Operative Management of Spinal Infections: A Comprehensive Surgical Guide
Key Takeaway
Spinal infections, encompassing pyogenic spondylodiscitis and tuberculous spondylitis, present complex diagnostic and surgical challenges. Successful management requires a multidisciplinary approach, combining targeted antimicrobial therapy with radical surgical debridement, anterior column reconstruction, and rigid internal fixation. This guide details the historical evolution, biomechanical principles, and step-by-step surgical techniques essential for eradicating infection, restoring spinal stability, and preventing severe neurological sequelae in affected patients.
Comprehensive Introduction and Patho-Epidemiology
The management of spinal infections, encompassing pyogenic spondylodiscitis, epidural abscesses, and granulomatous osteomyelitis, represents one of the most formidable and high-stakes challenges in operative orthopaedics and spine surgery. Evidence of spinal infection in humans predates recorded history; Neolithic remains (c. 7000–300 B.C.) and Egyptian mummies (c. 3000 B.C.) exhibit profound kyphotic deformities characteristic of tuberculous spondylitis. Hippocrates first described the clinical condition, astutely noting that the prognosis was superior when the infection localized below the diaphragm. In 1779, Sir Percivall Pott provided the first comprehensive clinical description of tuberculous spinal infection, forever linking his name to the disease (Pott's disease) and its devastating neurological sequelae (Pott paraplegia). The scientific understanding of pyogenic osteomyelitis advanced significantly in 1884 when Rodet demonstrated its development following intravenous injections of Staphylococcus aureus in animal models. Before the advent of modern antimicrobial therapy, mortality rates for spinal infections ranged from 40% to 70%, and early surgical interventions were strictly limited to the palliative drainage of massive abscesses.
Despite the advent of broad-spectrum antimicrobial chemotherapy and advanced neuroimaging, spinal infections remain a critical public health issue with a rising incidence. Currently, vertebral osteomyelitis accounts for approximately 2% to 4% of all osteomyelitis cases, with an estimated incidence of 4.8 to 5.8 cases per 100,000 population in developed nations. This epidemiological shift is driven by an aging population, the escalating prevalence of medical comorbidities (e.g., diabetes mellitus, chronic kidney disease), expanding cohorts of immunocompromised hosts, and the ongoing epidemic of intravenous drug use (IVDU). Mortality has decreased significantly from the pre-antibiotic era but still ranges from 1% to 20%, heavily dependent on patient frailty, the presence of endocarditis, and the virulence of the infecting organism. The most alarming statistic remains the incidence of neurological compromise; paralysis or severe paresis is reported in up to 50% of patients, varying by the spinal segment involved and the specific patient population. A persistent clinical challenge is the delay in diagnosis, which currently averages 2 to 3 months from symptom onset.
The pathophysiology of spinal infections is dictated by the unique vascular anatomy of the vertebral column. Infections typically originate via three primary routes: hematogenous dissemination, direct inoculation, and contiguous spread. Hematogenous spread is overwhelmingly the most common etiology. In the adult spine, the intervertebral disc is largely avascular; therefore, blood-borne pathogens lodge in the highly vascularized subchondral bone of the vertebral endplates, specifically within the terminal capillary loops of the metaphyseal arterial supply. The sluggish blood flow in these venous lakes, combined with the lack of phagocytic cells in the adjacent avascular disc, creates an immunologically privileged sanctuary for bacterial proliferation. The infection subsequently destroys the bony endplate and invades the disc space via the elaboration of bacterial proteolytic enzymes. Alternatively, retrograde flow through the valveless epidural venous plexus of Batson during periods of increased intra-abdominal pressure (e.g., Valsalva maneuver) can seed the spine from pelvic or urogenital infections.
Microbiologically, Staphylococcus aureus remains the predominant pathogen, responsible for over 50% of pyogenic cases, with Methicillin-resistant S. aureus (MRSA) representing a growing and particularly virulent subset. Coagulase-negative staphylococci (S. epidermidis) are frequently implicated in postoperative surgical site infections and delayed hardware seeding. Gram-negative bacilli, including Escherichia coli and Pseudomonas aeruginosa, are increasingly isolated, particularly in the context of genitourinary tract procedures, advanced age, and intravenous drug use. Granulomatous infections, most notably Mycobacterium tuberculosis, exhibit a distinct pathophysiological mechanism; they typically spare the intervertebral disc until late in the disease process due to a lack of proteolytic enzymes, instead causing profound destruction of the anterior vertebral body. This leads to the classic sharp, angular kyphosis known as a gibbus deformity. Fungal osteomyelitis (e.g., Coccidioides, Aspergillus, Candida) remains rare but is a critical consideration in endemic regions and profoundly immunosuppressed cohorts.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of spinal anatomy and regional biomechanics is the sine qua non of successful operative intervention for spinal infections. The vertebral column is structurally divided into the anterior column (comprising the anterior longitudinal ligament, the anterior two-thirds of the vertebral body, and the annulus fibrosus) and the posterior column (encompassing the posterior third of the vertebral body, posterior longitudinal ligament, pedicles, facets, lamina, and the posterior ligamentous complex). The anterior column is the primary load-bearing axis of the human spine, supporting approximately 80% of physiological axial compressive loads in the upright posture. Because the microvascular anatomy predisposes the subchondral endplates to initial bacterial seeding, spondylodiscitis is fundamentally a disease of the anterior column. As the infection incites an intense inflammatory response, osteoclastic resorption outpaces osteoblastic bone formation, leading to cavitary defects within the cancellous centrum of the vertebral body and subsequent structural collapse.
The biomechanical consequences of anterior column destruction are catastrophic if left untreated. As the vertebral body and intervertebral disc lose their structural integrity, the anterior column foreshortens. This pathological collapse shifts the instantaneous axis of rotation (IAR) posteriorly, transforming normal axial compressive forces into immense tensile stresses applied to the posterior ligamentous complex (PLC). The intact PLC may temporarily resist this stress, acting as a tension band; however, progressive anterior bone loss inevitably leads to a biomechanical failure of this tension band mechanism. The result is progressive kyphotic deformity. This regional kyphosis is not merely a cosmetic issue; it mechanically tethers the spinal cord and nerve roots over the apex of the bony deformity. When combined with the space-occupying effect of ventral epidural abscesses and inflammatory granulation tissue, this biomechanical collapse is the primary driver of profound myelopathy and irreversible neurological deficits.
Regional anatomical variations dictate both the clinical presentation and the surgical approach. In the cervical spine, the relatively small vertebral bodies and high degree of mobility make it highly susceptible to rapid collapse and severe kyphosis. The cervical spinal canal is narrow relative to the diameter of the spinal cord, meaning even small epidural abscesses or minor degrees of retropulsion can precipitate acute tetraplegia. Furthermore, anterior cervical abscesses can track along the prevertebral fascia, presenting as retropharyngeal abscesses that threaten the airway. In the thoracic spine, the physiological kyphosis and the rigid splinting effect of the rib cage alter the biomechanical environment. While the rib cage provides some intrinsic stability, the thoracic spinal canal is the narrowest in the entire neuraxis, and the regional blood supply to the spinal cord (the watershed zone of the artery of Adamkiewicz) is tenuous. Consequently, thoracic epidural abscesses carry the highest risk of devastating paraplegia.
The lumbar spine, characterized by massive vertebral bodies and a physiological lordosis, is designed to withstand immense axial loads. Spondylodiscitis in the lumbar spine frequently involves the psoas musculature, as the infection tracks laterally along the path of least resistance, yielding massive psoas abscesses that can extend distally to the groin and thigh. The lumbar canal contains the cauda equina rather than the spinal cord; these peripheral nerve roots are relatively more resilient to compression than the central nervous system tracts of the cord. Therefore, lumbar infections may present with profound radicular pain and isolated motor deficits rather than upper motor neuron signs. However, the surgical reconstruction of the lumbar spine demands robust biomechanical support, as the reconstruction must restore the physiological lordosis to maintain global sagittal balance and prevent adjacent segment degeneration.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention in the setting of spinal infection requires a nuanced synthesis of the patient's neurological status, biomechanical stability, systemic physiological reserve, and response to empirical or targeted antimicrobial therapy. The historical paradigm dictated that the vast majority of pyogenic spinal infections could be managed non-operatively with prolonged intravenous antibiotics and rigid orthotic bracing. While this remains true for early, uncomplicated spondylodiscitis without structural collapse, the threshold for surgical intervention has progressively lowered. This shift is driven by advancements in rigid spinal instrumentation, minimally invasive techniques, and a deeper understanding of the devastating long-term consequences of post-infectious kyphosis. Surgery is not merely a salvage procedure; when appropriately indicated, it is the definitive method for achieving source control, protecting the neural elements, and restoring the mechanical integrity of the spine.
Absolute indications for emergent or urgent surgical intervention are well-defined within the orthopaedic and neurosurgical literature. The most critical indication is the presence of a progressive neurological deficit in the setting of an epidural abscess or severe bony retropulsion. Time is of the essence; decompression performed within 24 to 36 hours of the onset of neurological symptoms is associated with significantly higher rates of functional recovery. A second absolute indication is the presence of gross clinical or radiographic spinal instability, defined as progressive kyphotic deformity, translation, or the destruction of more than 50% of the vertebral body height. Failure to stabilize such lesions inevitably leads to delayed neurological compromise and severe, intractable mechanical back pain. Additionally, the presence of an epidural abscess in the cervical or thoracic spine, even in the absence of profound neurological deficits, is frequently treated with early surgical decompression due to the high risk of sudden, irreversible ischemic injury to the spinal cord.
Relative indications for surgery require careful multidisciplinary deliberation. Failure of medical management is a primary relative indication, defined as persistent or worsening clinical symptoms (intractable pain), persistently elevated inflammatory markers (C-reactive protein [CRP] and Erythrocyte Sedimentation Rate [ESR]), or progressive radiographic bony destruction despite 4 to 6 weeks of culture-directed intravenous antimicrobial therapy. Another common indication is the necessity for an open biopsy. When multiple CT-guided percutaneous needle biopsies fail to yield a causative organism—a scenario occurring in up to 30% of cases—an open surgical biopsy and debridement are mandated to isolate the pathogen, particularly in patients who are deteriorating or who reside in regions endemic for tuberculosis or fungal pathogens. Finally, severe, intractable mechanical back pain that prevents mobilization and threatens the patient with the complications of prolonged bed rest (e.g., deep vein thrombosis, decubitus ulcers, pneumonia) may justify surgical stabilization.
Contraindications to operative management are primarily dictated by the patient's systemic ability to tolerate major reconstructive surgery. Severe hemodynamic instability, profound septic shock requiring high-dose vasopressor support, and multi-organ failure constitute absolute contraindications to complex spinal reconstruction, though palliative bedside or minimally invasive drainage of an abscess may be attempted as a life-saving measure. Severe medical comorbidities, such as end-stage cardiopulmonary disease, uncorrectable coagulopathy, or profound immunodeficiency, significantly elevate the perioperative mortality risk and must be weighed against the natural history of the infection. In cases of extensive, multi-level holospinal infection where complete debridement is anatomically impossible, radical surgery may be contraindicated in favor of long-term suppressive antimicrobial therapy and palliative bracing.
| Clinical Scenario / Parameter | Operative Indications | Operative Contraindications |
|---|---|---|
| Neurological Status | Progressive motor deficit, cauda equina syndrome, acute myelopathy. | Stable, non-progressive radiculopathy responsive to steroids/antibiotics. |
| Biomechanical Stability | Progressive kyphosis, >50% vertebral body collapse, translation >3mm. | Intact anterior column, preserved disc height, no dynamic instability. |
| Infectious Disease Factors | Failure of medical management (>4-6 weeks), unknown pathogen after percutaneous biopsy. | Rapid clinical and laboratory (CRP/ESR) improvement on IV antibiotics. |
| Systemic Health | Intractable mechanical pain preventing mobilization, ASA Class I-III. | Hemodynamic instability, severe sepsis/shock, uncorrectable coagulopathy. |
| Anatomical Considerations | Ventral epidural abscess causing cord compression (especially Cervical/Thoracic). | Holospinal diffuse osteomyelitis lacking a focal compressive lesion. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the foundation of successful surgical execution in the infected spine. The diagnostic imaging workup must be exhaustive. Magnetic Resonance Imaging (MRI) with and without gadolinium contrast is the gold standard modality. Short tau inversion recovery (STIR) and T2-weighted sequences are exquisitely sensitive for detecting bone marrow edema and disc space inflammation, while T1-weighted post-contrast images clearly delineate the enhancing margins of epidural, paraspinal, and psoas abscesses. However, MRI overestimates the extent of cortical bone destruction. Therefore, a fine-cut Computed Tomography (CT) scan with sagittal and coronal reconstructions is absolutely mandatory for surgical templating. The CT scan allows the surgeon to accurately assess the degree of osteolysis, measure the regional kyphotic angle, and evaluate the morphometry of the pedicles for planned instrumentation. In patients with severe osteoporosis, Hounsfield unit measurements on CT can guide the decision to utilize cement-augmented pedicle screws.
Medical optimization prior to surgery is critical, though often constrained by the urgency of the neurological presentation. A multidisciplinary approach involving infectious disease specialists, internal medicine, and anesthesiology is required. Nutritional status is a profound predictor of post-operative wound healing and infection clearance; serum albumin, pre-albumin, and total lymphocyte counts should be assessed. While acute malnutrition cannot be reversed overnight, early enteral or parenteral feeding protocols should be initiated. Glycemic control is paramount, as hyperglycemia severely impairs leukocyte function and exacerbates surgical site infections. If the patient is on immunosuppressive medications (e.g., TNF-alpha inhibitors, high-dose corticosteroids), these must be carefully managed and typically held in consultation with the prescribing rheumatologist or oncologist. Furthermore, a thorough cardiac and pulmonary evaluation is necessary, particularly for thoracic approaches that require single-lung ventilation.
Patient positioning is a critical step that dictates the ease of anatomical exposure and the safety of the neural elements. For anterior cervical approaches, the patient is positioned supine with the neck slightly extended using a rolled towel beneath the interscapular region; extreme extension must be avoided in the presence of severe stenosis or instability to prevent iatrogenic cord injury. Thoracic anterior approaches (transthoracic or thoracoabdominal) require the lateral decubitus position. The patient is typically positioned with the side of the maximal abscess facing upward. An axillary roll is placed, and the patient is secured with rigid bean bags and adhesive tape. A double-lumen endotracheal tube is utilized by anesthesia to allow for selective deflation of the ipsilateral lung, providing a clear corridor to the thoracic spine. Lumbar anterior approaches also utilize the lateral decubitus position, employing a retroperitoneal approach to avoid peritoneal contamination and minimize bowel manipulation.
For posterior approaches, including costotransversectomy or standard posterior instrumented fusion, the patient is positioned prone. The utilization of a radiolucent Jackson table or a specialized spine frame is mandatory. The abdomen must hang completely free; any compression of the abdomen increases intra-abdominal pressure, which is transmitted to the epidural venous plexus of Batson, resulting in torrential intra-operative epidural bleeding that obscures the surgical field. All pressure points (face, axillae, ulnar nerves, genitalia, knees) must be meticulously padded. Intra-operative neuromonitoring (IONM), including Somatosensory Evoked Potentials (SSEPs) and Motor Evoked Potentials (MEPs), is highly recommended, particularly when correcting severe kyphotic deformities. Baseline signals must be obtained prior to positioning, and any loss of signals during the turn to the prone position necessitates immediate reversal and reassessment of spinal stability.
Step-by-Step Surgical Approach and Fixation Technique
Anterior Decompression and Reconstruction
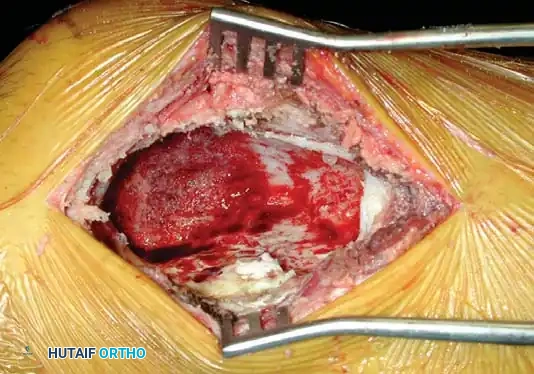
Because spinal infections predominantly destroy the anterior column, the anterior approach remains the most direct and mechanically sound method for achieving radical debridement and structural reconstruction. The primary goal is the complete extirpation of all necrotic bone, infected disc material, and purulent exudate until healthy, bleeding cancellous bone is encountered—a concept championed by Hodgson and Stock in their pioneering "Hong Kong operation" for tuberculosis.
In the cervical spine, a standard Smith-Robinson anterolateral approach is utilized. The prevertebral fascia, which often contains the abscess, is incised, and purulent material is immediately sent for aerobic, anaerobic, mycobacterial, and fungal cultures. A radical corpectomy of the involved vertebral bodies is performed using a high-speed burr and Kerrison rongeurs. The decompression must extend laterally to the uncovertebral joints to decompress the neural foramina, and posteriorly to the posterior longitudinal ligament (PLL). If an epidural abscess is present, the PLL must be meticulously resected using micro-curettes to expose and decompress the dura. The resulting defect is reconstructed using a structural autograft (tricortical iliac crest or fibula) or a titanium mesh cage filled with local autograft or allograft. Anterior cervical plating is applied to provide immediate rigid stability, spanning from the healthy vertebra above to the healthy vertebra below.
In the thoracic spine, a transthoracic or thoracoabdominal approach provides unparalleled access to the anterior column. After deflating the ipsilateral lung, the parietal pleura overlying the spine is incised. The segmental vessels at the level of the infected vertebral bodies are isolated, ligated, and divided at the mid-vertebral body level to mobilize the great vessels (aorta or vena cava) away from the spine. Radical corpectomy is performed. The thoracic spinal canal is accessed by removing the posterior wall of the vertebral body, allowing for direct ventral decompression of the spinal cord. Following copious irrigation with saline and local antibiotics, a structural rib autograft (harvested during the thoracotomy), fibular strut, or expandable titanium cage is impacted into the defect. Anterolateral screw-rod instrumentation can be applied for stabilization, though severe cases often require supplemental posterior fixation.
The lumbar spine is approached via an anterolateral retroperitoneal corridor. This minimizes the risk of peritoneal contamination and paralytic ileus. The psoas muscle is frequently engorged and infiltrated with purulent material (psoas abscess). The abscess is drained, and the psoas muscle must be carefully mobilized and retracted posteriorly. Extreme caution is required to protect the lumbar plexus, which resides within the substance of the psoas. Following radical discectomy and partial or complete corpectomy, the endplates of the adjacent healthy vertebrae are prepared. A large-footprint titanium cage or structural allograft is inserted to restore lumbar lordosis and foraminal height. Given the massive biomechanical forces in the lumbar spine, anterior-only constructs are prone to failure in the setting of infection; thus, supplemental posterior pedicle screw fixation is standard practice.
Posterior Approaches and Costotransversectomy
When profound anterior column destruction exists but the patient cannot tolerate a thoracotomy or laparotomy due to severe medical or pulmonary comorbidities, posterior-only approaches offer a viable alternative. The costotransversectomy or lateral extracavitary approach provides access to the anterior column via a posterior midline or paramedian incision. The paraspinal muscles are mobilized laterally. The transverse process and the proximal 3 to 5 cm of the corresponding rib are resected at the involved levels. The intercostal nerve is identified and traced medially to the neural foramen. By resecting the pedicle, a corridor is created lateral to the thecal sac, allowing the surgeon to evacuate a ventral paraspinal abscess and perform a limited debridement of the vertebral body and disc space.
While costotransversectomy avoids the morbidity of a chest tube and single-lung ventilation, it has distinct limitations. It is technically demanding to place a large structural strut graft into the anterior column via this narrow posterior corridor. Furthermore, visualization of the contralateral epidural space is limited, increasing the risk of incomplete decompression. Therefore, posterior approaches are frequently utilized in conjunction with transpedicular decompression and the placement of expandable titanium cages, followed by long-segment posterior pedicle screw fixation to bypass the diseased anterior column and provide immediate biomechanical stability.
Instrumentation in the Setting of Active Infection
Historically, placing foreign bodies (hardware) into an infected surgical field was considered a strict contraindication, governed by the fear of biofilm formation and persistent, incurable osteomyelitis. However, modern clinical evidence has completely overturned this paradigm. Rigid internal fixation is now recognized as essential for promoting bony arthrodesis, which is the ultimate biological cure for osteomyelitis. Micro-motion at the site of infection perpetuates inflammation and prevents bacterial clearance; rigid stabilization arrests this cycle.
The choice of biomaterial is critical. Titanium and its alloys are highly preferred over stainless steel or cobalt-chrome. Titanium exhibits superior biocompatibility, significantly reduced artifact on post-operative MRI (allowing for accurate surveillance), and, crucially, a lower propensity for bacterial glycocalyx (biofilm) adherence. When placing pedicle screws in the infected and often osteoporotic spine, meticulous technique is required. The trajectory must be optimized to maximize cortical purchase. In cases of severe bone loss, the use of fenestrated pedicle screws with polymethylmethacrylate (PMMA) cement augmentation provides superior pull-out strength. The modern consensus dictates that radical surgical debridement, copious pulsatile lavage, and the placement of titanium instrumentation, followed by targeted, prolonged antimicrobial therapy, is safe, efficacious, and represents the standard of care for complex spinal infections.
Complications, Incidence Rates, and Salvage Management
The operative management of spinal infections is fraught with potential complications, stemming from the inherent fragility of the infected tissue, the proximity of critical neurovascular structures, and the compromised systemic state of the host. Complications can be broadly categorized into neurological, biomechanical (hardware-related), and infectious/medical domains. Anticipation, early recognition, and aggressive management of these complications are critical to preventing catastrophic outcomes.
Neurological complications are the most feared. Iatrogenic injury to the spinal cord or nerve roots can occur during radical debridement, particularly when dissecting dense inflammatory granulation tissue away from the dura. The incidence of new or worsening neurological deficit post-operatively ranges from 2% to 5%. Post-operative epidural hematoma is a surgical emergency that presents with acute, progressive neurological decline in the immediate post-operative period; it mandates emergent return to the operating room for evacuation. Failure to adequately decompress the neural elements, either due to retained ventral bone fragments or an unrecognized contralateral abscess, can also lead to persistent or worsening myelopathy, requiring revision decompression.
Biomechanical and hardware-related complications are highly prevalent, occurring in 10% to 20% of cases, primarily due to the poor bone quality associated with osteomyelitis and disuse osteopenia. Subsidence of the anterior interbody cage into the adjacent vertebral bodies is common; while mild subsidence is tolerated, severe subsidence leads to a loss of sagittal alignment and recurrent foraminal stenosis. Pedicle screw pull-out or fracture of the posterior rods can occur if the construct is subjected to excessive stress before solid bony fusion is achieved. The "race" in spinal infection surgery is between the biological process of bony arthrodesis and the mechanical failure of the hardware. If pseudoarthrosis (non-union) occurs, the hardware will inevitably fail, necessitating revision surgery, extension of the fusion construct, and potentially the use of bone morphogenetic proteins (BMP), though the use of BMP in active infection remains controversial and off-label.
Infectious and medical complications reflect the systemic burden of the disease. Recurrent or persistent infection occurs in 5% to 15% of patients, often due to inadequate initial debridement, retained necrotic bone, or the presence of highly resistant organisms (e.g., MRSA, Pseudomonas). Management requires repeat radical debridement, exchange of hardware if gross loosening is present, and consultation with infectious disease for optimization of the antimicrobial regimen. Approach-related complications are unique to the surgical corridor utilized. Anterior cervical approaches carry risks of dysphagia, recurrent laryngeal nerve palsy (vocal cord paralysis), and esophageal perforation. Thoracic approaches can result in pulmonary contusion, atelectasis, pneumonia, or chylothorax from thoracic duct injury. Lumbar retroperitoneal approaches risk injury to the ureter, sympathetic chain (resulting in retrograde ejaculation in males), and the lumbar plexus.
| Complication Category | Specific Complication | Estimated Incidence | Salvage / Management Strategy |
|---|---|---|---|
| Neurological | Post-op Epidural Hematoma | 1 - 3% | Emergent MRI, immediate return to OR for evacuation and hemostasis. |
| Neurological | Iatrogenic Cord/Nerve Injury | 2 - 5% | High-dose MAP maintenance (>85 mmHg), steroids (controversial), rehabilitation. |
| Biomechanical | Cage Subsidence / Hardware Failure | 10 - 20% | Revision surgery, extension of posterior fusion construct, cement augmentation. |
| Biomechanical | Pseudoarthrosis (Non-union) | 5 - 15% | Revision grafting, optimization of metabolic bone health, electrical bone stimulation. |
| Infectious | Persistent/Recurrent Infection | 5 - 15% | Repeat radical debridement, hardware retention if stable, long-term suppressive IV antibiotics. |
| Approach-Related | Recurrent Laryngeal Nerve Palsy | 2 - 8% (Cervical) | ENT evaluation, vocal cord injection if persistent >6 months, speech therapy. |
| Approach-Related | Chylothorax | 1 - 2% (Thoracic) | Conservative (medium-chain triglyceride diet), thoracic duct ligation if output >1L/day. |
Phased Post-Operative Rehabilitation Protocols
Successful surgical intervention is merely the culmination of the acute phase of treatment; the ultimate eradication of the infection and restoration of function require strict adherence to a phased, multidisciplinary post-operative protocol. The rehabilitation timeline is dictated by the rigidity of the surgical construct, the virulence of the pathogen, and the patient's pre-operative neurological baseline.
Phase I: Acute Post-Operative Phase (0 to 2 weeks)
The immediate focus is on hemodynamic stability, pain control, and the initiation of targeted antimicrobial therapy. Patients are typically monitored in an Intensive Care Unit (ICU) or step-down unit for the first 24 to 48 hours. Intravenous antibiotics are tailored based on the intra-operative culture sensitivities and are administered via a Peripherally Inserted Central Catheter (PICC). Surgical drains are monitored closely and removed when output is minimal (typically <30 cc per shift). Early mobilization is paramount to prevent deep vein thrombosis (DVT), pulmonary embolism, and generalized deconditioning. Physical therapy is initiated on post-operative day one, focusing on log-rolling, safe transfer techniques, and isometric core activation. Depending on the surgeon's assessment of construct rigidity and patient bone quality, an external orthosis (e.g., a rigid Cervical Collar or a Thoracolumbosacral Orthosis [TLSO]) may be fitted prior to mobilization.
Phase II: Subacute and Healing Phase (2 to 6 weeks)
During this phase, patients are often discharged to a subacute rehabilitation facility or home with home health nursing. Intravenous antibiotics are continued; the standard duration of IV therapy is 6 to 8 weeks from the date of the definitive surgical debridement. Weekly laboratory monitoring of inflammatory markers (ESR and CRP), complete blood counts, and renal/hepatic function is mandatory to assess treatment response and monitor for antibiotic toxicity. CRP is the most responsive marker and should demonstrate a steady logarithmic decline; a plateau or secondary spike in CRP warrants immediate clinical and radiographic re-evaluation for recurrent
