Comprehensive Management of Spinal Infections: Nonoperative Protocols and Surgical Principles
Key Takeaway
The management of spinal infections requires a multidisciplinary approach, balancing targeted antimicrobial therapy with mechanical stabilization. While nonoperative treatment—comprising culture-specific intravenous antibiotics and orthotic immobilization—remains the primary modality, surgical intervention is mandated for progressive neurological deficits, epidural abscesses, or structural instability. Accurate diagnosis via MRI and image-guided biopsy is critical to optimizing clinical outcomes and preventing catastrophic complications such as paralysis or severe kyphotic deformity.
Comprehensive Introduction and Patho-Epidemiology
The traditional treatment of spinal infection has historically relied upon prolonged bed rest and rigid immobilization, paradigms established long before the advent of modern antimicrobial therapy and advanced spinal instrumentation. While these principles remain the foundational mainstay of conservative care, modern orthotic advancements have largely replaced the cumbersome, poorly tolerated body cast with removable, custom-molded thoracolumbosacral orthoses (TLSO) or body jackets in compliant patients. The cornerstone of contemporary nonoperative management relies intrinsically on targeted, culture-specific antimicrobial therapy. Empirical treatment must be strictly avoided until a definitive microbiological diagnosis is established via dual-site blood cultures or image-guided percutaneous biopsy, except in cases of fulminant sepsis, hemodynamic instability, or rapid neurological decline where withholding broad-spectrum coverage would prove life-threatening.
The vertebral column is involved in 0.15% to 3.9% of all osteomyelitis cases, representing a relatively rare but highly morbid clinical entity. Epidemiological data from landmark studies by Digby and Kersley indicate an overall incidence of approximately 1 in 250,000 individuals annually, though recent literature suggests this rate is climbing due to an aging population, the rising prevalence of diabetes mellitus, and the expanding use of immunosuppressive therapies. The demographic distribution skews heavily toward adult males, who account for 55% to 75% of the incidence, with a peak age of onset between 45 and 65 years. Staphylococcus aureus remains the most ubiquitous pathogen across all demographics, responsible for over half of all pyogenic vertebral osteomyelitis cases. However, specific patient populations exhibit unique microbiological profiles that demand high clinical suspicion; for instance, intravenous drug abusers (IVDU) have a markedly higher propensity for Pseudomonas aeruginosa and Serratia marcescens infections, while patients with indwelling genitourinary instrumentation frequently present with enteric gram-negative bacilli.
Pediatric discitis presents a fundamentally unique clinical entity compared to adult osteomyelitis, primarily due to the distinct vascular anatomy of the immature spine. It is classically characterized by a triad of low-grade fever, elevated erythrocyte sedimentation rate (ESR), and delayed disc space narrowing on plain radiographs, which typically only becomes visible 4 to 6 weeks post-onset. The average age of onset is 6 to 7 years. The clinical presentation is often insidious and challenging to diagnose; the child may exhibit a refusal to walk or crying during ambulation, loss of normal lumbar lordosis causing them to hold the spine rigidly erect, hamstring tightness, and vague abdominal pain. This abdominal referral pattern frequently leads to misdiagnosis in older children, mimicking appendicitis or other acute abdominal pathologies. Neurological deficits in the pediatric population are exceedingly rare but highly ominous, often signaling an expanding epidural abscess rather than simple discitis.
Unlike the pediatric spine, the adult intervertebral disc is entirely avascular. Consequently, primary hematogenous disc space infection is virtually impossible without preceding vertebral endplate osteomyelitis. True isolated disc space infections in adults are almost exclusively iatrogenic, resulting from direct penetrating trauma such as surgical discectomy, discography, or epidural injections. The incidence of postoperative discitis ranges from 1% to 2.8% following open disc surgery, and 0.5% to 1% following discography, with S. aureus again serving as the predominant organism. Diagnosis in the postoperative patient is frequently delayed due to the confounding presence of expected postoperative back pain. However, the persistence of severe, unrelenting muscle spasm, an inability to mobilize, and an ESR or C-reactive protein (CRP) that fails to normalize 4 to 6 weeks postoperatively are highly indicative of an iatrogenic infection requiring immediate advanced imaging.
Detailed Surgical Anatomy and Biomechanics
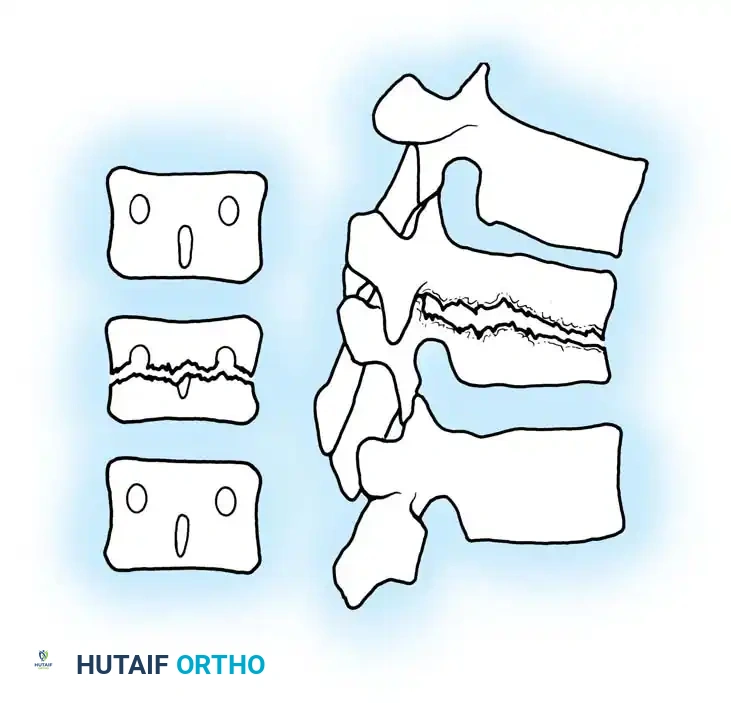
Understanding the pathophysiology and surgical management of spinal infections requires an intimate knowledge of the vascular anatomy and biomechanical environment of the spinal column. The arterial supply to the vertebral bodies is delivered via paired segmental arteries that branch from the aorta. These vessels bifurcate to supply the anterior and posterior portions of the vertebral body, terminating in a rich capillary network at the subchondral bone adjacent to the cartilaginous endplate. In adults, the intervertebral disc is the largest avascular structure in the human body, relying entirely on passive diffusion from these endplate capillary beds for nutrient exchange. When bacteremia occurs, sluggish blood flow in these terminal endplate capillary loops creates an ideal environment for bacterial seeding. Microthrombosis ensues, leading to localized avascular necrosis of the endplate, subsequent structural failure, and direct extension of the purulent exudate into the adjacent avascular disc space.
The venous drainage of the spine plays an equally critical role in the dissemination of infection, particularly via Batson’s valveless venous plexus. This intricate network of epidural and paravertebral veins communicates directly with the pelvic and systemic venous systems. Because these veins lack valves, intra-abdominal or intra-thoracic pressure variations can cause retrograde blood flow, providing a direct conduit for pelvic, genitourinary, or gastrointestinal pathogens to seed the spinal column. This anatomical quirk perfectly explains the high incidence of vertebral osteomyelitis following urological procedures. Furthermore, Hogan's seminal cryomicrotome studies demonstrated that the epidural fat and venous plexus are discontinuous and segmented, which somewhat compartmentalizes the infection longitudinally but forces expanding purulence to track along paths of least resistance, often resulting in ventral epidural abscesses that directly compress the thecal sac.
Selecting the appropriate antibiotic requires an understanding of the unique avascular microenvironment of the intervertebral disc and the surrounding necrotic bone. Specific antibiotics that demonstrate excellent serum bactericidal activity may completely fail to achieve minimum inhibitory concentrations (MIC) within the spinal axis. Eismont et al. demonstrated that 1 hour post-injection, cephalothin was undetectable in the intervertebral disc, penetrating to less than 4% of serum values. Conversely, clindamycin and tobramycin achieved greater than 50% of serum levels within the same timeframe, highlighting the critical need for selecting agents with high osseous and discal penetrance. Furthermore, Gibson et al. confirmed these pharmacokinetic limitations in pediatric populations undergoing anterior spinal surgery, noting that neither flucloxacillin nor cephradine was identifiable in the discs despite therapeutic serum concentrations in adjacent tissues.
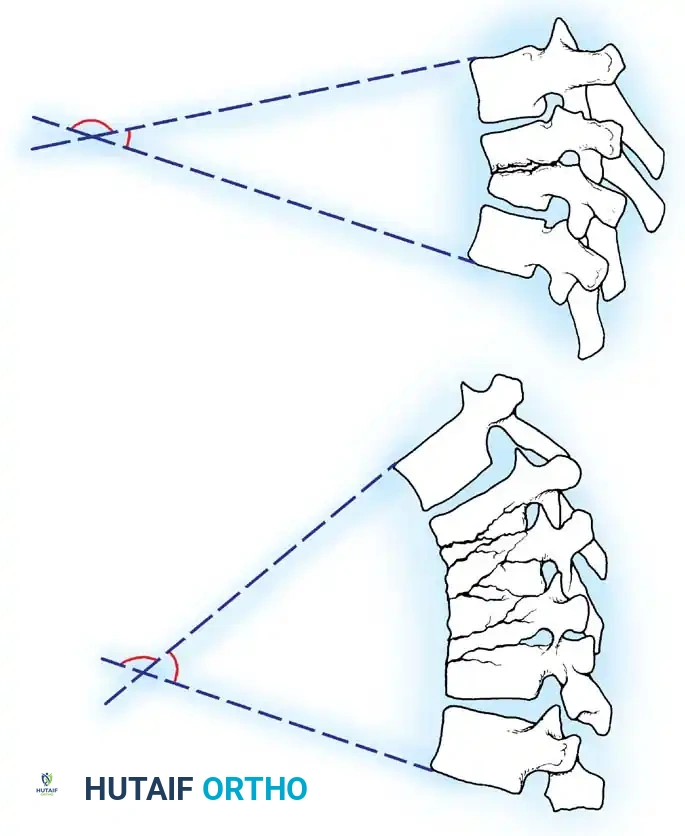
Biomechanically, the most devastating delayed complications of spinal infection include progressive kyphosis, paralysis, and myelopathy, which peak during the "soft bone" phase. This is the period when the active infection is microbiologically controlled by antibiotics, but the osteomyelitic bone remains structurally deficient and intensely hyperemic. During this vulnerable window, the healing process has not yet advanced to the point of solid neo-osteogenesis or spontaneous arthrodesis around the infected tissue. The anterior column, which normally bears 80% of the axial load, becomes mechanically incompetent. Without the rigid support of an intact vertebral body, the spine is highly susceptible to axial collapse and angular deformity, shifting the center of gravity anteriorly and exacerbating the kyphotic moment. This structural collapse can rapidly compress the anterior spinal cord, necessitating emergent biomechanical reconstruction.
Exhaustive Indications and Contraindications
The decision to transition a patient from nonoperative antimicrobial management to definitive surgical intervention is highly nuanced, requiring a meticulous synthesis of clinical trajectory, neurological status, and radiographic findings. While the natural history of most spinal infections involves symptomatic and radiographic resolution within 9 to 24 months of onset with conservative care alone, surgical intervention becomes the definitive standard of care when specific high-risk criteria are met. The overarching goals of surgical intervention are threefold: radical debridement of infected and necrotic tissue to reduce the bacterial bioburden, direct mechanical decompression of compromised neural elements, and the immediate restoration of biomechanical stability to the spinal column.
Savage et al. demonstrated that medical management (IV antibiotics and close observation) is a viable alternative for highly selected patients who present solely with axial back pain or whose neurological deficits have been completely stable for greater than 72 hours. However, any hint of progressive neurological deterioration mandates emergent surgical decompression. Heusner established the critical temporal window for intervention, demonstrating that early decompression—performed before the onset of profound paralysis or within 36 hours of initial motor weakness—yields a greater than 50% chance of complete neurological recovery. Delays beyond this window often result in irreversible ischemic damage to the spinal cord secondary to microvascular thrombosis and direct mechanical compression.
A critical surgical pitfall that must be vehemently avoided is the inappropriate use of isolated posterior laminectomy in the setting of anterior column disease. Laminectomy is strictly contraindicated in patients with ventral (anterior) osteomyelitis and secondary epidural abscess. Removing the posterior tension band (the lamina, spinous processes, and interspinous ligaments) in the presence of an existing anterior column defect will inevitably result in catastrophic iatrogenic destabilization. This leads to rapid kyphotic collapse, progressive anterior cord tethering, and acutely worsening neurological injury. The surgical approach must always be dictated by the anatomical location of the primary pathology.
| Clinical Scenario | Surgical Indication Status | Rationale / Contraindication Details |
|---|---|---|
| Progressive Neurological Deficit | Absolute Indication | Evolving myelopathy or cauda equina syndrome requires emergent decompression (<36 hours) to prevent irreversible ischemia and permanent paralysis. |
| Spinal Instability / Kyphosis | Absolute Indication | Anterior column collapse during the "soft bone" phase leads to progressive deformity and delayed neurological compromise; requires structural grafting. |
| Failure of Medical Management | Relative Indication | Persistent bacteremia or rising ESR/CRP despite 2-3 weeks of culture-directed IV antibiotics necessitates open debridement and removal of sequestered bone. |
| Ventral Epidural Abscess | Absolute Indication (Anterior) | Requires anterior corpectomy and decompression. Isolated posterior laminectomy is Strictly Contraindicated due to risk of catastrophic destabilization. |
| Intractable Axial Pain | Relative Indication | Severe, unrelenting pain secondary to mechanical collapse that fails rigid bracing and pharmacological management warrants stabilization. |
| Negative Percutaneous Biopsy | Relative Indication | When two successive CT-guided biopsies yield negative cultures in a deteriorating patient, open excisional biopsy is required for definitive diagnosis. |
Pre-Operative Planning, Templating, and Patient Positioning
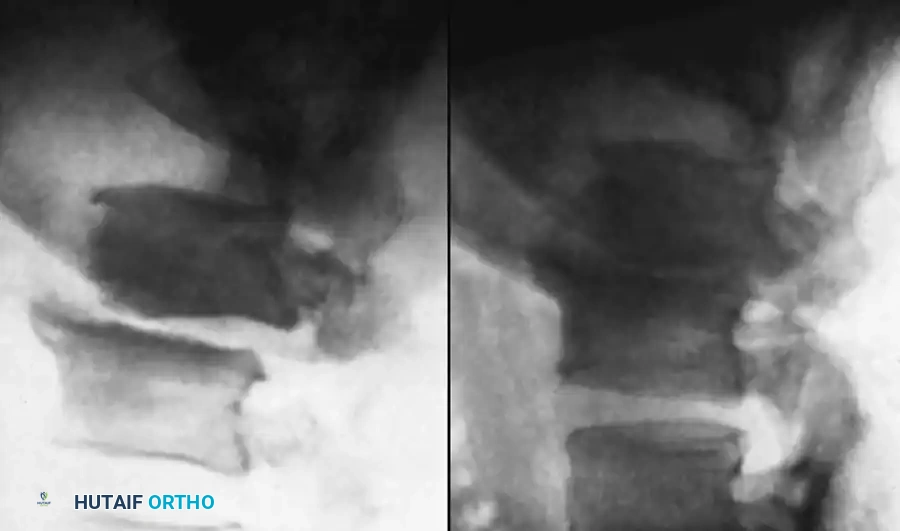
Thorough preoperative planning is the linchpin of successful surgical outcomes in the management of complex spinal infections. The diagnostic imaging workup must be exhaustive. Plain radiographs, while notoriously insensitive in the acute phase (often remaining normal for up to 4 weeks), are essential for establishing baseline sagittal and coronal alignment. Magnetic Resonance Imaging (MRI) with and without gadolinium contrast is the gold standard, offering the highest sensitivity and specificity. T1-weighted images typically demonstrate confluent decreased signal intensity in the involved vertebral bodies and disc space, while T2-weighted and STIR sequences reveal hyperintensity consistent with bone marrow edema and fluid collections. Gadolinium enhancement is critical for delineating the margins of epidural abscesses and differentiating phlegmon from drainable purulence. In patients with contraindications to MRI, a combination of fine-cut Computed Tomography (CT) with myelography and Technetium-99m/Gallium-67 bone scanning must be utilized to assess bone stock destruction and inflammatory extent.
Laboratory evaluation must include a complete blood count with differential, comprehensive metabolic panel, and serial inflammatory markers (ESR, CRP, and Procalcitonin). Blood cultures (minimum of two sets from distinct venipuncture sites) should be drawn during febrile spikes. It is imperative that all empirical antimicrobial therapy be suspended for at least 48 to 72 hours prior to any planned biopsy or surgical debridement, provided the patient is hemodynamically stable, to maximize the yield of intraoperative tissue cultures. Preoperative templating utilizing 3D CT reconstructions is mandatory for calculating the required dimensions of structural allografts or titanium mesh cages, anticipating the degree of necessary kyphosis correction, and selecting appropriate pedicle screw trajectories in potentially osteoporotic or compromised bone.
Patient positioning is entirely dependent on the selected surgical approach, which in turn is dictated by the anatomical location of the pathology. For isolated posterior epidural abscesses or supplemental posterior stabilization, the patient is positioned prone on a radiolucent Jackson spinal table. All bony prominences are meticulously padded, and the abdomen must hang free to decrease intra-abdominal pressure, thereby reducing epidural venous engorgement and intraoperative blood loss. The head is secured in a Mayfield skull clamp or a specialized prone headrest, ensuring the eyes are free from pressure to prevent ischemic optic neuropathy.
Conversely, for the anterior approach (corpectomy and strut grafting), the patient is placed in the lateral decubitus position. For thoracolumbar junction pathology, a left-sided approach is generally preferred to mobilize the aorta rather than the thin-walled, more easily injured inferior vena cava. An axillary roll is placed, and the patient is secured to the table with heavy adhesive tape and kidney rests. Fluoroscopy is utilized prior to incision to confirm orthogonal views and verify the exact spinal levels, as anatomical landmarks are frequently distorted by profound destructive changes and surrounding inflammatory phlegmon.
Step-by-Step Surgical Approach and Fixation Technique
The selection of the surgical approach is dictated entirely by the anatomical location of the pathology. Because abscesses arising from direct extension of vertebral osteomyelitis are almost universally located in the ventral (anterior) epidural space, directly compressing the thecal sac, the anterior approach is the workhorse of spinal infection surgery. For thoracolumbar lesions, a retroperitoneal or transthoracic approach is utilized depending on the exact level. Following the skin incision and division of the superficial musculature, the retroperitoneal space is entered, and the psoas muscle is carefully mobilized posteriorly. The segmental vessels overlying the infected vertebral bodies are identified, ligated with non-absorbable sutures or surgical clips, and divided. This allows the great vessels (aorta or vena cava) to be safely mobilized away from the infected spine.
Once the infected levels are exposed, a radical corpectomy is performed. The anterior longitudinal ligament is incised, and high-speed burrs and rongeurs are used to meticulously excise all necrotic bone, infected disc material, and epidural purulence. The debridement must be aggressive, extending back to bleeding, healthy, well-vascularized cancellous bone, much like the oncological principles of tumor resection. The posterior longitudinal ligament (PLL) is frequently necrotic and must be resected to ensure complete, unhindered decompression of the ventral thecal sac. Copious pulsatile lavage with liters of sterile saline is utilized to mechanically reduce the bacterial load. Intraoperative deep tissue cultures (minimum of three to five distinct samples) are sent for aerobic, anaerobic, mycobacterial, and fungal analysis before any irrigation is applied.
Following radical debridement, the massive anterior column defect must be reconstructed to restore height and sagittal alignment. This is achieved using a structural autograft (e.g., tricortical iliac crest, vascularized fibula) or, more commonly in modern practice, a titanium mesh cage packed with autologous bone graft or demineralized bone matrix. Titanium is highly resistant to bacterial biofilm formation and is safe to use in the setting of active infection. The cage is gently impacted into the defect under fluoroscopic guidance, ensuring it rests securely on the hard cortical endplates of the adjacent healthy vertebrae to prevent delayed subsidence. Anterior plating or supplemental posterior pedicle screw fixation is then applied to provide rigid biomechanical stability, which is an absolute prerequisite for infection eradication and successful arthrodesis.
In cases where the pathology is strictly confined to the dorsal elements (e.g., isolated dorsal epidural abscesses, isolated facet joint pyarthrosis), a posterior approach is indicated. A standard midline incision is made, and bilateral subperiosteal dissection exposes the posterior elements. A wide, multi-level laminectomy is performed to evacuate the purulent collection. If the posterior elements are structurally compromised by the infection or the extent of the decompression, pedicle screw instrumentation must be placed to bridge the defect. Screws are inserted into the healthy vertebrae at least one to two levels above and below the infection. Posterolateral bone grafting is performed, taking care to avoid placing graft directly over exposed dura. The wound is closed in multiple robust layers over subfascial drains to prevent postoperative hematoma formation.
Complications, Incidence Rates, and Salvage Management
The surgical management of spinal infections is fraught with potential complications, driven by the compromised systemic state of the host, the destructive nature of the pathogen, and the immense biomechanical forces acting on the reconstructed spine. Spinal epidural abscesses (SEA) carry exceptionally high morbidity and mortality rates, particularly in immunosuppressed cohorts, diabetics, and the elderly. Even with prompt surgical intervention, the systemic inflammatory response can precipitate multi-organ failure, acute respiratory distress syndrome (ARDS), and profound septic shock.
One of the most challenging local complications is reconstructive failure, primarily manifesting as cage subsidence or hardware pullout. This occurs because the adjacent vertebral endplates, while seemingly healthy during surgery, may harbor microscopic osteomyelitis or be profoundly osteoporotic due to regional hyperemia. When the titanium cage or strut graft subsides into the adjacent vertebral body, it results in a loss of sagittal correction, recurrent kyphosis, and potential delayed neurological compromise. Salvage management for severe subsidence typically requires a revision surgery via a posterior approach to extend the pedicle screw construct further proximally and distally, utilizing osteotomies if necessary to restore the sagittal balance.
Recurrence of infection is a persistent threat, particularly during periods of transient immunosuppression or if the initial debridement was inadequate. Persistent mechanical back pain, a new rise in acute-phase reactants, or the development of a draining sinus tract postoperatively should immediately prompt a comprehensive reevaluation. This may necessitate repeat imaging and a return to the operating room for an open biopsy to obtain fresh cultures, exchange of loose hardware, and aggressive re-debridement of sequestered, necrotic material.
| Complication | Estimated Incidence | Salvage Management & Clinical Strategy |
|---|---|---|
| Cage Subsidence / Graft Collapse | 10% - 25% | Close radiographic monitoring. If progressive kyphosis or new neuro deficits occur, requires posterior revision with extended pedicle screw fixation and possible osteotomy. |
| Recurrent / Persistent Infection | 5% - 15% | Requires repeat MRI with contrast. If fluid collection or osteolysis is present, emergent return to OR for radical washout, hardware retention (if stable) or exchange, and ID consultation for antibiotic adjustment. |
| Neurological Deterioration | 2% - 8% | Immediate postoperative MRI to rule out epidural hematoma or inadequate decompression. Emergent surgical re-exploration required if compressive lesion is identified. |
| Dural Tear / CSF Leak | 3% - 10% | Primary watertight repair with 4-0 Nurolon. Augmentation with fibrin glue or muscle patch. Postoperative flat bed rest for 48-72 hours. Subfascial drain on gravity (no suction). |
| Pseudarthrosis (Non-union) | 10% - 20% | Diagnosed via dynamic radiographs or fine-cut CT at 6-12 months. Requires revision surgery with decortication, robust autogenous bone grafting, and optimization of systemic host factors (e.g., smoking cessation). |
Phased Post-Operative Rehabilitation Protocols
Postoperative care following the surgical reconstruction of a spinal infection requires a highly coordinated, multidisciplinary approach integrating orthopedic surgery, infectious disease specialists, and physical medicine and rehabilitation. The rehabilitation protocol is strictly phased to balance the competing demands of mobilizing the patient to prevent medical complications (DVT, pneumonia) while protecting the fragile structural graft and internal fixation until solid arthrodesis is achieved.
Phase I: Acute Postoperative and Antimicrobial Phase (Weeks 0-6)
Immediately following surgery, the patient is typically managed in an intensive care or step-down unit. Intravenous (IV) antibiotics are initiated immediately postoperatively, tailored specifically to the intraoperative deep tissue cultures once finalized. This IV therapy is continued for a strict minimum of 6 weeks. Depending on the rigidity of the internal fixation and the patient's bone quality, patients may be mobilized out of bed on postoperative day 1 or 2. If the construct is deemed tenuous, mobilization is strictly performed in a custom-molded TLSO brace. Strict log-rolling precautions are enforced to prevent torsional stresses on the hardware. Aggressive deep vein thrombosis (DVT) prophylaxis is initiated once the risk of epidural hematoma has passed (typically 24-48 hours postoperatively). Serial inflammatory markers (ESR, CRP) are drawn weekly to monitor the biological response to the antimicrobial regimen.
Phase II: Transitional and Suppressive Phase (Weeks 6-12)
At the 6-week mark, follow-up upright radiographs are obtained to monitor for early graft subsidence, hardware failure, or progressive deformity. If the clinical response is favorable—defined by the resolution of constitutional symptoms, a healing surgical incision, and the normalization of acute-phase reactants (primarily the CRP, as the ESR may lag)—the patient is transitioned from intravenous to oral suppressive antimicrobial therapy. Collert established the paradigm that antimicrobial therapy must continue until the ESR returns to baseline; failure to do so is highly predictive of clinical relapse. During this phase, the patient is encouraged to increase ambulatory distance progressively. The TLSO brace is maintained whenever the patient is out of bed. Physical therapy focuses on isometric core strengthening and lower extremity conditioning, strictly avoiding active spinal flexion, extension, or rotation.
Phase III: Consolidation and Weaning Phase (Months 3-6+)
At 3 months postoperatively, a comprehensive radiographic evaluation is performed, often utilizing a fine-cut CT scan to assess for early trabecular bridging across the corpectomy defect or posterolateral gutters. If radiographic union is progressing satisfactorily and the patient remains clinically asymptomatic with normal inflammatory markers, the TLSO brace is gradually weaned over a 4-week period. Oral antibiotics may be discontinued at this stage, though some infectious disease protocols mandate 6 to 12 months of suppressive therapy for highly virulent organisms or in immunocompromised hosts. MRI is generally avoided during routine surveillance due to extensive hardware artifact and persistent, sterile postoperative edema, but it is reserved for cases of suspected clinical recurrence or the acute onset of new neurological symptoms. Heavy lifting and high-impact activities remain permanently restricted, but patients are guided back to functional independence and low-impact activities of daily living.
Summary of Landmark Literature and Clinical Guidelines
The contemporary management algorithms for spinal infections are built upon the foundational research of several pioneering surgeons and scientists. Understanding these landmark studies is critical for the academic orthopedic surgeon and serves as high-yield knowledge for board examinations.
Eismont et al. profoundly influenced the pharmacological approach to spinal infections by elucidating the pharmacokinetic limitations of antibiotic penetration into the avascular intervertebral disc. Their demonstration that cephalosporins exhibit poor discal penetrance compared to clindamycin and tobramycin fundamentally altered empirical prescribing habits. Furthermore, Eismont's epidemiological work highlighted that S. aureus infections carry the highest statistical risk of progressing to epidural extension and subsequent paralysis, mandating heightened vigilance in these cohorts. Gibson et al. expanded on this by confirming similar pharmacokinetic barriers in pediatric populations, emphasizing the need for sustained, high-dose intravenous therapy to achieve therapeutic MICs within the necrotic bone.
In the realm of pediatric discitis, the literature reflects a historical evolution from conservative isolation to active antimicrobial management. Spiegel et al. and Boston et al. historically recommended strict bed rest and immobilization without antibiotics, arguing that the condition in very young children (<6 years) was often a self-limiting or viral etiology. However, this paradigm was aggressively challenged by Wenger et al., who advocated for routine blood cultures followed by immediate IV antibiotics until the child is pain-free and ambulatory, followed by 3 weeks of oral therapy. Wenger's protocol has since become the modern standard of care, significantly reducing the duration of morbidity and the incidence of spontaneous interbody fusion.
Surgical timing and indications have been definitively shaped by the works of Heusner, Savage, and Feldenzer. Heusner established the critical 36-hour window for surgical decompression in the setting of spinal epidural abscesses, proving that intervention prior to profound motor weakness drastically improves neurological salvage rates. Savage et al. provided the counter-balance, demonstrating through rigorous clinical criteria that medical management alone is viable, but strictly limited to neurologically intact patients. Finally, Collert established the enduring clinical guideline that antimicrobial therapy must be dictated by the biological response of the host, specifically mandating that treatment continue until the erythrocyte sedimentation rate (ESR) normalizes, a paradigm that remains a cornerstone of postoperative surveillance today.
