably, the defect is virtually never present at birth and is absent in chronically bedridden patients, strongly indicating an acquired mechanical etiology superimposed on genetic susceptibility. Epidemiological data strongly supports a genetic link: up to 50% of Inuit populations possess spondylolisthesis, compared to only 6% to 7% of Caucasian males and 1.1% of African American females. The condition is also disproportionately prevalent in adolescent athletes subjected to repetitive hyperextension, such as female gymnasts, interior linemen in American football, and fast bowlers in cricket.
The natural history of untreated spondylolysis and low-grade spondylolisthesis is overwhelmingly benign. Beutler et al. conducted a landmark 50-year prospective study (initiated by Dr. Daniel Baker) following 500 first-grade children. Initially, 4.4% exhibited a lytic pars defect, which increased to 6% by adulthood. Key findings from the Beutler study include: subjects with unilateral defects never experienced slippage; progression of slippage slowed significantly with each advancing decade; there was no statistical correlation between slip progression and the incidence of low back pain; and SF-36 health survey scores of the study cohort were indistinguishable from the general population. If slip progression is to occur, it almost exclusively happens during the adolescent growth spurt (ages 9 to 15) and is exceedingly rare after age 20.
Accurate classification is essential for determining prognosis and guiding surgical intervention. Historically, the Wiltse, Newman, and Macnab Classification was the most widely utilized system, categorizing the condition into five distinct types based on etiology: Type I (Dysplastic), Type II (Isthmic, including lytic, elongated, and acute fracture subtypes), Type III (Degenerative), Type IV (Traumatic), and Type V (Pathological). However, Marchetti and Bartolozzi criticized the Wiltse system for mixing etiological and topographical criteria, arguing it failed to accurately predict progression or surgical response. They proposed a system emphasizing the degree of dysplasia, dividing patients into Developmental (High Dysplastic vs. Low Dysplastic) and Acquired (Traumatic, Postsurgery, Pathological, Degenerative). When evaluating a patient, the surgeon must first differentiate developmental from acquired. High dysplastic slips are inherently unstable and require more aggressive, heavily instrumented surgical stabilization.
Detailed Surgical Anatomy and Biomechanics
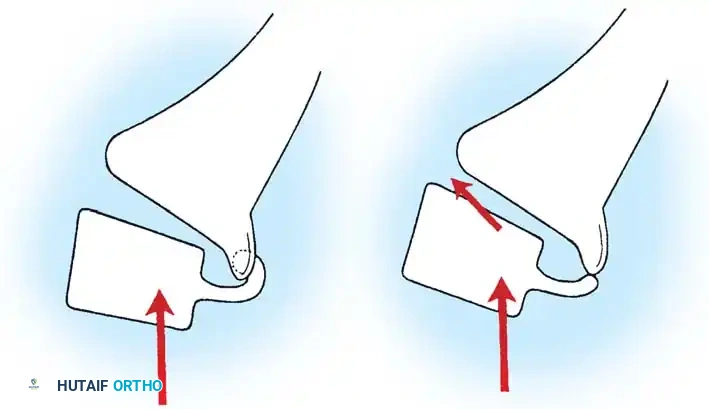
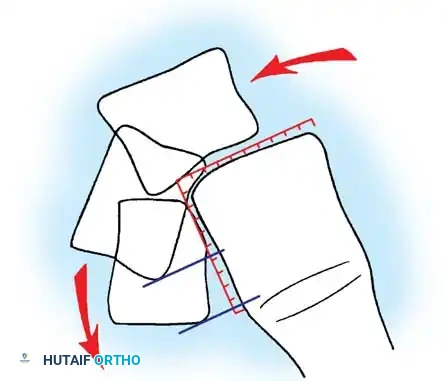
The stability of the lumbosacral junction relies heavily on the integrity of the posterior osseous and ligamentous complex. The critical anatomical structure preventing anterior translation of L5 over S1 is the "bony hook." The bony hook is comprised of the pedicle, the pars interarticularis, the inferior articular facets of L5, and the superior articular facets of the sacrum. In a normal spine, this hook effectively resists the anterior shear forces generated by the lumbar lordosis and the sacral slope. When a defect occurs in the pars interarticularis (spondylolysis), the posterior elements are uncoupled from the anterior vertebral body, rendering the bony hook incompetent and allowing anterior translation under physiological loads.
The degree of lumbar lordosis and the position of the sagittal gravity line are critical predictors of slip progression. The further anterior the gravity line falls relative to the sacral promontory, the higher the shear forces acting on the pars interarticularis, increasing the likelihood of progressive spondylolisthesis. Wiltse et al. postulated that the normal flexion contractures of the hip in early childhood accentuate lumbar lordosis, thereby concentrating weight-bearing and shear forces directly onto the pars interarticularis. Letts et al. further demonstrated that shear stresses on the pars are maximized during lumbar extension. Cyron and Hutton's biomechanical studies revealed that the pars interarticularis is structurally thinner, and the intervertebral disc less resistant to shear, in children and adolescents compared to adults.
Furthermore, the competency of the intervertebral disc at the affected level plays a vital role in resisting shear. Early disc degeneration or failure exacerbates instability. The intervertebral disc acts as the primary anterior column restraint against translation once the posterior bony hook fails. As the disc undergoes desiccation and loss of proteoglycan content, its viscoelastic properties diminish, leading to a loss of disc height and an increase in translational micromotion. This micromotion accelerates facet arthropathy and further destabilizes the functional spinal unit. Magnetic Resonance Imaging (MRI) is often required to accurately assess disc hydration and structural integrity, guiding the surgeon in deciding whether an interbody fusion is necessary to restore anterior column support.
Spinopelvic parameters are deeply intertwined with the biomechanics of spondylolisthesis. Pelvic Incidence (PI), a fixed morphological parameter, dictates the individual's required lumbar lordosis. Patients with a high PI require a proportionally high Sacral Slope (SS) and Lumbar Lordosis (LL) to maintain sagittal balance. This high SS creates a steep lumbosacral angle, dramatically increasing the anterior shear forces at L5-S1. Conversely, Pelvic Tilt (PT) is a compensatory parameter; as L5 slips anteriorly, the patient retroverts the pelvis (increasing PT) to keep the center of gravity over the femoral heads. Recognizing these biomechanical relationships is crucial, as surgical correction must aim not only to stabilize the slip but also to restore harmonious spinopelvic alignment to prevent adjacent segment disease.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention for spondylolysis and spondylolisthesis is multifaceted, relying on patient age, slip grade, symptom duration, and the presence of neurological deficits. Conservative management—encompassing activity modification, non-steroidal anti-inflammatory drugs (NSAIDs), targeted physical therapy focusing on core stabilization and hamstring flexibility, and rigid antilordotic bracing—remains the first line of treatment for symptomatic low-grade slips. However, when conservative measures fail to provide durable relief, or when the natural history dictates a high likelihood of catastrophic progression, surgical stabilization becomes imperative.
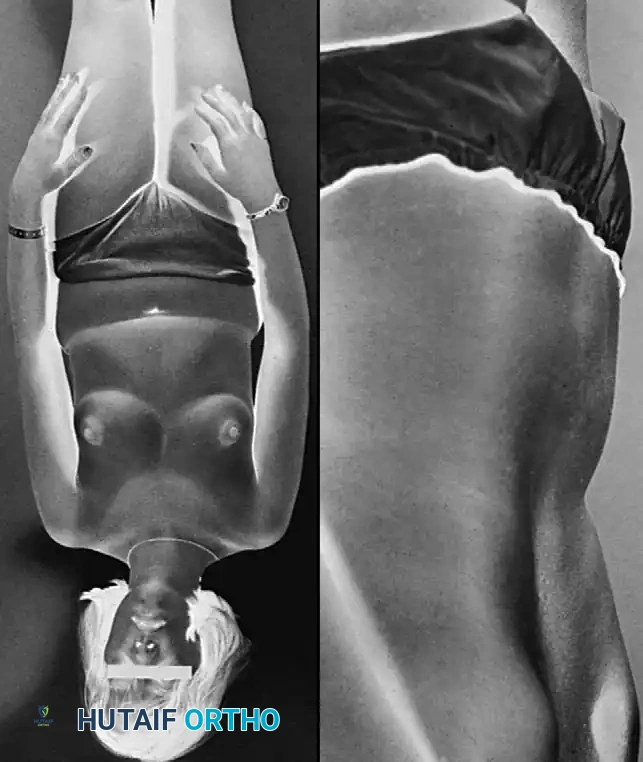
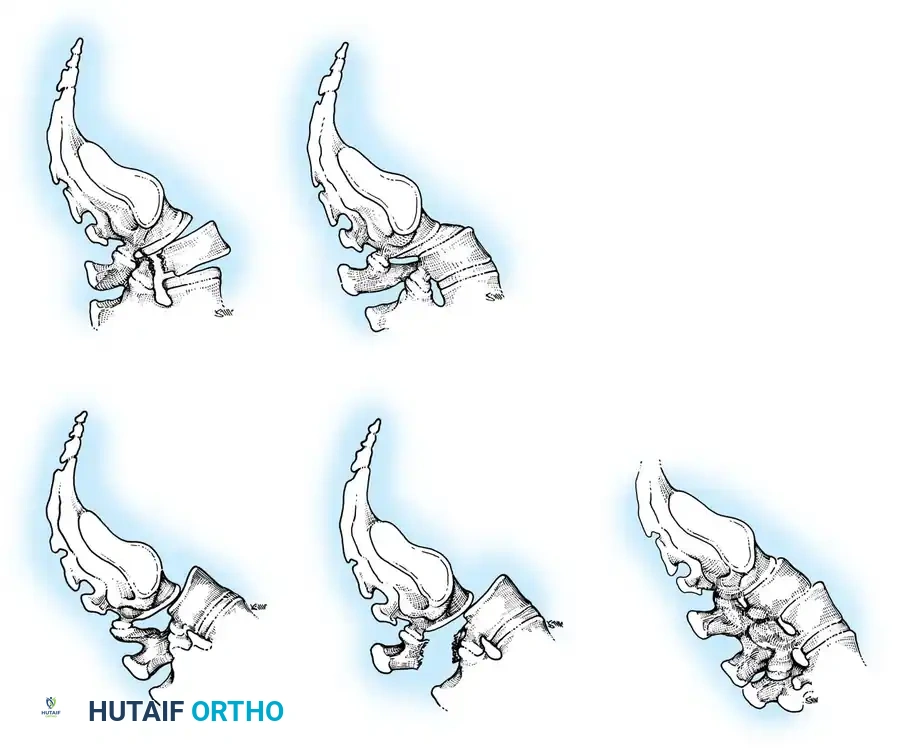
Surgical indications are generally categorized into absolute and relative parameters. Absolute indications include progressive neurological deficits, such as a developing foot drop or cauda equina syndrome, which necessitate emergent or urgent decompression and stabilization. High-grade slips (Meyerding Grade III, IV, or V/spondyloptosis) in pediatric and adolescent patients are universally considered surgical indications due to the extreme risk of progression, severe resulting sagittal imbalance, and the development of the characteristic "pelvic waddle" gait. In these high-dysplastic scenarios, the biomechanical environment is so severely compromised that spontaneous stabilization is virtually impossible.
Relative indications encompass persistent, intractable mechanical axial back pain or radicular leg pain that has failed a minimum of six months of comprehensive conservative care. Additionally, a progressive slip beyond Grade II (50%) in a growing child warrants surgical fusion to halt deformity progression. Contraindications must be carefully weighed. Absolute contraindications include active systemic infection, severe medical comorbidities precluding general anesthesia, and patient refusal. Relative contraindications involve severe osteoporosis (which compromises hardware purchase), active nicotine use (which drastically increases pseudarthrosis rates), and profound psychiatric overlays that may interfere with postoperative rehabilitation compliance.
| Parameter | Indications for Surgical Intervention | Contraindications to Surgery |
|---|---|---|
| Neurological | Progressive motor deficit (e.g., foot drop), Cauda Equina Syndrome, Intractable radiculopathy. | Absence of symptoms in low-grade slips (incidental findings). |
| Biomechanical | High-grade slip (Grade III, IV, V), Documented slip progression in a growing child, Severe sagittal imbalance. | Severe osteoporosis precluding rigid screw fixation (Relative). |
| Clinical | Intractable axial back pain failing >6 months of conservative care, Severe postural deformity (pelvic waddle). | Active systemic or local spinal infection (Absolute). |
| Patient Factors | Failure of bracing and physical therapy, Diminished quality of life. | Uncontrolled medical comorbidities, Active heavy smoking (Relative). |
Pre-Operative Planning, Templating, and Patient Positioning
Comprehensive preoperative planning is the bedrock of successful surgical outcomes in spondylolisthesis management. Standard radiographic evaluation is mandatory and begins with full-length, 36-inch standing scoliosis films. These films are critical for calculating the patient's global sagittal balance (Sagittal Vertical Axis - SVA) and specific spinopelvic parameters, including Pelvic Incidence (PI), Pelvic Tilt (PT), and Sacral Slope (SS). Lowe et al. demonstrated a 26% increase in measured slip on standing lateral films compared to supine films, underscoring the necessity of weight-bearing imaging to assess the true dynamic instability of the segment.


In addition to standard AP and lateral views, the Ferguson Coronal View is highly recommended. In this view, the X-ray beam is angled 30 degrees cephalad, parallel to the L5-S1 disc space. This provides a true en face projection of the L5 pedicles, transverse processes, and the sacral ala, which is invaluable for templating pedicle screw trajectories and planning posterolateral fusion beds. Advanced imaging is utilized to refine the surgical strategy. Computed Tomography (CT) is the gold standard for defining osseous anatomy, assessing the degree of facet dysplasia, and confirming acute stress fractures versus chronic non-unions with sclerotic margins. Furthermore, CT is essential for evaluating bone stock and planning the dimensions of pedicle screws and interbody cages.


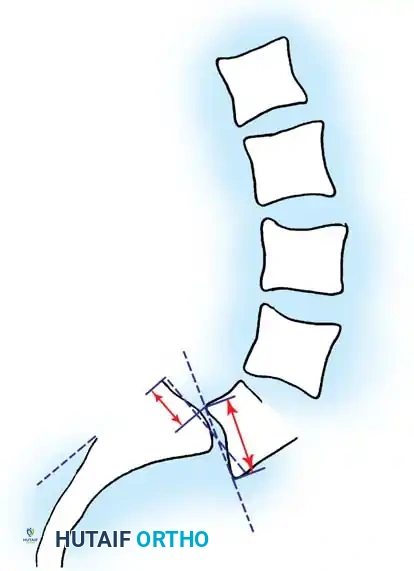
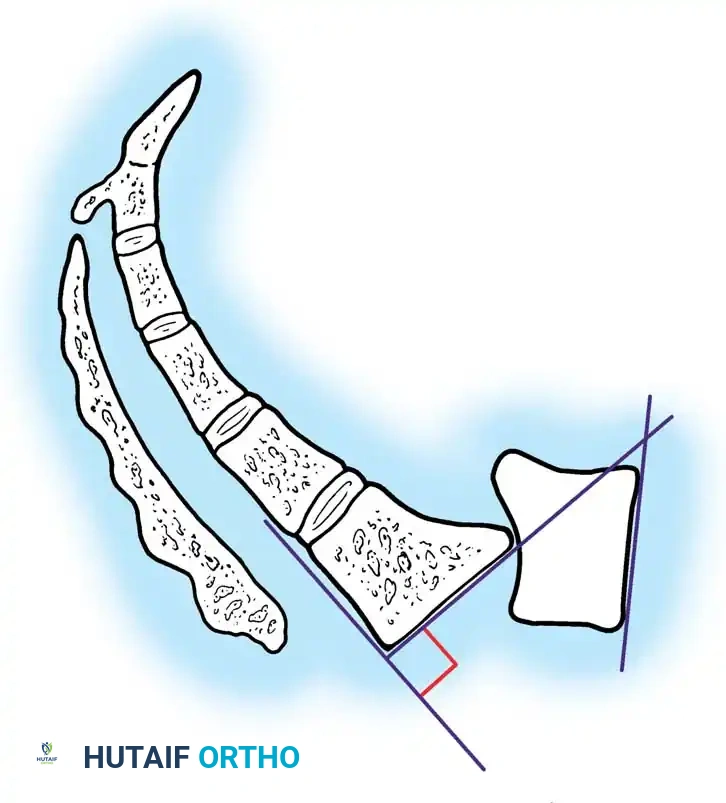
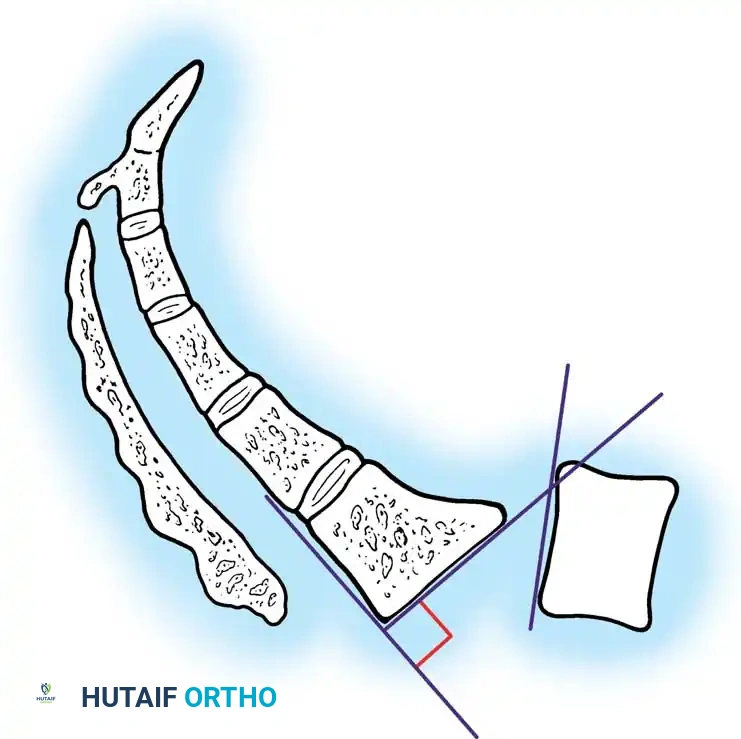
Magnetic Resonance Imaging (MRI) is indispensable for evaluating neural element compression. In isthmic spondylolisthesis, the exiting L5 nerve root is frequently compressed in the neuroforamen by hypertrophic fibrocartilaginous pseudarthrosis tissue at the pars defect (the "Gill lesion"). MRI accurately delineates this foraminal stenosis, as well as the hydration and structural integrity of the adjacent intervertebral discs. Radiographic grading systems, such as the universally applied Meyerding Classification, the DeWald Modification for quantifying anterior "roll," and Boxall's Slip Angle, are meticulously calculated to determine the severity of localized lumbosacral kyphosis and to guide the necessity of reduction maneuvers.


Patient positioning in the operating room is a critical, often underappreciated, step. The patient is typically positioned prone on a radiolucent Jackson spinal table. It is imperative that the abdomen hangs completely free. This decreases intra-abdominal pressure, which in turn reduces inferior vena cava compression, minimizing epidural venous engorgement and intraoperative blood loss. The hips and knees should be extended to maximize lumbar lordosis during the instrumentation and fusion phases. Meticulous padding of all bony prominences and peripheral nerves is required to prevent positioning-related neuropathies during these potentially lengthy procedures.
Step-by-Step Surgical Approach and Fixation Technique
The surgical management of spondylolisthesis requires a meticulous, step-wise approach to ensure adequate decompression, rigid stabilization, and biological fusion. A standard posterior midline incision is utilized, extending from the spinous process of the vertebra above the slip to the sacral spine. Subperiosteal dissection is performed bilaterally to expose the spinous processes, laminae, pars interarticularis, and transverse processes of L4, L5, and the sacral ala. Extreme care must be taken during the exposure of the L5 transverse processes, as the exiting L4 nerve root lies in close proximity anteriorly.


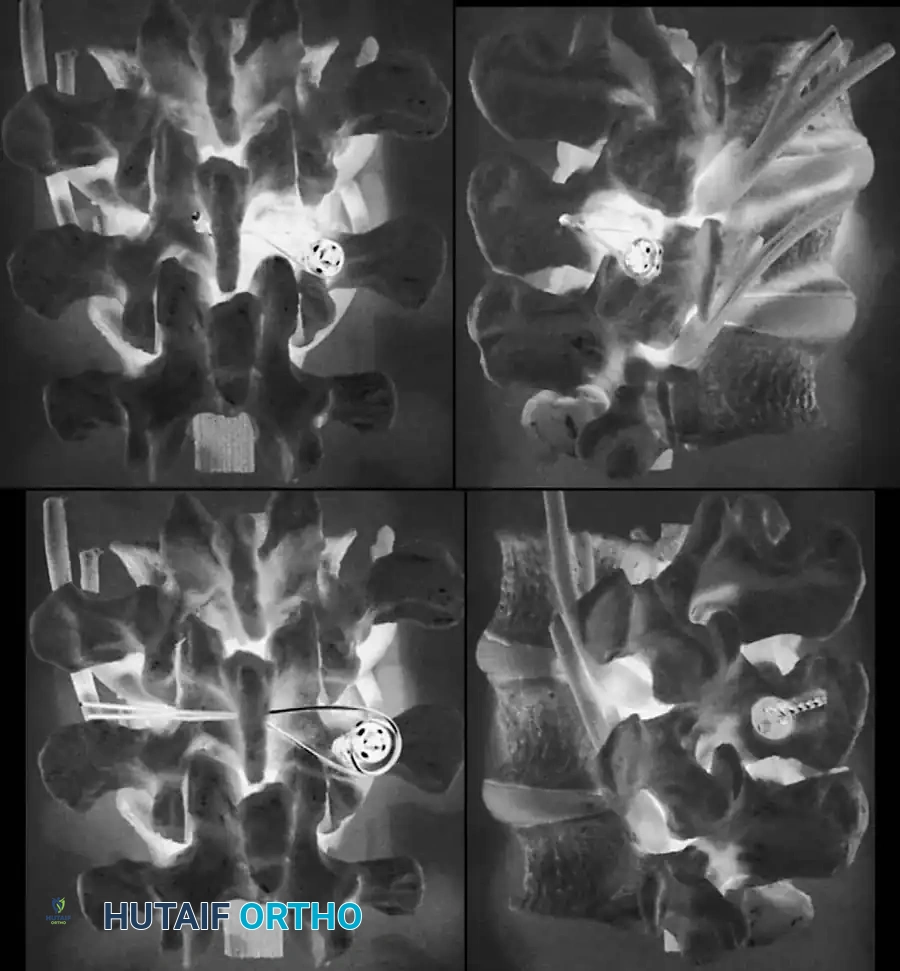
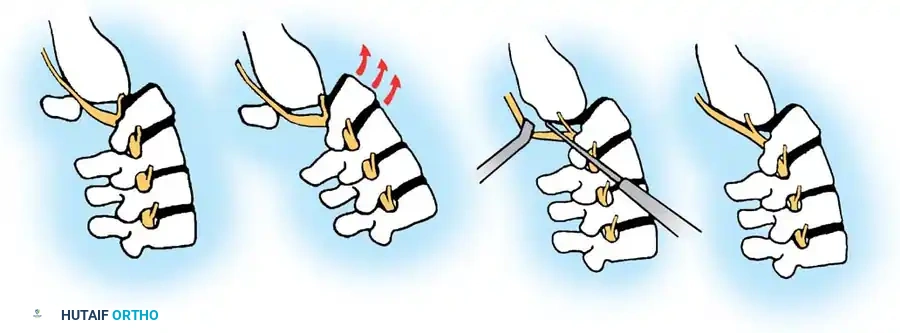
Following exposure, decompression of the neural elements is undertaken. In the setting of a lytic slip, the posterior arch of L5 (the lamina and inferior articular processes) is essentially "floating," disconnected from the vertebral body by the bilateral pars defects. A Gill laminectomy involves the en bloc removal of this loose posterior element. It is a critical surgical pitfall to leave this floating lamina in place while attempting reduction, as pulling the L5 vertebral body posteriorly will cause the intact posterior arch to act as a guillotine, severely compressing the cauda equina against the sacrum. Once the lamina is removed, the fibrocartilaginous pseudarthrosis tissue at the pars defects must be meticulously excised to thoroughly decompress the exiting L5 nerve roots bilaterally.

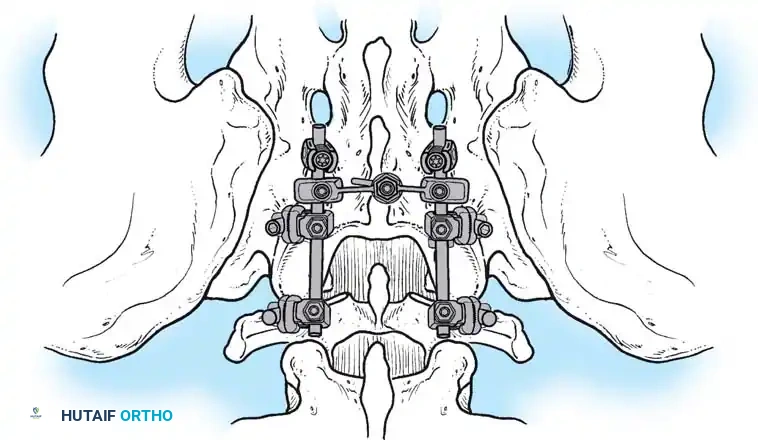
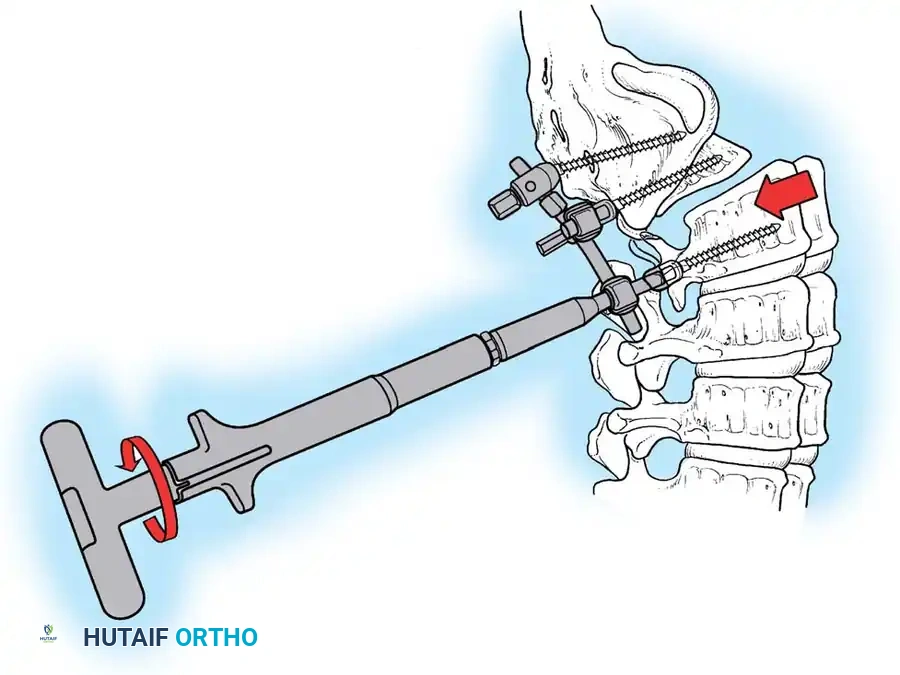
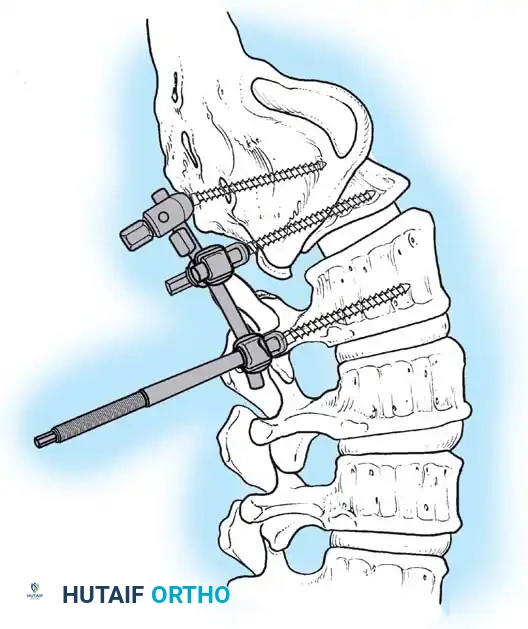
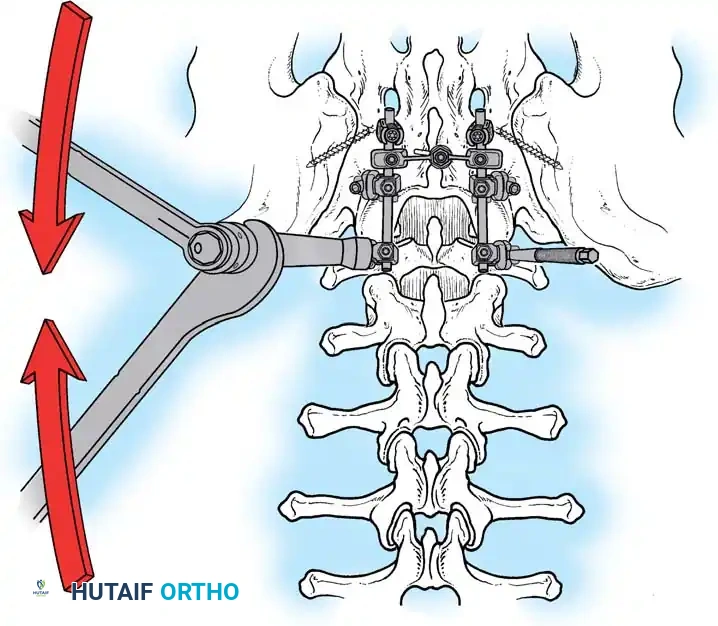
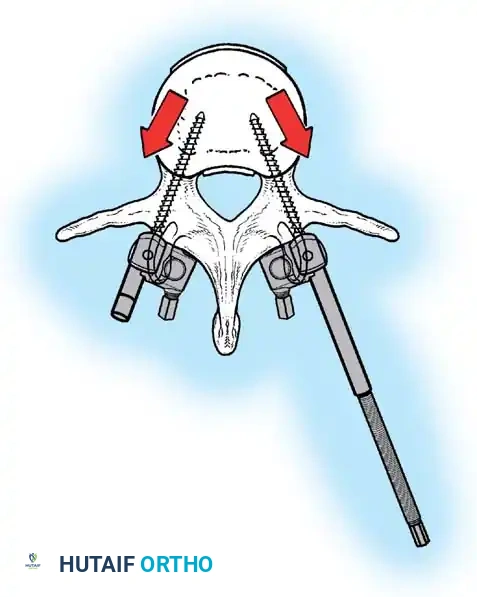
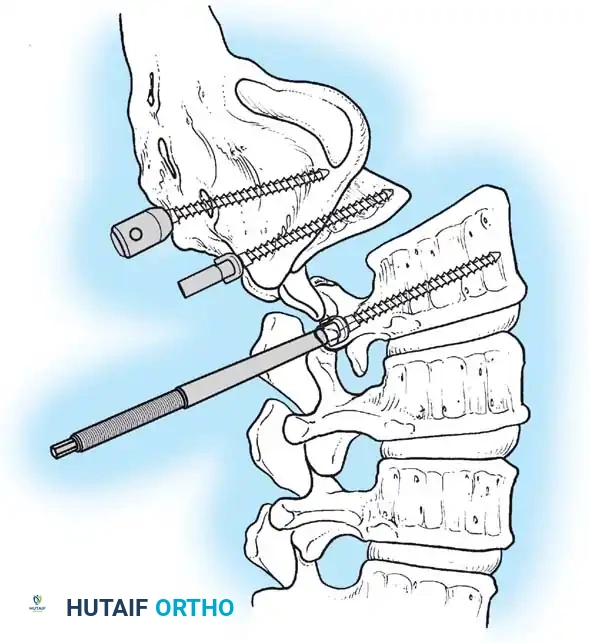
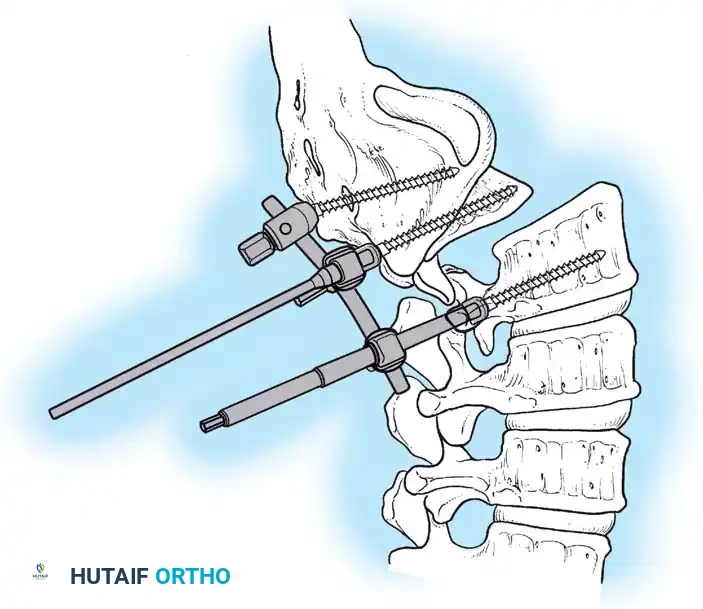
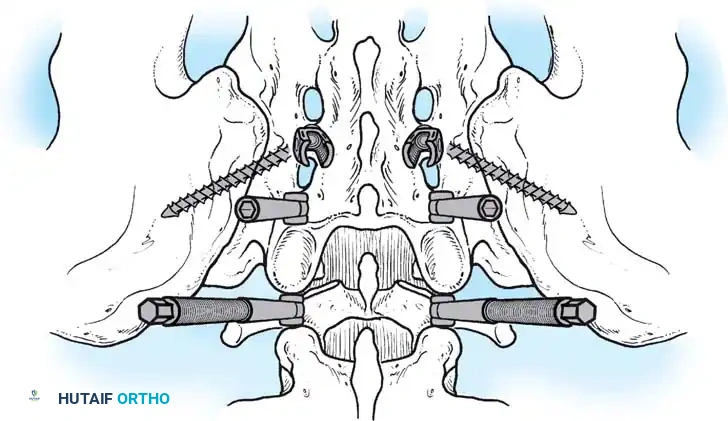
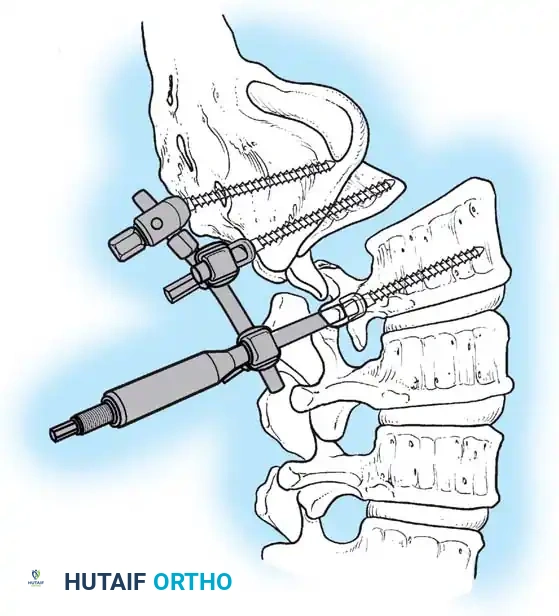
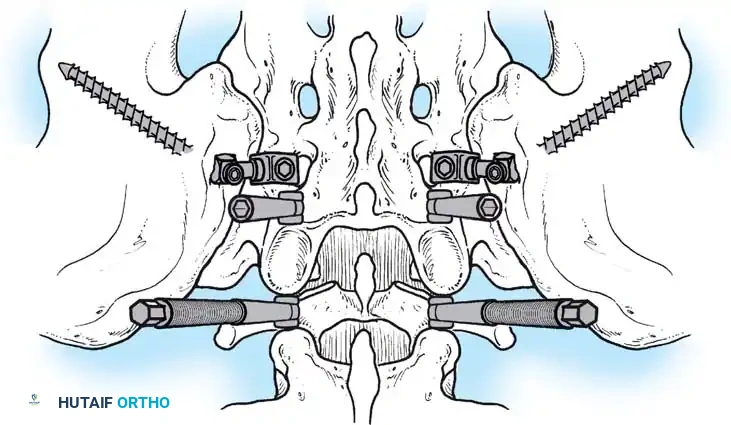
Pedicle screw instrumentation is the gold standard for stabilizing the lumbosacral junction. Screws are placed bilaterally into the L5 pedicles and the S1 pedicles. In high-grade slips (Grade III or above), the L5 pedicles are often dysplastic, and the anatomy is grossly distorted. In such cases, instrumentation is frequently extended proximally to L4 and distally into the pelvis (using iliac or S2-alar-iliac screws) to provide a robust mechanical anchor and prevent sacral screw pullout. The trajectory of the L5 screws must be carefully planned, often requiring a more medial and cephalad angulation due to the anterior and inferior displacement of the vertebral body.


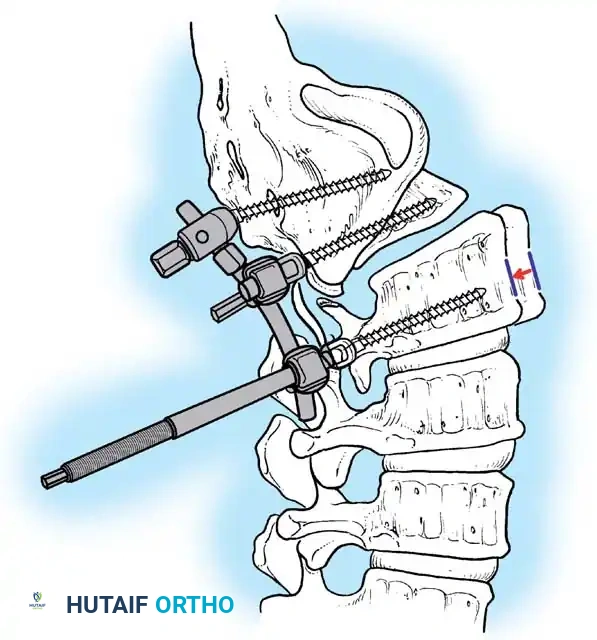
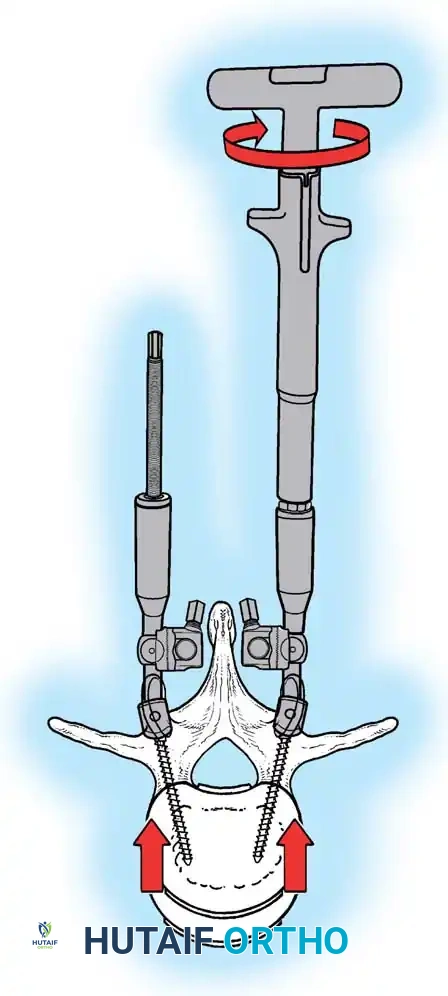
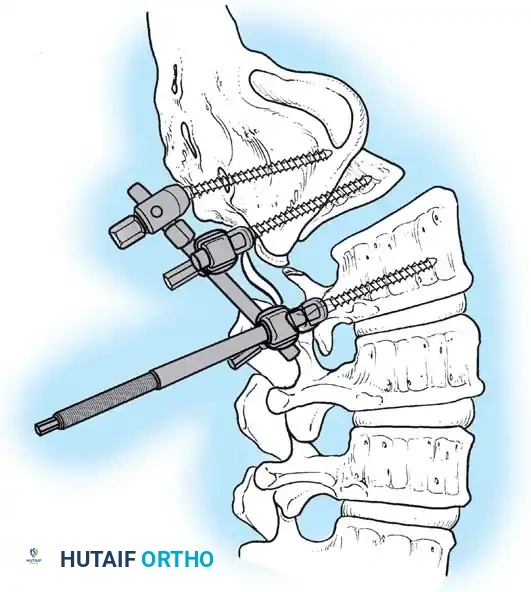
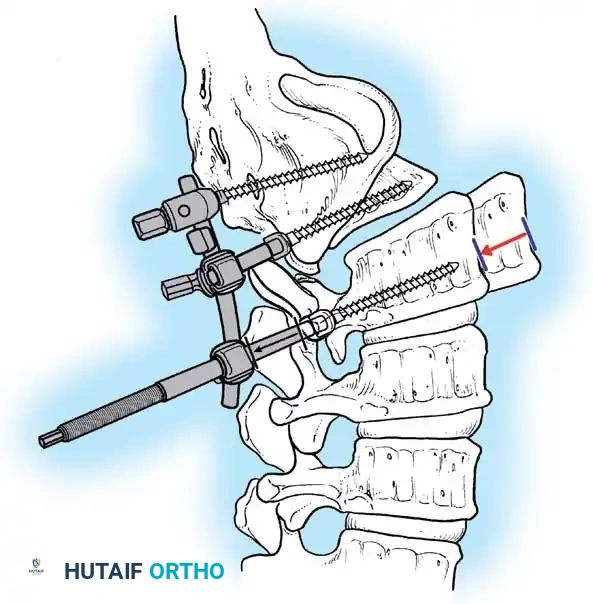
The decision to actively reduce the spondylolisthesis versus fusing in situ remains one of the most debated topics in spine surgery. Partial reduction is generally advocated to improve sagittal balance, restore the slip angle, and increase the surface area available for interbody fusion. However, aggressive reduction maneuvers carry a significant risk of stretching the exiting L5 nerve root, leading to postoperative neuropraxia or permanent deficit. Interbody fusion, utilizing Transforaminal Lumbar Interbody Fusion (TLIF) or Posterior Lumbar Interbody Fusion (PLIF) techniques, is heavily favored to provide anterior column support, restore foraminal height, and achieve a circumferential (360-degree) arthrodesis. Copious autograft, often supplemented with allograft or biologics like Bone Morphogenetic Protein (BMP), is packed into the disc space and along the decorticated transverse processes to ensure a robust fusion mass.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the operative management of spondylolisthesis is associated with a specific profile of complications that the surgeon must be prepared to manage. The overall complication rate scales directly with the severity of the slip, the complexity of the deformity, and the necessity for reduction maneuvers. Thorough preoperative patient counseling regarding these risks is a mandatory component of informed consent.
Neurological injury is the most feared complication, with L5 nerve root neuropraxia being particularly prevalent during reduction of high-grade slips. The L5 root is tethered by the lumbosacral ligament and is acutely stretched as the L5 vertebral body is pulled posteriorly and superiorly over the sacral dome. The incidence of L5 root injury during high-grade reduction ranges from 5% to 30% in the literature. Intraoperative neuromonitoring (somatosensory evoked potentials and spontaneous/triggered electromyography) is absolutely critical. If monitoring alerts occur during reduction, the surgeon must immediately release the tension and accept a lesser degree of reduction or revert to an in situ fusion. Most stretch palsies are transient, but recovery can take several months.
Incidental durotomy (dural tear) is another common intraoperative complication, particularly during the dissection of dense epidural adhesions or the excision of the Gill lesion. Primary watertight repair using 4-0 or 5-0 non-absorbable suture is the salvage treatment of choice, often supplemented with a dural sealant and a fascial or fat patch. Postoperatively, patients may require a period of flat bedrest to prevent cerebrospinal fluid (CSF) fistulas. Pseudarthrosis (non-union) remains a significant long-term failure mode, especially in patients with poor bone quality, active smokers, or when anterior column support (interbody fusion) is omitted in highly unstable segments. Hardware failure, such as screw breakage or rod fracture, is typically secondary to an underlying pseudarthrosis and requires revision surgery with extension of the construct and biological
Clinical & Radiographic Imaging Archive