Unraveling Thoracolumbar Spine Injuries: What You Must Know
Key Takeaway
We review everything you need to understand about Unraveling Thoracolumbar Spine Injuries: What You Must Know. Thoracolumbar spine injuries involve the transition zone of 12 thoracic and 5 lumbar vertebrae. These injuries account for 90% of vertebral fractures, frequently occurring in males aged 30-39, often due to motor vehicle trauma or falls. Neurologic injury complicates 15-20% of cases, particularly within the T2-T10 region, which is especially vulnerable due to its anatomical and circulatory characteristics.
Introduction and Epidemiology
Thoracolumbar spine injuries represent a significant source of morbidity and mortality, demanding a rigorous understanding of spinal biomechanics, precise neurologic assessment, and advanced surgical execution. The epidemiology of these injuries demonstrates a distinct bimodal distribution. High-energy trauma, such as motor vehicle collisions and falls from significant heights, accounts for approximately 65% of thoracolumbar fractures. The remainder of high-energy injuries are typically sustained during athletic participation or interpersonal assault. In this high-energy cohort, thoracolumbar trauma occurs most frequently in male patients between 30 and 39 years of age.

Conversely, low-energy mechanisms primarily affect the elderly population, driven by decreased bone mineral density. Most isolated thoracic and lumbar spine fractures are related to osteoporosis and involve minimal or no trauma. The sheer volume of osteoporotic fractures is staggering; osteoporosis accounts for approximately 750,000 vertebral fractures annually in the United States, far outnumbering the 15,000 trauma-related thoracic and lumbar spine fractures.
Topographically, the thoracolumbar region is the epicenter of spinal trauma. Ninety percent of all vertebral fractures occur in the thoracolumbar spine, and 60% of these fractures specifically localize to the transition zone between the T11 and L2 vertebral levels. Neurologic injury complicates 15% to 20% of all fractures at the thoracolumbar level, necessitating urgent evaluation and often surgical intervention to decompress neural elements and stabilize the spinal column.
Surgical Anatomy and Biomechanics
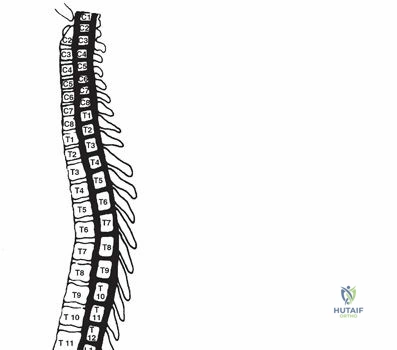
A profound comprehension of the osseous, ligamentous, and neurologic anatomy of the thoracolumbar spine is non-negotiable for the operating surgeon. The thoracolumbar spine consists of 12 thoracic vertebrae and 5 lumbar vertebrae. Biomechanically, the thoracic level is natively kyphotic, while the lumbar region is lordotic. The thoracolumbar junction (T11-L2) serves as a critical transition zone between the rigid thoracic spine and the highly mobile lumbar spine, rendering it exceptionally prone to mechanical failure under axial and torsional loads.

Osseous and Articular Biomechanics
The thoracic spine is significantly stiffer than the lumbar spine in flexion-extension and lateral bending. This rigidity is primarily a reflection of the restraining effect of the rib cage, the sternum, and the thinner intervertebral discs inherent to the thoracic spine. However, axial rotation is greater in the thoracic spine, achieving a maximum arc of motion at the T8-T9 level. The biomechanical explanation for this disparity lies in the spatial orientation of the facet joints. Thoracic facets are oriented in the coronal plane, facilitating rotation, whereas lumbar facets are oriented in the sagittal plane. This sagittal orientation limits the rotation arc to approximately 10 degrees for the entire lumbar spine, contrasted sharply against the 75 degrees of rotation permitted in the thoracic spine.
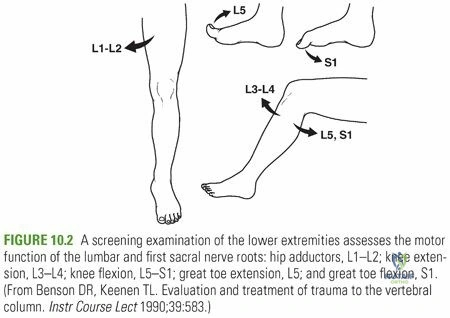
Neurologic Anatomy and Vulnerability
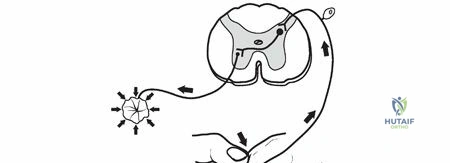
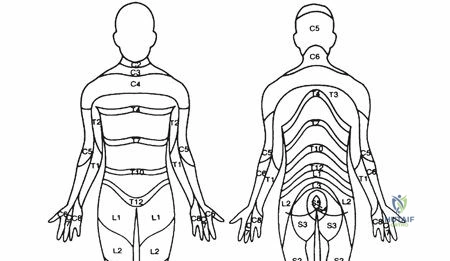
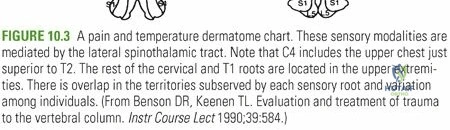
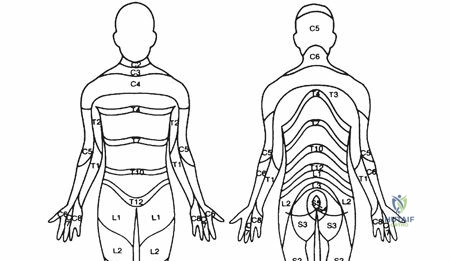
The spatial relationship between the spinal canal and the spinal cord dictates the pattern of neurologic deficits following trauma. The ratio of the spinal canal cross-sectional area to the spinal cord dimensions is smallest in the T2-T10 region. Consequently, this region is highly intolerant of space-occupying lesions, such as retropulsed bone fragments or epidural hematomas, making it highly prone to catastrophic neurologic injury after trauma. Neurologic deficits secondary to skeletal injury from the T1 through T10 levels are frequently complete deficits, primarily related to direct spinal cord injury with varying levels of root injury.
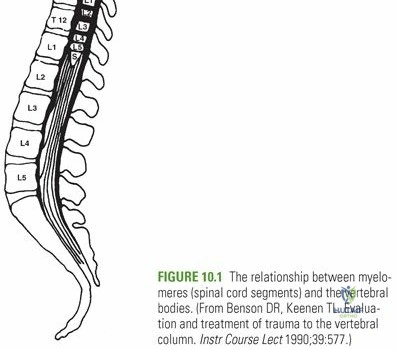
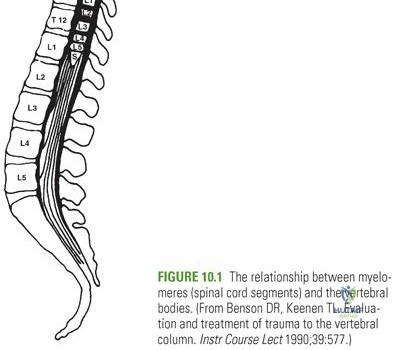
The conus medullaris typically terminates at the L1-L2 disc space. The cauda equina, which comprises the motor and sensory roots of the lumbosacral myelomeres, lies caudal to the conus.
Because the spinal cord ends at this transition zone, the proportion of root injury increases with more caudal injuries. Skeletal injuries caudal to L1 cause exclusively root (lower motor neuron) injuries, which generally carry a more favorable prognosis for recovery compared to central cord injuries. Furthermore, the corticospinal tracts demonstrate distinct polarity within the cord parenchyma, with cervical fibers distributed centrally and sacral fibers located peripherally.
Vascular Watershed Zones
Vascular supply to the spinal cord is a critical consideration during both the initial trauma resuscitation and subsequent surgical intervention. The region between T2 and T10 represents a circulatory watershed area. It derives its proximal blood supply from antegrade vessels originating in the upper thoracic spine, and its distal supply from retrograde flow via the great anterior radiculomedullary artery (Artery of Adamkiewicz). This critical vessel is variably located between T9 and L2, most commonly on the left side. Disruption of this vessel, or systemic hypotension during surgery, can lead to devastating anterior spinal artery syndrome.
Indications and Contraindications
Decision-making in thoracolumbar trauma relies heavily on standardized classification systems, primarily the Thoracolumbar Injury Classification and Severity Score and the AOSpine Thoracolumbar Spine Injury Classification System. These systems evaluate injury morphology, the integrity of the posterior ligamentous complex, and the patient's neurologic status to guide operative versus non-operative management.
Operative Versus Non Operative Management Parameters
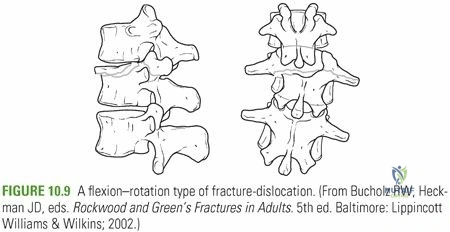
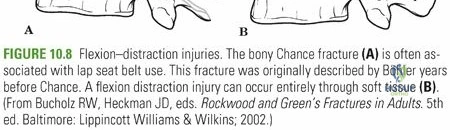
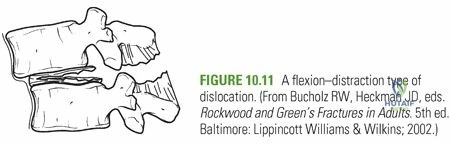
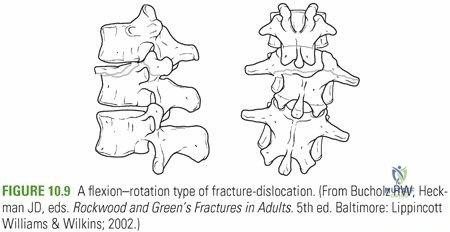
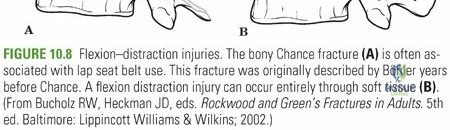
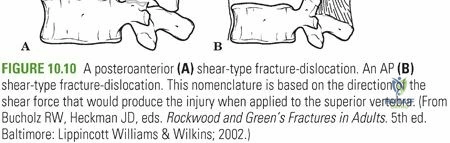
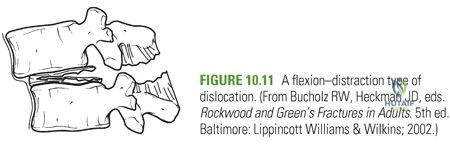
Surgical intervention is generally indicated for patients with progressive neurologic deficits, unstable fracture patterns (such as flexion-distraction injuries or fracture-dislocations), and significant kyphotic deformity that threatens the biomechanical integrity of the spinal axis.
| Clinical Parameter | Non Operative Management | Operative Management |
|---|---|---|
| TLICS Score | 3 or less | 5 or greater (4 is indeterminate) |
| Neurologic Status | Intact | Progressive deficit or incomplete cord syndrome |
| Posterior Ligamentous Complex | Intact | Disrupted (widened interspinous distance) |
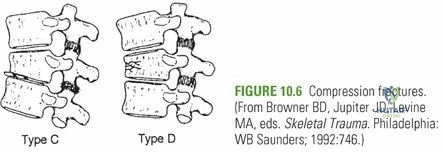
| Morphology | Compression fracture, stable burst | Translation, rotation, distraction, unstable burst |
| Kyphotic Deformity | Less than 20 degrees | Greater than 20 to 30 degrees |
| Canal Compromise | Minimal, no neuro deficit | Greater than 50 percent with radiculopathy/myelopathy |
Absolute and Relative Contraindications
Absolute contraindications to surgical intervention include a medically unstable polytrauma patient who cannot tolerate anesthesia (requiring damage control orthopedics), or a patient with an unrecoverable, prolonged complete spinal cord injury where surgery would not alter the neurologic outcome and only add surgical morbidity, unless stabilization is required for nursing care and mobilization. Relative contraindications include severe osteoporosis where hardware purchase is highly questionable, though modern techniques utilizing cement augmentation have mitigated this risk.
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is paramount. High-resolution computed tomography of the entire spine is mandatory to delineate fracture morphology, assess pedicle dimensions for instrumentation, and rule out non-contiguous injuries, which occur in up to 20% of patients. Magnetic resonance imaging is indicated to evaluate the integrity of the posterior ligamentous complex, intervertebral discs, and the presence of epidural hematoma or cord contusion.
Patient Positioning and Intraoperative Monitoring
For the standard posterior approach, the patient is positioned prone on a radiolucent Jackson spinal table. This positioning allows the abdomen to hang free, reducing intra-abdominal pressure and consequently decreasing epidural venous engorgement and intraoperative blood loss. Careful padding of all bony prominences is required to prevent pressure necrosis, and the eyes must be checked to ensure no external pressure is applied, mitigating the risk of ischemic optic neuropathy.
Intraoperative neuromonitoring, including somatosensory evoked potentials and motor evoked potentials, is standard of care during the reduction and instrumentation of thoracolumbar fractures. Baseline signals must be obtained prior to positioning and monitored continuously throughout the procedure.
Detailed Surgical Approach and Technique
The posterior approach remains the workhorse for the stabilization of thoracolumbar fractures, allowing for direct decompression, reduction of deformity, and robust multi-segmental fixation.
Exposure and Dissection
A standard midline longitudinal incision is utilized, centered over the fractured vertebra and extending proximally and distally to incorporate the planned instrumented levels. The fascia is incised precisely in the midline over the spinous processes. Subperiosteal dissection of the paraspinal musculature is performed bilaterally using electrocautery and Cobb elevators. The dissection must be meticulous, staying strictly subperiosteal to minimize bleeding, and is carried laterally to the tips of the transverse processes in the thoracic spine and the lateral border of the pars interarticularis and transverse processes in the lumbar spine.
Pedicle Screw Instrumentation
Accurate pedicle screw placement is the cornerstone of posterior stabilization. In the thoracic spine, the starting point is typically at the intersection of the bisected transverse process and the lateral border of the superior articular facet. In the lumbar spine, the starting point is at the intersection of the pars interarticularis, the midpoint of the transverse process, and the lateral border of the superior articular process (the mamillary process).
A high-speed burr or rongeur is used to decorticate the starting point. A pedicle probe (gearshift) is advanced through the pedicle into the vertebral body. The trajectory in the sagittal plane should parallel the superior endplate, while the axial trajectory converges toward the midline, with convergence angles increasing from the upper thoracic spine down to the lumbar spine.
The pedicle tract is palpated with a ball-tipped sound to ensure five distinct bony walls (medial, lateral, superior, inferior, and anterior). Tapping may be performed, followed by the insertion of appropriately sized pedicle screws. Fluoroscopy, or increasingly, intraoperative stereotactic navigation, is utilized to confirm accurate hardware placement.
Decompression and Reduction Techniques
If a neurologic deficit is present secondary to anterior column retropulsion, a direct or indirect decompression is required. Indirect decompression relies on ligamentotaxis—applying distraction across the construct to pull retropulsed bone fragments back into the vertebral body via the intact posterior longitudinal ligament. This is most effective within the first 48 hours post-injury.
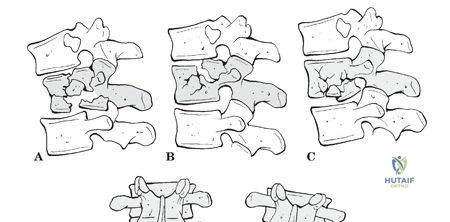
If ligamentotaxis is insufficient or the posterior longitudinal ligament is disrupted, a direct decompression is necessary. This may involve a wide laminectomy and a transpedicular or costotransversectomy approach to impact the retropulsed fragments anteriorly into the vertebral body using reverse angle curettes or specialized impaction tools.
Following decompression, pre-contoured rods are seated into the screw heads. Reduction of kyphotic deformity is achieved through a combination of patient positioning, cantilever reduction techniques using the rods, and in situ compression or distraction. Once satisfactory alignment is confirmed radiographically, set plugs are definitively torqued, and a posterolateral arthrodesis is performed using local autograft and allograft extenders over the decorticated transverse processes and pars interarticularis.
Complications and Management
Surgical management of thoracolumbar trauma carries inherent risks. A systematic approach to complication avoidance and management is essential for optimizing patient outcomes.

Recognized Surgical Complications
Complications can be broadly categorized into neurologic, mechanical, and infectious etiologies. Neurologic deterioration postoperatively demands immediate investigation with MRI to rule out epidural hematoma or iatrogenic hardware malposition. Mechanical failures often result from inadequate construct length, failure to recognize anterior column instability, or profound osteoporosis.
| Complication | Estimated Incidence | Prevention and Salvage Strategy |
|---|---|---|
| Infection (Surgical Site) | 2 to 5 percent | Meticulous hemostasis, prophylactic antibiotics. Salvage: I&D, hardware retention if stable, targeted IV antibiotics. |
| Dural Tear | 3 to 10 percent | Careful dissection around lamina. Salvage: Primary repair with 4-0 Nurolon, fibrin sealant, bed rest. |
| Hardware Failure or Pullout | 2 to 8 percent | Use of cement augmentation in osteoporotic bone, longer construct lengths. Salvage: Revision with extension of fusion, larger diameter screws. |
| Neurologic Deficit (Iatrogenic) | 1 to 3 percent | Intraoperative neuromonitoring, precise screw trajectory. Salvage: Immediate hardware removal/repositioning, high-dose steroids (controversial). |
| Pseudarthrosis | 5 to 15 percent | Meticulous decortication, adequate bone grafting. Salvage: Revision arthrodesis, potentially adding anterior column support. |
Dural tears encountered during decompression must be addressed meticulously. Primary watertight repair is the gold standard, often supplemented with dural sealants or fascial onlay grafts. Postoperatively, the patient may be kept flat to decrease hydrostatic pressure on the repair, though protocols vary based on the integrity of the closure.
Post Operative Rehabilitation Protocols
The immediate postoperative phase focuses on hemodynamic stability, pain control, and early mobilization to prevent deep vein thrombosis, pulmonary embolism, and atelectasis. Modern rigid pedicle screw constructs generally negate the need for postoperative bracing (Thoracolumbosacral orthosis), allowing for immediate mobilization out of bed.
Physical and occupational therapy are initiated on postoperative day one. Patients are instructed on strict spinal precautions, commonly referred to as the "BLT" restrictions: no bending, lifting (greater than 10 pounds), or twisting. These precautions are typically maintained for 6 to 12 weeks until radiographic evidence of arthrodesis is observed.
In patients with complete or incomplete spinal cord injuries, rehabilitation is significantly more complex, requiring transfer to a specialized spinal cord injury unit. Management of neurogenic bowel and bladder, prevention of decubitus ulcers, and aggressive physical therapy for spasticity and contracture prevention become the primary focus of the multidisciplinary team.
Summary of Key Literature and Guidelines
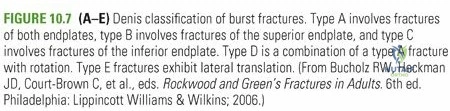
The management of thoracolumbar trauma is heavily guided by landmark literature and evolving society guidelines. Historically, the Denis three-column theory provided the foundational understanding of spinal stability, dictating that disruption of two of the three columns resulted in mechanical instability.
However, the paradigm shifted significantly with the introduction of the Thoracolumbar Injury Classification and Severity Score by Vaccaro et al. This system integrated neurologic status and the integrity of the posterior ligamentous complex, providing a more comprehensive, outcome-driven algorithm for surgical decision-making.
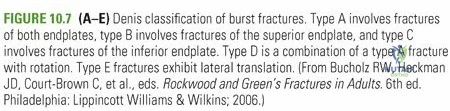
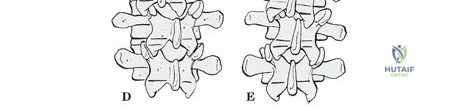
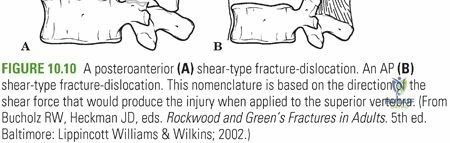
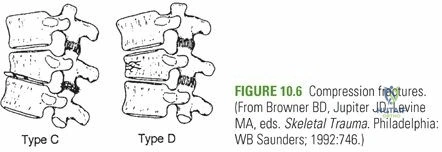
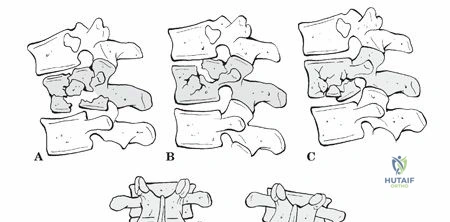
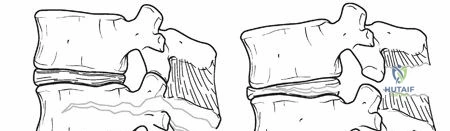
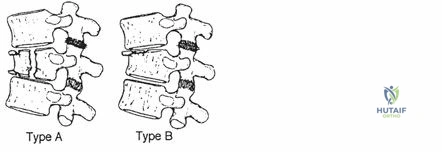
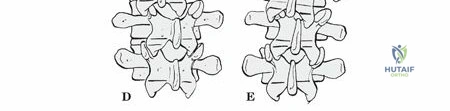
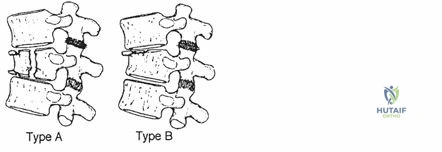
More recently, the AOSpine Thoracolumbar Spine Injury Classification System was developed to create a universally accepted nomenclature, categorizing injuries into Type A (compression), Type B (tension band disruption), and Type C (translation/displacement).
Regarding the timing of surgical intervention, the Surgical Timing in Acute Spinal Cord Injury Study (STASCIS) provided compelling evidence that early decompression (less than 24 hours post-injury) in the setting of acute spinal cord injury is associated with improved neurologic outcomes compared to delayed decompression. These guidelines underscore the necessity for rapid transport, efficient imaging, and expedited surgical care in the management of thoracolumbar spine injuries.
Clinical & Radiographic Imaging