Posterolateral Thoracolumbar Fusion with Instrumentation: An Intraoperative Masterclass

Key Takeaway
This masterclass guides you through posterolateral thoracolumbar fusion, emphasizing meticulous anatomy, precise pedicle screw placement, and comprehensive instrumentation. We cover preoperative planning, patient positioning, step-by-step intraoperative execution, and critical pearls for successful spinal stabilization and optimal patient outcomes. Learn to navigate complex spinal pathologies with confidence.
Comprehensive Introduction and Patho-Epidemiology
Welcome to the operating theater, colleagues. Today, we embark on a detailed exploration of posterolateral thoracolumbar fusion with instrumentation—a foundational, workhorse procedure in the armamentarium of the modern orthopedic spine surgeon. This is not merely an exercise in carpentry; it is a profound biomechanical reconstruction that demands an intimate understanding of spinal osteology, neurovascular proximity, and the physiological principles of arthrodesis. The evolution of this procedure, from the uninstrumented in situ fusions of the early 20th century to the highly precise, image-guided pedicle screw constructs of today, represents one of the most significant advancements in orthopedic surgery. As we scrub in, recognize that every trajectory chosen and every decortication performed has lasting implications for the patient's functional longevity and sagittal balance.
The patho-epidemiology necessitating thoracolumbar fusion is vast and heterogeneous, encompassing degenerative disc disease, isthmic and degenerative spondylolisthesis, traumatic burst fractures, neoplastic destruction, and complex spinal deformities. Degenerative lumbar spondylosis, the most common indication, affects a massive demographic, with symptomatic instability often leading to debilitating mechanical back pain and radiculopathy. The biomechanical rationale for intervention is straightforward: to eliminate pathologic segmental motion, decompress neural elements (when combined with laminectomy), and restore physiological lordosis. However, achieving these goals requires navigating a complex biological environment where successful bony union is the ultimate arbiter of long-term success.
Historically, the introduction of pedicle screw fixation revolutionized our approach. Before pedicle screws, constructs relied on sublaminar wires or hooks, which offered inferior three-column biomechanical control and carried higher risks of neurologic injury during placement. The pedicle, functioning as the anatomical bridge between the anterior and posterior columns, provides the most robust anchor point in the vertebral segment. By rigidly locking the motion segment, pedicle screw instrumentation decreases the micromotion at the fusion interface, thereby dramatically increasing the fusion rate compared to uninstrumented or hook-based techniques.
As we progress through this masterclass, we will systematically deconstruct the procedure. We will analyze the nuanced morphology of the pedicle cylinder across the thoracic and lumbar spine, discuss the critical importance of preoperative templating, and detail the step-by-step execution of the surgical approach, pedicle cannulation, and fusion bed preparation. We will also address the harsh realities of intraoperative complications and the rigorous postoperative rehabilitation required to maximize our surgical outcomes. Let this serve as your definitive guide to mastering the posterolateral thoracolumbar fusion.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel is handed to you, a profound, three-dimensional understanding of regional anatomy is paramount. The thoracolumbar spine is a transition zone fraught with unique biomechanical and anatomical challenges. We are bridging the rigid, kyphotic thoracic spine to the mobile, lordotic lumbar spine, necessitating an acute awareness of varying pedicle morphologies and adjacent neurovascular structures.
Thoracolumbar Osteology and the Pedicle Cylinder
The pedicle is our primary conduit for fixation, a dense cortical cylinder enveloping a cancellous core. Its morphology dictates our screw diameter, length, and trajectory. In the thoracic spine (T1-T12), pedicles are generally smaller and more ovoid than their lumbar counterparts. They are narrowest in the mediolateral dimension, particularly in the midthoracic region from T3 to T5, with T5 often representing the narrowest point (mean width approximately 4.5 mm). This anatomical bottleneck demands extreme precision, as a screw diameter exceeding the pedicle width guarantees a cortical breach. From this nadir, pedicle width gradually increases both cephalad towards T1 and caudad towards T12.
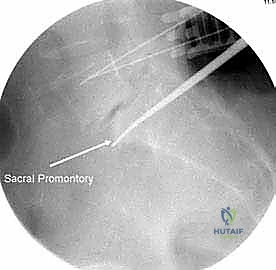
Horizontal and vertical angulations also vary significantly. Medial angulation in the thoracic spine is highest at T1 (up to 30 degrees) and gradually decreases to a neutral or even slightly lateral trajectory at T12. Vertically, thoracic pedicles dictate a slightly superior trajectory, particularly in the upper thoracic spine, to parallel the superior endplate. Conversely, lumbar pedicles (L1-L5) are wider, more robust, and generally easier to cannulate. Width increases progressively from L1 to L5. The horizontal trajectory in the lumbar spine requires increasing medialization, starting from approximately 5-10 degrees at L1 and reaching up to 30 degrees at L5. The S1 pedicle, the widest of all (mean width ~18 mm), requires a distinct trajectory—typically 25 degrees medially and 10 degrees inferiorly, aiming toward the dense bone of the sacral promontory for optimal purchase.
Biomechanically, the integrity of the screw-bone interface is dictated by insertional torque, bone mineral density, and the percentage of the pedicle filled by the screw. Maximizing screw diameter without breaching the cortex increases pullout strength exponentially. Furthermore, achieving an appropriate trajectory that parallels the endplate and converges medially ensures that the screw engages the dense subchondral bone of the anterior vertebral body, maximizing resistance to cantilever bending forces.
Musculoligamentous Corridors and Neurovascular Proximity
Our standard approach is a midline, subperiosteal dissection. This interval separates the erector spinae musculature (multifidus, longissimus, iliocostalis) from the spinous processes, laminae, and facet joints. The multifidus, innervated by the medial branch of the dorsal ramus, is particularly vulnerable to crush injury from prolonged self-retaining retraction; thus, meticulous, efficient exposure is critical to prevent postoperative paraspinal muscle atrophy and chronic axial pain. Alternatively, the Wiltse paraspinal approach exploits the natural cleavage plane between the multifidus and longissimus, preserving midline ligamentous tension bands and minimizing muscle ischemia, a technique often favored in less invasive or adjacent-segment procedures.
The neurovascular risks associated with pedicle preparation are unforgiving. In the thoracic spine, the spinal cord lies immediately medial to the pedicle; a medial breach here can result in catastrophic, irreversible myelopathy. Laterally, the intercostal neurovascular bundles run inferior to the ribs, while anteriorly, the descending aorta (left) and azygos vein (right) pose massive hemorrhagic risks if the anterior vertebral cortex is aggressively violated.
In the lumbar spine, the neural elements are represented by the cauda equina and traversing nerve roots medially, and the exiting nerve roots laterally within the neural foramen. A medial breach risks radiculopathy or dural tears, while a lateral/inferior breach directly endangers the exiting nerve root in Kambin's triangle. Anteriorly, the great vessels—the abdominal aorta and inferior vena cava—lie directly apposed to the anterior longitudinal ligament. An anterior breach with a drill, tap, or over-lengthened screw is a life-threatening vascular emergency.
Exhaustive Indications and Contraindications
The decision to perform a posterolateral instrumented fusion is one of the most consequential in orthopedic practice. It requires a meticulous synthesis of the patient's clinical presentation, radiographic findings, and physiological capacity to tolerate a major reconstructive procedure.
Surgical Decision Making and Patient Selection
The primary indication for this procedure is mechanical instability of the thoracolumbar spine that has proven refractory to exhaustive conservative management (physical therapy, epidural steroid injections, NSAIDs). Degenerative spondylolisthesis, particularly when accompanied by dynamic instability on flexion-extension radiographs, is a classic indication. In these cases, fusion not only stabilizes the slipping segment but also prevents the recurrence of neural compression following a requisite laminectomy. Isthmic spondylolisthesis, driven by a pars interarticularis defect, similarly benefits from robust pedicle screw fixation to halt slip progression and facilitate a stable biological union.
Trauma represents another major category of indications. Unstable burst fractures (e.g., Thoracolumbar Injury Classification and Severity Score [TLICS] > 4), flexion-distraction injuries (Chance fractures), and fracture-dislocations necessitate immediate rigid internal fixation to protect the neural elements, restore sagittal alignment, and allow for early patient mobilization. In the realm of spinal oncology and infection (osteomyelitis/discitis), fusion is indicated when pathological destruction of the anterior or posterior columns renders the spine mechanically incompetent, often performed in conjunction with radical debridement or corpectomy.
Furthermore, iatrogenic instability following aggressive, multi-level decompressive laminectomies or facetectomies (resecting >50% of bilateral facets) mandates concomitant fusion. Adult spinal deformity, including degenerative scoliosis and sagittal imbalance, requires extensive, multi-level instrumented fusions to correct coronal and sagittal parameters, utilizing complex osteotomies and robust pelvic fixation to achieve a balanced, durable spine.
Relative and Absolute Contraindications
While the indications are broad, the contraindications must be respected to avoid catastrophic failure. Absolute contraindications include active, untreated systemic infection (unless the spine itself is the source and requires debridement/stabilization), severe medical comorbidities precluding general anesthesia (e.g., recent myocardial infarction, severe pulmonary hypertension), and a lack of patient consent or capacity to comply with postoperative rehabilitation.
Relative contraindications require nuanced judgment. Severe osteoporosis is a major hurdle; diminished bone mineral density drastically reduces pedicle screw pullout strength, increasing the risk of hardware loosening, subsidence, and adjacent segment fractures. In such cases, surgical strategies must be modified, potentially utilizing cement-augmented fenestrated screws, expanding the construct length to distribute stress, or utilizing under-tapping techniques to maximize cortical thread purchase.
Smoking and nicotine use represent severe relative contraindications due to their profound inhibitory effect on osteogenesis and microvascular perfusion. Nicotine significantly increases the rate of pseudarthrosis (non-union) and postoperative wound complications. Many surgeons mandate documented smoking cessation (often verified via serum cotinine levels) prior to elective fusion. Similarly, chronic steroid use, poorly controlled diabetes mellitus, and severe malnutrition (low serum albumin) severely compromise bone healing and soft tissue recovery, demanding preoperative medical optimization.
| Category | Indications | Contraindications (Relative & Absolute) |
|---|---|---|
| Degenerative | Symptomatic degenerative spondylolisthesis, recurrent disc herniation with instability, severe discogenic pain with Modic changes. | Severe osteoporosis (Relative - requires modified technique), active systemic infection (Absolute). |
| Trauma/Structural | Unstable burst fractures, flexion-distraction injuries, isthmic spondylolisthesis, iatrogenic instability post-laminectomy. | Uncorrectable coagulopathy (Absolute), severe medical frailty precluding anesthesia (Absolute). |
| Deformity/Pathology | Adult degenerative scoliosis, sagittal imbalance, neoplastic destruction, osteomyelitis requiring structural stabilization. | Active smoking/nicotine use (Relative - high risk of pseudarthrosis), severe malnutrition (Relative). |
Pre-Operative Planning, Templating, and Patient Positioning
The success of a thoracolumbar fusion is largely dictated before the patient ever enters the operating room. Meticulous preoperative planning, advanced imaging analysis, and precise patient positioning are the bedrock of a safe and efficient procedure.
Advanced Imaging and Trajectory Templating
Our preoperative assessment begins with high-quality, standing posteroanterior (PA) and lateral radiographs. Standing films are non-negotiable; they reveal the spine under physiological axial load, unmasking deformities and sagittal imbalances that disappear when the patient is supine.

Dynamic flexion-extension views are essential for quantifying occult instability, measuring the exact degree of translation or angular change across a motion segment. For deformity cases, full-length 36-inch cassettes are required to calculate global parameters such as Pelvic Incidence (PI), Pelvic Tilt (PT), Lumbar Lordosis (LL), and the Sagittal Vertical Axis (SVA).
The Computed Tomography (CT) scan is the gold standard for osteological templating.

Axial, coronal, and sagittal reconstructions allow us to meticulously measure the width, length, and trajectory of every individual pedicle. We pre-select our screw diameters based on the narrowest mediolateral dimension of the pedicle isthmus, aiming for an 80% pedicle fill to maximize biomechanical purchase without risking cortical blowout. We also assess bone density via Hounsfield units; low values alert us to the potential need for larger diameter screws, longer trajectories engaging the anterior cortex, or cement augmentation. Magnetic Resonance Imaging (MRI) is concurrently reviewed to assess the degree of central canal, lateral recess, and foraminal stenosis, guiding our decompressive efforts prior to instrumentation.
Prone Positioning and Physiological Optimization
Patient positioning is an active surgical step, not merely a preparatory task. The patient is intubated on the stretcher and carefully log-rolled onto a radiolucent Jackson spinal table.


The Jackson table is preferred over a standard Wilson frame as it avoids excessive hip flexion, thereby preserving physiological lumbar lordosis—a critical factor when locking the spine into a fused position. The chest pads are placed just proximal to the xiphoid, and the iliac pads are positioned precisely over the anterior superior iliac spines (ASIS).
This specific pad placement allows the abdomen to hang completely free. If the abdomen is compressed, intra-abdominal pressure rises, compressing the inferior vena cava. This forces venous return through the epidural venous plexus (Batson's plexus), resulting in torrential, uncontrollable epidural bleeding during the decompression phase. A free-hanging abdomen is arguably your best hemostatic agent.
The arms are placed on padded arm boards, abducted to no more than 90 degrees, and slightly forward-flexed to prevent brachial plexus traction injuries. The elbows must be meticulously padded to protect the ulnar nerve at the cubital tunnel. The neck is maintained in a neutral position to avoid cervical myelopathy, particularly in elderly patients with concurrent cervical stenosis. Before draping, we utilize the C-arm to ensure clear AP and lateral fluoroscopic visualization of all planned operative levels, ensuring the table's crossbars do not obscure our radiographic landmarks.
Step-by-Step Surgical Approach and Fixation Technique
With the patient optimized and prepped, we initiate the surgical exposure. This phase demands efficiency, respect for soft tissue envelopes, and an encyclopedic knowledge of posterior spinal landmarks.
Midline Exposure and Subperiosteal Dissection
We begin with a precise midline incision centered over the spinous processes of the target levels, confirmed via lateral fluoroscopy.

Using monopolar electrocautery, we divide the subcutaneous fat down to the thick, white lumbodorsal fascia. We incise the fascia strictly in the midline, directly over the tips of the spinous processes, to maintain a bloodless plane.

Using a Cobb elevator and electrocautery, we perform a meticulous subperiosteal dissection. The goal is to strip the paraspinal muscles off the bone in one confluent layer, minimizing bleeding from the segmental vessels that pierce the muscle. We expose the spinous processes, the entire lamina, the pars interarticularis, and the facet joints.
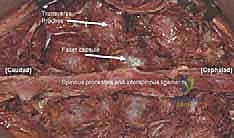
Crucially, the dissection must extend laterally to expose the tips of the transverse processes. The transverse processes and the lateral aspect of the superior articular processes are the anatomical keys to identifying our pedicle starting points and form the primary bed for our posterolateral bone graft. Self-retaining retractors (e.g., Weitlaner or specialized spine retractors) are placed, ensuring they are periodically relaxed to restore perfusion to the multifidus muscle and prevent ischemic necrosis.
Pedicle Cannulation and Instrumentation Mechanics
Pedicle screw insertion is the biomechanical crux of the operation. We rely on a synthesis of anatomical landmarks, tactile feedback, and fluoroscopic confirmation.
In the lumbar spine, the classic starting point is the intersection of a vertical line bisecting the superior articular process and a horizontal line bisecting the transverse process. We use a high-speed burr or a rongeur to decorticate this starting point, creating a small pilot hole that prevents our instruments from skiving.


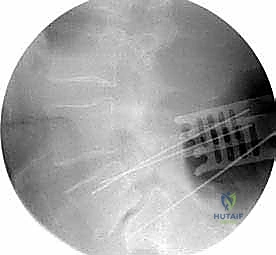
We then introduce the pedicle probe (often a curved gearshift). The trajectory must respect the medial angulation of the pedicle (e.g., 10-15 degrees at L3, up to 30 degrees at L5) and parallel the superior endplate on the sagittal plane.


Advancing the probe requires a delicate touch; you must feel the smooth, continuous resistance of the cancellous bone. A sudden loss of resistance indicates a cortical breach. Once the probe reaches the vertebral body (typically 30-40mm depth), we remove it and utilize a flexible ball-tip feeler to palpate the bottom and all four walls of the tract (medial, lateral, superior, inferior) to definitively rule out a breach.

If the tract is intact, we may tap the pedicle. In osteoporotic bone, we often under-tap by 1mm or skip tapping entirely to maximize the insertional torque and pullout strength of the screw. The pedicle screw is then inserted.
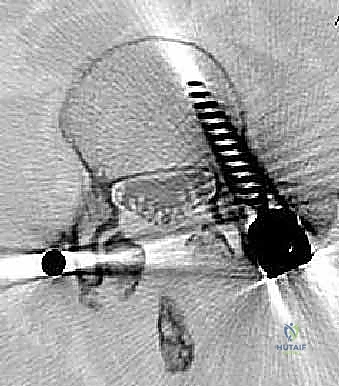
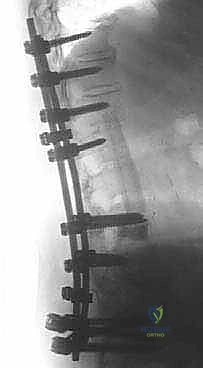
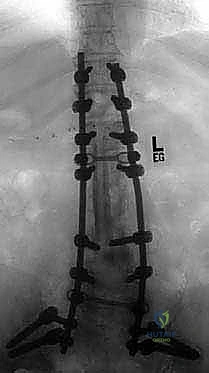
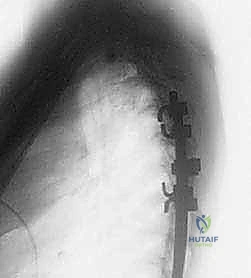
We repeat this process for all planned levels. Intraoperative AP and lateral fluoroscopy are utilized to confirm ideal screw placement: the screw tips should reside in the anterior third of the vertebral body on the lateral view, and the screw heads should not cross the medial border of the pedicle on the AP view.
Decortication and Bone Grafting Strategies
Instrumentation provides immediate mechanical stability, but long-term success relies entirely on biological arthrodesis. If the bone does not fuse, the hardware will eventually fail due to fatigue fracture. Therefore, preparation of the fusion bed is arguably the most critical step for long-term durability.
Once the screws are placed and any necessary neural decompression is complete, we turn our attention to the "posterolateral gutters." This involves aggressive, meticulous decortication of the transverse processes, the lateral aspect of the superior articular processes, and the pars interarticularis. Using a high-speed matchstick burr, we remove the outer cortical layer of bone until bleeding cancellous bone is exposed. This bleeding bone provides the osteoprogenitor cells and vascular supply necessary for the fusion mass to incorporate.


We then pack our bone graft tightly into these decorticated gutters. The gold standard remains iliac crest bone graft (ICBG), which provides osteogenic cells, osteoinductive proteins, and an osteoconductive scaffold. However, due to donor site morbidity, we frequently utilize local autograft (bone harvested during the laminectomy) mixed with allograft extenders (demineralized bone matrix) or synthetic biologics such as Recombinant Human Bone Morphogenetic Protein-2 (rhBMP-2). The graft must bridge the transverse processes continuously. Finally, the contoured titanium or cobalt-chrome rods are seated into the screw heads, and the set screws are provisionally tightened.
Final compression or distraction is applied to optimize lordosis and foraminal height before final torqueing of the construct.

The wound is then heavily irrigated and closed in multiple robust layers to prevent dead space and postoperative hematoma.
Complications, Incidence Rates, and Salvage Management
Even in the most experienced hands, thoracolumbar fusion carries significant risks. A master surgeon is defined not just by their ability to place screws, but by their capacity to anticipate, recognize, and seamlessly manage intraoperative and postoperative complications.
Intraoperative Adversities and Mitigation
Dural tears (incidental durotomies) are the most frequent intraoperative complication, occurring in roughly 5-10% of primary cases and up to 20% in revision surgeries. They typically occur during aggressive bony decompression or scar tissue dissection. If a tear occurs, it must be recognized immediately. Primary repair with 4-0 or 5-0 non-absorbable suture (e.g., Prolene or Nurolon) is the gold standard. If primary repair is impossible due to the tear's location, dural sealants, muscle patches, or fat grafts are utilized, followed by a period of postoperative flat bedrest to prevent cerebrospinal fluid (CSF) fistulas and pseudomeningoceles.
Pedicle screw malposition is another critical risk. A medial breach violates the spinal canal, risking direct trauma to the spinal cord (thoracic) or traversing nerve roots (lumbar). If the ball-tip feeler detects a medial breach during probing, the trajectory must be instantly redirected laterally. If a screw is placed medially and causes neuromonitoring changes (e.g., loss of MEPs or SSEPs) or active CSF leak, it must be removed and redirected. Lateral breaches are less dangerous neurologically but can irritate the exiting nerve root or result in poor biomechanical purchase. Anterior breaches, particularly on the left side of the spine, risk catastrophic injury to the aorta or iliac vessels. If an anterior vascular injury is suspected, the screw should NOT be removed until a vascular surgeon is present and proximal/distal control is established, as the screw may be acting as a tamponade.
Hardware pullout or loss of purchase during insertion occurs primarily in osteoporotic bone. If a pedicle strips during screw insertion, salvage options include upsizing the screw diameter by 1-2mm, increasing the screw length to engage the anterior cortex (bicortical purchase), utilizing a different trajectory (e.g., cortical bone trajectory), or augmenting the pedicle with polymethylmethacrylate (PMMA) bone cement prior to screw re-insertion.
Postoperative Hardware Failure and Pseudarthrosis
Long-term complications center around the failure of the biological fusion process. Pseudarthrosis (non-union) occurs when the bone graft fails to consolidate into a solid mass. It presents months to years later with recurrent axial back pain and eventual hardware failure (screw breakage or rod fracture) due to cyclic micro-motion. Incidence ranges from 5-15%, heavily influenced by patient factors (smoking, diabetes) and surgical technique (inadequate decortication, insufficient graft material). Treatment requires revision surgery, aggressive re-decortication, robust biological augmentation (e.g
