Lumbar Microdiscectomy Masterclass: A Comprehensive Intraoperative Guide
Key Takeaway
Welcome, fellows, to a comprehensive masterclass on lumbar microdiscectomy. We will meticulously navigate every phase of this gold-standard procedure, from precise preoperative planning and patient positioning to the granular intraoperative execution and critical postoperative management. Emphasizing anatomical nuances, instrument handling, and complication avoidance, this guide prepares you for successful surgical intervention for clinically significant lumbar disc herniations.
Welcome, colleagues and fellows, to the operating theater. Today, we delve into the nuances of the lumbar microdiscectomy, a procedure that remains the gold standard for the surgical management of refractory lumbar radiculopathy. When executed with precision, a profound understanding of spinal pathoanatomy, and respect for the surrounding neural elements, this operation offers immediate and life-altering relief to patients suffering from debilitating sciatica. The true art of modern spinal surgery lies not merely in technical execution, but in a comprehensive grasp of the patient's unique anatomical variations, the biomechanical principles at play, and the meticulous preservation of stabilizing structures.
This masterclass is designed to provide an exhaustive, intraoperative guide to lumbar microdiscectomy. We will transcend basic procedural steps, exploring the deep anatomical rationale, advanced preoperative planning, precise microsurgical techniques, and evidence-based complication management required to perform this procedure at the highest academic level.
Comprehensive Introduction and Patho-Epidemiology
Lumbar disc herniation is among the most prevalent spinal pathologies encountered in orthopedic and neurosurgical practice, representing a significant cause of morbidity and economic burden globally. The evolution of its surgical treatment—from the extensive, destabilizing laminectomies of the early 20th century to the minimally invasive, microscope-assisted techniques pioneered by Yasargil and Caspar—reflects a paradigm shift toward tissue preservation. Today, the goal is to achieve maximal neural decompression with minimal iatrogenic disruption of the posterior tension band and paraspinal musculature.
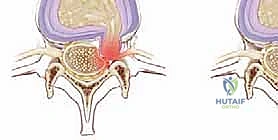
The pathophysiology of lumbar radiculopathy is dual-faceted, involving both mechanical compression and severe biochemical inflammation. A focal distortion of the normal anatomic configuration of discal material leads to direct pressure on the traversing or exiting lumbar nerve root. However, mechanical compression alone is often insufficient to produce the classic, agonizing pain of sciatica. It is the exposure of the highly immunogenic nucleus pulposus to the epidural space—a space normally devoid of these antigens—that triggers a robust, local inflammatory cascade. Cytokines, phospholipase A2, and tumor necrosis factor-alpha (TNF-alpha) sensitize the dorsal root ganglion, drastically lowering the threshold for pain transmission.
Understanding this dual mechanism is critical for the operating surgeon. It explains why a massive, contained protrusion might cause less radicular pain than a small, uncontained sequestration. Furthermore, it underscores the necessity of not only mechanically removing the offending fragment but also thoroughly irrigating the epidural space to clear inflammatory mediators. The natural history of lumbar disc herniation is largely favorable, with macrophage-mediated phagocytosis and dehydration of the extruded fragment leading to spontaneous resolution in a vast majority of patients. However, for those who fail conservative management or present with progressive neurological deficits, surgical intervention provides a definitive, rapid, and highly effective solution.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel ever touches the skin, the surgeon must possess a three-dimensional, deeply internalized map of the lumbar spine. The intervertebral disc is a marvel of biomechanical engineering, designed to allow segmental mobility while providing immense stability and protection to the delicate neural structures housed within the spinal canal.
The Intervertebral Disc Complex
The functional components of the intervertebral disc operate in a delicate biomechanical synergy. The Annulus Fibrosus is the tough, outer boundary composed of 15 to 25 concentric lamellae of highly organized Type I collagen. These fibers are oriented at alternating angles of approximately 30 degrees to the horizontal plane. This highly specific architectural arrangement is critical, as it converts axial compressive loads and multi-planar bending forces into hoop stresses, effectively containing the highly pressurized central core.
The Nucleus Pulposus is the central, gelatinous core, rich in Type II collagen and heavily populated by proteoglycans, specifically aggrecan. These proteoglycans possess a high fixed negative charge density, which osmotically imbibes water, creating a hydrostatic shock absorber. This pressurized core balances mechanical loads across the vertebral segment, pushing outward against the annulus and upward against the endplates. The Vertebral Endplates are thin layers of hyaline and fibrocartilage capping the superior and inferior vertebral bodies. Because the adult disc is the largest avascular structure in the human body, these endplates are the sole avenue for the diffusion of essential nutrients (glucose, oxygen) into the nucleus and the expulsion of metabolic waste (lactic acid).
With progressive disc degeneration—a natural aging process frequently accelerated by genetic predisposition and repetitive microtrauma—the endplates become sclerotic, severely impeding diffusion. The nucleus, starved of nutrition, fails to synthesize new proteoglycans and loses its hydrostatic properties. Concurrently, the annular lamellae undergo structural failure, losing collagen crosslinking and developing radial clefts. This biomechanical collapse shifts the axial load directly onto the posterior annulus, creating the perfect storm for the herniation of nuclear material through the weakened fibrous ring.
Neural Anatomy and Topographical Zones
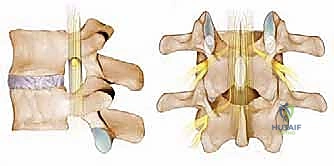
The lumbar nerve roots travel within the common dural sac, forming the cauda equina, before systematically exiting at each respective level. It is a fundamental anatomical rule that lumbar nerve roots are numbered according to the pedicle beneath which they pass. Therefore, the L5 nerve root exits beneath the L5 pedicle, traversing the L4-L5 disc space before doing so. Understanding the relationship between the traversing root and the exiting root at any given disc level is the cornerstone of safe microdiscectomy.
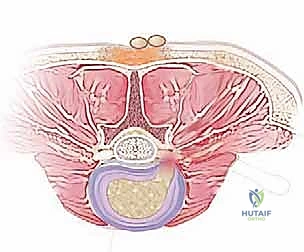
The spinal canal and its lateral recesses are surgically divided into distinct topographical zones from medial to lateral. The Central Canal is the most medial portion, containing the dural sac and the descending cauda equina. Herniations here typically affect the traversing roots or, if massive, can precipitate cauda equina syndrome. The Subarticular Zone (Lateral Recess) lies lateral to the central canal, bordered anteriorly by the posterior aspect of the vertebral body and disc, and posteriorly by the superior articular process (medial facet). This is the most common site for nerve root compression by a paracentral disc herniation, directly impinging the traversing nerve root.
Moving further laterally, we encounter the Foraminal Zone, the neural foramen itself, bounded by the pedicles superiorly and inferiorly. Here, the exiting nerve root passes. Herniations in this zone are far less common but are notorious for causing severe radiculopathy of the exiting root (e.g., an L4-L5 foraminal herniation compressing the L4 root). Finally, the Extraforaminal (Far-Lateral) Zone lies entirely lateral to the pedicle borders. Herniations here also compress the exiting nerve root and require a completely different surgical approach, typically a Wiltse paraspinal muscle-splitting approach, rather than a traditional interlaminar window.
Pathoanatomic Classification of Herniations
Accurate morphological classification of the disc herniation is paramount for preoperative planning, predicting intraoperative findings, and minimizing surgical morbidity. We classify herniations based on two primary parameters: annular integrity and anatomic migration.
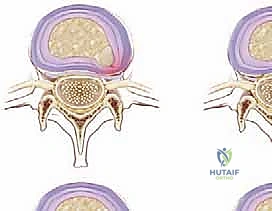
Based on annular integrity, a Protrusion (or bulge) indicates that the annulus remains intact, but there is a localized, broad-based or focal distortion of disc material. A Subannular Extrusion occurs when the nucleus has forced its way through the inner annular fibers but remains contained by the outermost annular lamellae or the posterior longitudinal ligament (PLL). A Transannular Extrusion signifies that the nuclear material has completely breached all layers of the annulus and the PLL, exposing the epidural space to raw nucleus pulposus. Finally, a Sequestration is a free fragment of nuclear material that has completely detached from the parent disc and migrated away from the annular defect.

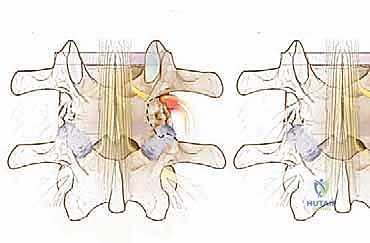
We further classify herniations based on their anatomic location relative to the disc space, utilizing the "story" concept to describe migration. The First Story represents pathology at the disc level itself. The Second Story indicates migration cephalad, typically lodging under the lamina of the superior vertebra or into the axilla of the exiting nerve root. The Third Story represents migration caudally, often sliding down the posterior aspect of the inferior vertebral body, adjacent to the pedicle below. Recognizing these migration patterns on preoperative imaging dictates the extent of bony resection required; a severe third-story migration will require a much more aggressive inferior laminotomy or even a partial pedicle resection to safely retrieve the fragment.

Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention must be grounded in a rigorous clinical evaluation, correlating the patient's subjective symptoms and objective neurological deficits with definitive advanced imaging. Surgery is never indicated for axial back pain alone in the setting of a focal disc herniation; the primary goal of a microdiscectomy is the relief of radiculopathy.
Absolute and Relative Indications
The absolute indications for lumbar microdiscectomy are rare but demand immediate, emergent surgical decompression. Cauda Equina Syndrome is the most critical of these, characterized by a massive central disc herniation compressing the entire thecal sac. Clinically, this manifests as bilateral lower extremity radiculopathy, progressive motor weakness, saddle anesthesia, and crucial autonomic dysfunction, typically urinary retention with overflow incontinence or loss of bowel control. The second absolute indication is a profound, rapidly progressive motor deficit (e.g., a sudden, profound foot drop). In these scenarios, time is tissue, and emergent decompression within 24 to 48 hours is mandated to maximize the potential for neurological recovery.
Relative indications encompass the vast majority of elective microdiscectomies. The most common is the failure of exhaustive conservative measures. A patient who has endured 6 to 12 weeks of excruciating radicular pain despite a rigorous regimen of NSAIDs, short-course oral corticosteroids, physical therapy (specifically McKenzie-based extension protocols), activity modification, and potentially fluoroscopically guided transforaminal epidural steroid injections is a prime surgical candidate. Furthermore, multiply recurrent sciatica that severely impacts the patient's quality of life, or a static but functionally limiting motor deficit (such as a persistent weakness in extensor hallucis longus testing), strongly justifies surgical intervention.
Differential Diagnosis and Contraindications
A master surgeon must always maintain a broad differential diagnosis to avoid operating on the wrong pathology. Intraspinal, extrinsic compression can mimic a disc herniation; conditions such as lateral recess stenosis from facet hypertrophy, synovial cysts, epidural abscesses, or spinal neoplasms must be ruled out. Intraspinal, intrinsic nerve root dysfunction, such as diabetic amyotrophy, herpes zoster radiculitis, or arachnoiditis, will not improve with decompression. Extraspinal sources of sciatic-like pain, including sacroiliac joint dysfunction, severe hip osteoarthritis, piriformis syndrome, or peripheral neuropathies (e.g., peroneal nerve entrapment at the fibular head), must be clinically excluded through a meticulous physical examination.
| Category | Specific Conditions | Clinical Implications |
|---|---|---|
| Absolute Indications | Cauda Equina Syndrome, Rapidly Progressive Motor Deficit | Emergent surgical decompression required (ideally < 48 hours). |
| Relative Indications | Failed Conservative Therapy (>6-12 weeks), Intractable Pain, Recurrent Sciatica | Elective surgery; high success rate for radicular pain relief. |
| Absolute Contraindications | Active systemic infection, Uncorrected coagulopathy, Absence of radicular symptoms | High risk of catastrophic complications; surgery will not benefit axial back pain. |
| Relative Contraindications | Severe psychological overlay, Uncontrolled diabetes, Morbid obesity | Increased risk of surgical site infection, poor wound healing, and suboptimal functional outcomes. |
Pre-Operative Planning, Templating, and Patient Positioning
"Failing to plan is planning to fail." This surgical adage is the bedrock of safe spinal surgery. Preoperative planning aims to definitively answer three critical questions: What specific nerve root is involved? Where precisely is the herniated material located relative to the neural elements? What surgical trajectory will afford the safest and most direct access to the pathology while minimizing collateral tissue damage?
Advanced Neuroimaging Modalities
Magnetic Resonance Imaging (MRI) without contrast is the absolute gold standard for evaluating lumbar disc herniation. The surgeon must personally review the T1, T2, and STIR (Short Tau Inversion Recovery) sequences in axial, sagittal, and coronal planes. T2-weighted sagittal images provide an excellent overview of disc hydration, annular tears (High-Intensity Zones), and thecal sac compression. Axial T2 images are critical for defining the exact zone of the herniation (central, subarticular, foraminal) and its relationship to the traversing and exiting nerve roots. Contrast-enhanced MRI (Gadolinium) is reserved for revision cases to differentiate between enhancing epidural fibrosis (scar tissue) and non-enhancing recurrent disc herniation.
When MRI is strictly contraindicated (e.g., patients with incompatible pacemakers or severe claustrophobia), a CT-Myelogram is the alternative of choice. While more invasive, it provides exquisite bony detail and clearly delineates nerve root cutoff or thecal sac compression. Plain radiographs, including standing anteroposterior, lateral, and dynamic flexion-extension views, are mandatory. They are not used to diagnose the disc herniation itself, but to rule out occult instability (spondylolisthesis), identify transitional lumbosacral anatomy (lumbarized S1 or sacralized L5), and assess overall sagittal balance—factors that could drastically alter the surgical plan from a simple decompression to a fusion.
Patient Positioning and Operating Room Setup
Patient positioning is a highly active phase of the operation. Proper positioning optimizes the surgical corridor, dramatically reduces intraoperative hemorrhage, and prevents catastrophic iatrogenic positioning injuries. We utilize a kneeling position, typically employing an Andrews frame, a Wilson frame, or a specialized Jackson table with a spinal sling.
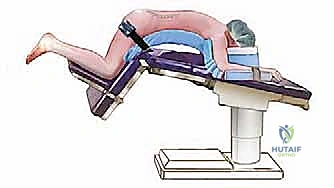
The primary goal of positioning is twofold. First, we must achieve a degree of lumbar flexion. By flexing the hips and knees, we reverse the natural lumbar lordosis, which opens the posterior interlaminar window, maximizing the space between adjacent spinous processes and laminae. This simple maneuver significantly reduces the amount of bony resection required to access the epidural space. Second, and equally critical, the patient's abdomen must be completely free and pendulous. Any external pressure on the abdomen increases intra-abdominal pressure, which is directly transmitted to the inferior vena cava. This forces venous return to bypass the IVC and engorge the valveless epidural venous plexus of Batson. An engorged Batson's plexus leads to torrential, obscuring epidural bleeding during the microdiscectomy, making the procedure exponentially more difficult and dangerous.
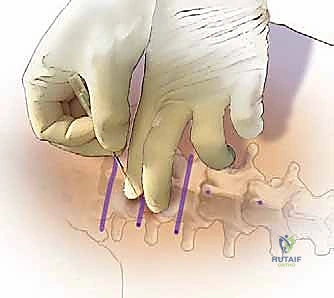
Upper extremity positioning requires meticulous attention. Shoulders must be abducted to less than 90 degrees with slight forward flexion to prevent brachial plexus stretch injuries. All bony prominences—the ulnar nerve at the cubital tunnel, the peroneal nerve at the fibular head, the patellae, and the face—must be heavily padded. Once positioned, fluoroscopy is brought in for definitive pre-incision localization. A spinal needle is placed over the presumed interspace, and a lateral radiograph confirms the exact level, allowing for a perfectly targeted, minimally invasive incision.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of a lumbar microdiscectomy requires a seamless blend of gross orthopedic exposure and delicate neurosurgical tissue handling. The transition from the macro-environment of the paraspinal musculature to the micro-environment of the epidural space demands a shift in both instrumentation and surgical mentality.
Incision and Myofascial Dissection
Following precise fluoroscopic localization, a strict midline incision is made, typically 2 to 3 centimeters in length, centered directly over the targeted interspace. The subcutaneous tissues are divided using electrocautery down to the lumbodorsal fascia. Hemostasis must be absolute at every layer to prevent blood from pooling in the microscopic field later in the case. The fascia is incised sharply just off the midline, preserving the supraspinous ligament.
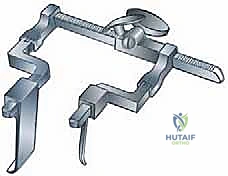
Using a Cobb elevator and precise monopolar cautery, a subperiosteal dissection of the multifidus and longissimus muscles is performed off the spinous processes and laminae of the superior and inferior vertebrae. This dissection must be strictly subperiosteal to minimize muscle bleeding and denervation. The exposure is carried laterally only as far as the medial aspect of the facet joint. Violating the facet capsule can lead to postoperative instability and persistent axial back pain. Once the interlaminar space is adequately exposed, a self-retaining retractor (such as a Taylor, Williams, or specialized tubular retractor) is deployed to maintain the corridor.

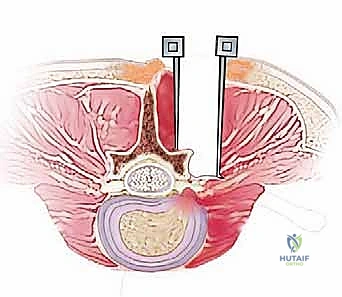
Bony Decompression and Flavectomy
At this juncture, the operating microscope or high-powered loupes with a coaxial headlight are introduced. The interlaminar window is often obscured by the overhanging inferior edge of the superior lamina and hypertrophic ligamentum flavum. Using a high-speed matchstick burr or a Leksell rongeur, a targeted inferior laminotomy is performed. The goal is to thin the lamina down to the underlying ligamentum flavum, creating a safe starting point for the Kerrison rongeurs.
The ligamentum flavum is the final barrier protecting the dura. It is carefully detached from its bony insertions using a curette. A small defect is created in the flavum using a sharp hook or a scalpel, exposing the epidural fat beneath. Once the epidural space is breached, a 2mm or 3mm Kerrison rongeur is used to systematically resect the ligamentum flavum, working from medial to lateral. The lateral recess must be adequately decompressed by undercutting the medial facet until the lateral border of the traversing nerve root is clearly visualized and free of bony impingement.
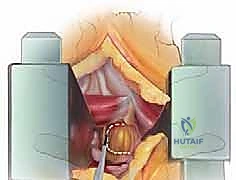
Neural Mobilization and Microdiscectomy
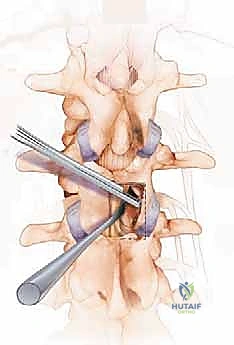
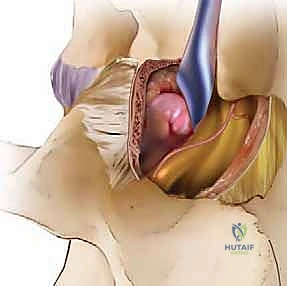
With the epidural space exposed, the surgeon will encounter the epidural venous plexus and the traversing nerve root. If the abdomen is well-positioned, venous bleeding will be minimal and easily controlled with bipolar electrocautery and micro-patties. The nerve root, often swollen, erythematous, and displaced posteriorly by the underlying disc herniation, must be handled with extreme reverence. Using a Penfield #4 or a specialized nerve root retractor, the root is gently mobilized and retracted medially.
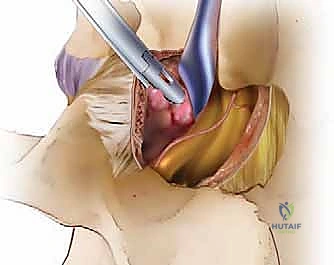
Retracting the root exposes the bulging annulus or the extruded nuclear fragment. If the fragment is sequestered, it can often be plucked directly from the epidural space using pituitary rongeurs. If the herniation is contained, a formal annulotomy is required. Using a #11 blade on a bayoneted handle, a crucial, box-like or cruciate incision is made in the annulus, strictly within the "safe zone" lateral to the dura and inferior to the exiting root.
Straight and up-angled pituitary rongeurs are then introduced into the disc space to remove loose, degenerated nuclear material. The goal is not a radical, complete discectomy—which accelerates disc collapse and degeneration—but rather a targeted subtotal discectomy, removing only the loose fragments that pose a risk for immediate reherniation. The nerve root is then allowed to return to its anatomic position. A blunt hook is passed into the foramen and lateral recess to ensure absolute freedom of the neural elements.
Following copious irrigation with antibiotic-impregnated saline to wash out inflammatory cytokines, absolute hemostasis is achieved. The fascia is closed tightly with interrupted heavy absorbable sutures to prevent muscular herniation and dead space formation. The subcutaneous tissue and skin are closed meticulously to ensure optimal cosmesis.

Complications, Incidence Rates, and Salvage Management
While lumbar microdiscectomy is highly successful, it is not without risk. A master surgeon is defined not only by their technical prowess but by their ability to anticipate, recognize, and definitively manage intraoperative and postoperative complications.
Intraoperative Complications
The most common intraoperative complication is an incidental durotomy (dural tear), occurring in approximately 3% to 5% of primary cases, and significantly higher in revision surgery due to epidural fibrosis. If a tear occurs, it must be recognized immediately. The primary treatment is meticulous, watertight primary repair using 4-0 or 5-0 non-absorbable monofilament suture (e.g., Prolene or Nurolon) under microscopic magnification. The repair is then reinforced with a dural sealant (fibrin glue) and occasionally an autologous muscle or fat patch. A Valsalva maneuver is performed by anesthesia to confirm the integrity of the repair.
Nerve root injury is a catastrophic complication, usually resulting from excessive traction, unrecognized aberrant anatomy (such as con
