Axial Skeleton Fractures: Understanding Spinal Cord Injury Risk
Key Takeaway
Discover the latest medical recommendations for Axial Skeleton Fractures: Understanding Spinal Cord Injury Risk. A spinal cord injury involves damage to the spinal cord, with approximately 12,000 new cases requiring treatment each year. Motor vehicle accidents account for roughly 50% of traumatic spinal cord injuries. Patients face a 17% mortality rate during initial hospitalization, and lifetime direct medical costs can range from $1.5 to $4.6 million, depending on injury severity.
Introduction and Epidemiology
Axial skeleton fractures encompass a broad spectrum of traumatic pathology, ranging from isolated, stable spinous process avulsions to highly unstable fracture-dislocations associated with catastrophic neurologic deficits. The management of these injuries requires a profound understanding of spinal biomechanics, neuroanatomy, and the pathophysiology of spinal cord injury.
Epidemiologically, the burden of traumatic spinal pathology is substantial. There are approximately 12,000 new spinal cord injuries requiring treatment each year in the United States. Injury to the vertebral column occurs much less frequently than injury to the appendicular skeleton, with vertebral column fractures accounting for approximately 6% of all skeletal fractures. It is a critical clinical axiom that 15% to 20% of vertebral fractures can occur at multiple noncontiguous levels, necessitating comprehensive imaging of the entire neuraxis in the setting of high-energy trauma.
Motor vehicle accidents remain the predominant etiology, accounting for approximately 50% of all traumatic spinal cord injuries. The demographic distribution is heavily skewed, with the ratio of male to female patients sustaining vertebral fractures being 4 to 1. The incidence of cervical spine fractures in the general trauma population is approximately 2% to 6%.
The systemic impact of a spinal cord injury is profound. In patients with an acute spinal cord injury, the overall mortality during the initial hospitalization is 17%. The long-term economic burden is staggering; the lifetime direct medical cost of a spinal cord injury for a person injured at age 25 years is estimated to be between $1.5 and $4.6 million, heavily dependent on the anatomic level and severity of the neurologic deficit.

Mechanism of Primary Injury
A long-standing and fundamental problem of classifying spinal injury based on presumed mechanism of injury is that the same mechanism can result in morphologically different patterns of injury. Conversely, similar morphologic patterns can be the result of different injury mechanisms. Furthermore, patterns of head deflection do not reliably predict spinal injury patterns. Several characteristics of the injury force determine the extent of neural tissue damage, including the rate of force application, the degree of neural tissue compression, and the duration of neural tissue compression.
Primary injury refers to the immediate physical tissue disruption caused by mechanical forces. This is categorized into four distinct mechanisms:
- Contusion: This sudden, brief compression by a displaced structure affects central tissues primarily and accounts for the majority of primary injuries. Consequently, it is responsible for the majority of neurologic deficits. Contusion injuries are potentially reversible, although irreversible neuronal death occurs along with vascular injury and intramedullary hemorrhage.
- Compression: Injury results from the decreased size of the spinal canal. It may occur with translation or angulation of the spinal column, as seen in burst fractures, fracture-dislocations, or epidural hematomas. Injury occurs via mechanical deformation interrupting axonal flow, and interruption of spinal vascularity resulting in ischemia of neurologic structures.
- Stretch: Injury results in longitudinal traction, as in the case of a flexion-distraction injury. Neural damage occurs as a result of capillary and axonal collapse secondary to tensile distortion.
- Laceration: This is caused by penetrating foreign bodies, missile fragments, or sharply displaced bone fragments transecting neural elements.
Surgical Anatomy and Biomechanics
A rigorous understanding of the spatial relationship between the osteoligamentous spinal column and the neural elements is paramount for safe surgical intervention.
Osteology and Canal Dimensions
The spinal cord occupies approximately 35% of the canal cross-sectional area at the level of the atlas (C1) and 50% of the canal in the lower cervical spine and thoracolumbar segments. The remainder of the canal is filled with epidural fat, cerebrospinal fluid, and dura mater. This anatomic variance explains why patients with C1 ring fractures (e.g., Jefferson fractures) often present without neurologic deficit due to the larger space available for the cord, whereas subaxial cervical trauma frequently results in cord compromise.
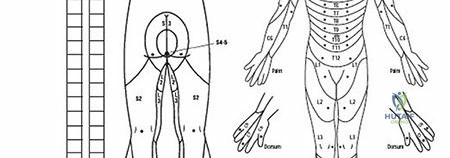
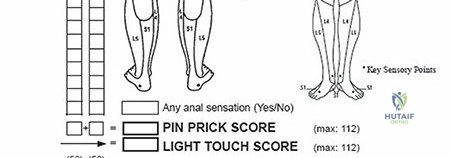
Neuroanatomy
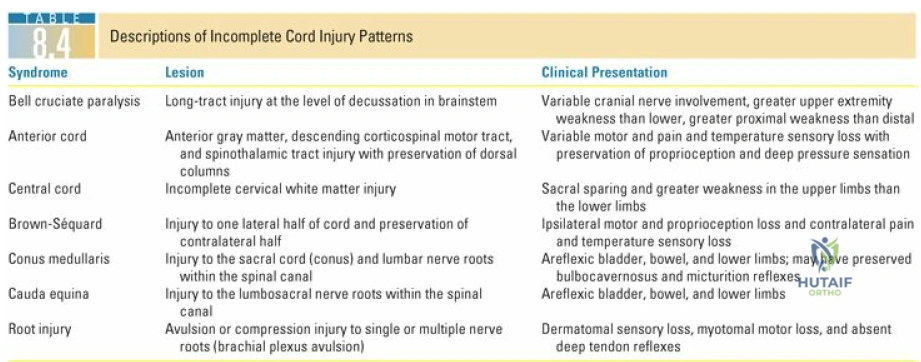
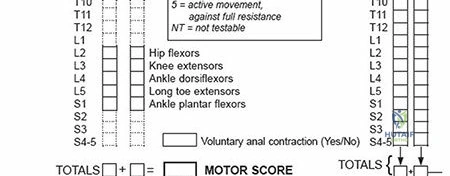
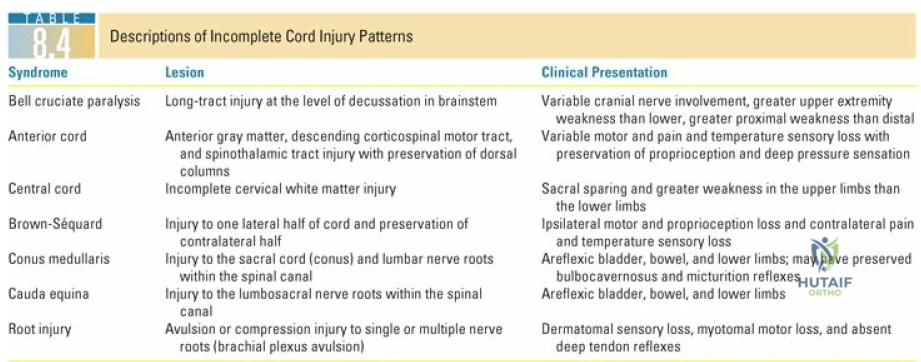
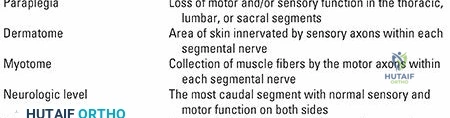
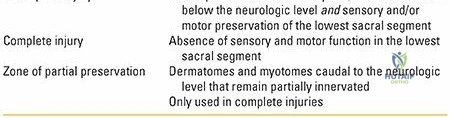
The conus medullaris represents the caudal termination of the spinal cord proper. It contains the sacral and coccygeal myelomeres and typically lies dorsal to the L1 vertebral body and the L1-L2 intervertebral disc. Injuries at this junctional zone present with a mixed upper and lower motor neuron clinical picture (Conus Medullaris Syndrome).
The cauda equina represents the motor and sensory roots of the lumbosacral myelomeres. These roots are less likely to be injured because they have more room in the lumbar canal and are not tethered to the same degree as the spinal cord. Furthermore, the motor nerve roots comprising the cauda equina are composed of lower motor neurons, which are intrinsically more resilient to mechanical ischemia and injury than the upper motor neurons of the brain and spinal cord.
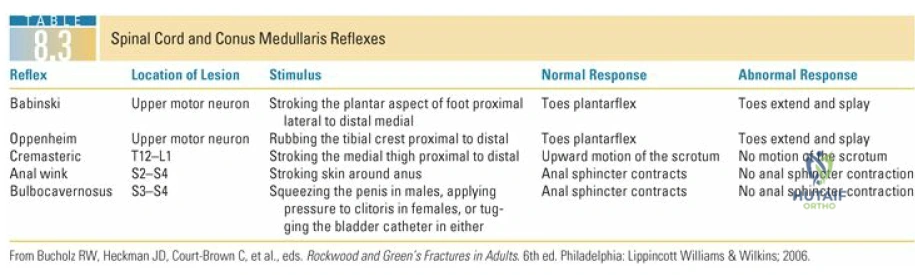
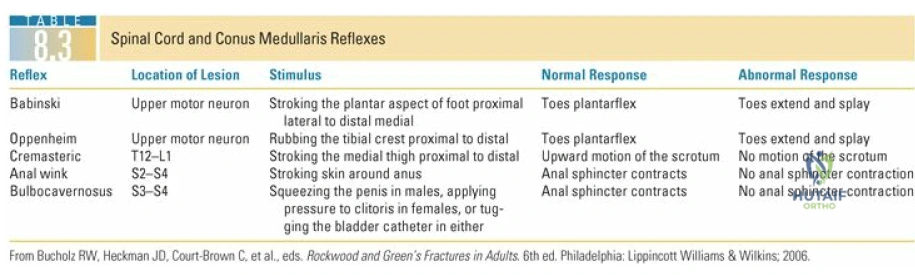
A reflex arc is a simple sensorimotor pathway that can function without using either ascending or descending white matter long tract axons. A spinal cord level that is anatomically and physiologically intact may demonstrate a functional reflex arc at that level despite complete dysfunction of the spinal cord cephalad to that level. This is clinically observed during the phase of spinal shock, where the bulbocavernosus reflex may return while long tract function remains absent.
Vascular Supply
The vascular supply to the spinal cord is a critical consideration during surgical exposure and decompression. The anterior two-thirds of the spinal cord is supplied by the single anterior spinal artery, which is formed by the union of branches from the vertebral arteries. It is highly dependent on radiculomedullary feeders, the most prominent being the Artery of Adamkiewicz (Arteria Radicularis Magna). This artery typically arises from the left side between T8 and L1 in 75% of individuals. Interruption of this supply during thoracolumbar approaches or due to fracture displacement can result in anterior cord syndrome. The posterior one-third of the cord is supplied by paired posterior spinal arteries, which have a more robust collateral network.
Indications and Contraindications
The decision to proceed with operative management of an axial skeleton fracture hinges on the assessment of mechanical instability, the presence of neurologic deficit, and the patient's physiologic ability to withstand surgery. Classification systems such as the Thoracolumbar Injury Classification and Severity Score and the Subaxial Injury Classification System are heavily utilized to guide these decisions.

Operative vs Non Operative Management
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Neurologic Status | Progressive neurologic deficit, incomplete spinal cord injury with active compression, epidural hematoma causing deficit. | Neurologically intact, complete spinal cord injury > 72 hours without mechanical instability (controversial). |
| Mechanical Stability | Disruption of the posterior ligamentous complex, translation/rotation injuries, highly comminuted burst fractures with kyphosis > 30 degrees. | Intact posterior ligamentous complex, isolated anterior column compression fractures, stable burst fractures without deficit. |
| Systemic Factors | Polytrauma requiring early mobilization, inability to tolerate prolonged bed rest or bracing. | Severe medical comorbidities precluding anesthesia, active systemic infection (relative contraindication for instrumentation). |
| Specific Fracture Patterns | Bilateral facet dislocations, unstable chance fractures, flexion-distraction injuries with ligamentous failure. | Isolated spinous/transverse process fractures, unilateral facet fractures without subluxation or radiculopathy. |
Pre Operative Planning and Patient Positioning
Pre-operative planning begins with the Advanced Trauma Life Support protocol. Hemodynamic optimization is critical; current guidelines recommend maintaining a Mean Arterial Pressure greater than 85 mmHg for seven days following an acute spinal cord injury to maximize spinal cord perfusion and mitigate secondary ischemic injury.
Advanced Imaging Protocols
Standard trauma protocols mandate thin-slice computed tomography of the entire spine. CT provides superior bony resolution to assess fracture morphology, facet subluxation, and pedicle anatomy for instrumentation planning. Magnetic Resonance Imaging is the gold standard for evaluating the neural elements, intervertebral discs, and the Posterior Ligamentous Complex. T2-weighted sequences are critical for identifying cord edema, contusion, epidural hematomas, and traumatic disc herniations that may influence the surgical approach (anterior vs. posterior).
Patient Positioning and Neuromonitoring
Positioning the spine-injured patient requires meticulous care to prevent exacerbation of neurologic deficits. For posterior approaches, the patient is typically placed prone on a radiolucent Jackson spinal table. This allows for the abdomen to hang free, reducing intra-abdominal pressure and thereby decreasing epidural venous engorgement and intraoperative bleeding.
In cases of cervical spine trauma, the head is often secured using Mayfield tongs or a rigid cranial fixation system. The neck must be maintained in a neutral alignment unless a specific reduction maneuver is planned. Awake fiberoptic intubation may be indicated for severe cervical stenosis or highly unstable upper cervical fractures.
Intraoperative neuromonitoring, utilizing Somatosensory Evoked Potentials and Motor Evoked Potentials, is standard of care. Baseline signals must be obtained prior to positioning and continuously monitored throughout the procedure, particularly during reduction maneuvers and instrumentation placement.
Detailed Surgical Approach and Technique
The surgical strategy for axial skeleton fractures generally involves decompression of the neural elements, reduction of the deformity, and rigid internal fixation to facilitate arthrodesis. The choice between an anterior, posterior, or combined approach depends on the location of the pathology, the mechanism of injury, and the surgeon's expertise.
Posterior Thoracolumbar Approach and Instrumentation
The standard posterior approach utilizes a midline longitudinal incision centered over the fractured levels. The length of the construct (short-segment vs. long-segment) is dictated by the fracture morphology and bone quality.
- Exposure: A subperiosteal dissection of the paraspinal musculature is performed off the spinous processes, laminae, and transverse processes. Care must be taken to preserve the facet capsules at the cranial and caudal levels adjacent to the planned fusion to prevent adjacent segment disease.
- Pedicle Screw Insertion: Using anatomic landmarks (the intersection of the pars interarticularis, the superior articular facet, and the transverse process), a high-speed burr or awl is used to decorticate the entry point. A pedicle probe is advanced down the cancellous channel of the pedicle into the vertebral body. The trajectory is confirmed using a ball-tip feeler to ensure no cortical breaches have occurred in the medial, lateral, superior, or inferior walls. The tract is tapped, and appropriately sized pedicle screws are inserted. Intraoperative fluoroscopy or stereotactic navigation is utilized to verify placement.
- Decompression: If central canal compromise is present (e.g., from a retropulsed burst fragment), a laminectomy is performed. The spinous process is removed with a Leksell rongeur. A high-speed matchstick burr is used to thin the lamina bilaterally at the junction of the medial facet. Kerrison rongeurs are then used to carefully resect the ligamentum flavum and complete the laminectomy, exposing the dura.
- Reduction and Fixation: Titanium or cobalt-chrome rods are contoured to match the desired sagittal alignment. The rods are seated into the pedicle screw tulips. Reduction maneuvers can be performed using specialized instrumentation (e.g., rod persuaders, in-situ benders) to restore vertebral body height and correct kyphosis.
- Arthrodesis: The transverse processes and lateral gutters are decorticated using a burr. Autograft (locally harvested bone from the laminectomy) and allograft are packed into the posterolateral gutters to promote a robust fusion mass.
Anterior Cervical Approach
For subaxial cervical spine fractures with anterior cord compression (e.g., traumatic disc herniation or teardrop fractures), an Anterior Cervical Discectomy and Fusion or anterior corpectomy is often indicated.
The approach utilizes a transverse or longitudinal incision in the anterior neck, utilizing the internervous plane between the carotid sheath (sternocleidomastoid) laterally and the visceral axis (trachea, esophagus) medially. The longus colli muscles are elevated laterally to expose the vertebral bodies. Following discectomy or corpectomy to decompress the cord, a structural allograft or titanium cage is placed, followed by an anterior cervical plate and screws to provide immediate stability.
Complications and Management
Surgical management of axial skeleton fractures carries a significant risk profile. Complications can be broadly categorized into intraoperative, early postoperative, and late postoperative events.
Common Surgical Complications
| Complication | Incidence | Etiology and Risk Factors | Salvage Strategy and Management |
|---|---|---|---|
| Incidental Durotomy | 4% - 14% | Adherent ligamentum flavum, sharp bone spicules, technical error with Kerrison rongeur. | Primary repair with 4-0 or 5-0 non-absorbable suture. Augmentation with dural sealants or muscle/fascia patch. Bed rest for 24-48 hours post-op. Subfascial drain placement. |
| Neurologic Deterioration | 1% - 3% | Epidural hematoma, over-distraction, malpositioned hardware, intraoperative hypotension. | Immediate assessment of hardware via CT. Return to OR for evacuation of hematoma or hardware revision. Maintenance of MAP > 85 mmHg. |
| Surgical Site Infection | 2% - 10% | Prolonged operative time, diabetes, obesity, malnutrition, posterior trauma approaches. | Aggressive surgical debridement, copious irrigation, retention of hardware if stable. Targeted intravenous antibiotics based on intraoperative cultures. |
| Hardware Failure | 5% - 15% | Poor bone quality (osteoporosis), pseudoarthrosis, inadequate construct length, non-compliance. | Revision surgery with extension of fusion levels, larger diameter screws, cement augmentation (PMMA), or combined anterior-posterior approaches. |
| Post-Traumatic Syringomyelia | 1% - 4% | Alteration of CSF dynamics following primary cord trauma and arachnoid scarring. | Serial MRI monitoring. Surgical detethering or placement of a syringosubarachnoid or syringopleural shunt if progressive neurologic deficit occurs. |
Post Operative Rehabilitation Protocols
The postoperative phase is critical for maximizing neurologic recovery and preventing systemic complications associated with immobility. Patients are typically managed in a surgical intensive care unit immediately following the procedure.
Hemodynamic and Medical Management
Strict adherence to hemodynamic parameters is maintained, continuing the MAP > 85 mmHg protocol for a total of seven days post-injury. Venous thromboembolism prophylaxis is paramount, as spinal cord injury patients are at the highest risk for deep vein thrombosis and pulmonary embolism. Chemical prophylaxis (e.g., low molecular weight heparin) should be initiated within 24 to 72 hours postoperatively, provided there is no evidence of expanding epidural hematoma.
Mobilization and Orthoses
Early mobilization is encouraged once spinal stability is achieved surgically. Depending on the bone quality and construct rigidity, patients may be mobilized with or without an orthosis. Cervical fractures may require a rigid collar (e.g., Aspen or Miami J), while thoracolumbar injuries may be managed with a Thoracolumbosacral Orthosis. The primary role of the orthosis postoperatively is to restrict gross truncal motion and provide proprioceptive feedback, rather than to provide absolute mechanical immobilization.
Autonomic Dysreflexia
In patients with spinal cord injuries at or above the T6 level, autonomic dysreflexia is a life-threatening complication that can occur during the rehabilitation phase. It is characterized by an uncoordinated sympathetic response to a noxious stimulus below the level of injury (e.g., distended bladder, bowel impaction). Clinical presentation includes severe hypertension, pounding headache, and bradycardia. Immediate management involves placing the patient in an upright position to induce orthostatic hypotension, identifying and removing the noxious stimulus, and administering rapid-acting antihypertensives if necessary.
Summary of Key Literature and Guidelines
Evidence-based management of axial skeleton fractures and spinal cord injury is continuously evolving. Several landmark studies and societal guidelines dictate current clinical practice.
Timing of Surgical Decompression
The Surgical Timing in Acute Spinal Cord Injury Study was a pivotal prospective, multicenter study that evaluated the impact of early versus late decompression. The STASCIS trial demonstrated that early surgical decompression (defined as less than 24 hours post-injury) in patients with cervical spinal cord injury resulted in a significantly higher rate of improvement in ASIA Impairment Scale grades at 6 months compared to late decompression. This has shifted the global paradigm toward emergent or urgent decompression for incomplete spinal cord injuries.
The Role of Corticosteroids
The use of high-dose methylprednisolone in acute spinal cord injury remains one of the most controversial topics in spine surgery. The National Acute Spinal Cord Injury Studies (NASCIS II and III) initially suggested a marginal neurologic benefit if steroids were administered within 8 hours of injury. However, subsequent independent analyses and systematic reviews highlighted severe methodological flaws and a high incidence of severe adverse events, including sepsis, pneumonia, and gastrointestinal hemorrhage. Current guidelines from the American Association of Neurological Surgeons and the Congress of Neurological Surgeons state that high-dose steroids are not recommended as a standard of care, but may be considered as a treatment option in highly selected patients after a thorough discussion of the risks.
Hemodynamic Guidelines
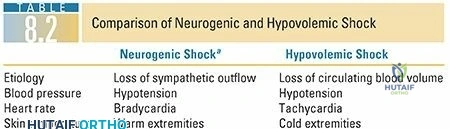
Current AANS/CNS guidelines strongly support the avoidance of hypotension (systolic blood pressure < 90 mmHg) and advocate for the maintenance of MAP > 85 mmHg for up to 7 days following acute spinal cord injury. This is based on robust preclinical and clinical data demonstrating that the injured spinal cord loses its autoregulatory capacity, rendering it highly susceptible to secondary ischemic cascades. Vasopressors, such as norepinephrine or dopamine, are frequently required to maintain these parameters in the setting of neurogenic shock.
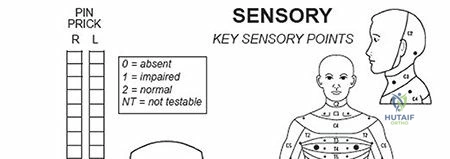
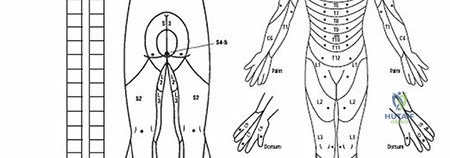
Clinical & Radiographic Imaging