General Cervical Treatment: Essential Spine Care & Options
Key Takeaway
Looking for accurate information on General Cervical Treatment: Essential Spine Care & Options? Initial treatment general cervical involves immobilization with a cervical orthosis for stable fractures or skull traction for unstable injuries. Vasopressor support may be indicated for neurogenic shock. Most fractures are managed nonoperatively using cervical orthoses, ranging from soft collars for minor issues to rigid devices like the Halo, which offers the most rigid immobilization. Traction with Gardner-Wells tongs aids reduction of facet dislocations.
Introduction and Epidemiology
Cervical spine injuries encompass a spectrum of pathologies ranging from soft tissue sprains and strains to complex fractures, dislocations, and devastating spinal cord injuries (SCI). These injuries represent a significant challenge in orthopedic trauma, given the critical neurovascular structures housed within the cervical column and the profound implications of neurological compromise. Effective management necessitates a thorough understanding of cervical anatomy, biomechanics, and evidence-based treatment strategies.
The epidemiology of cervical spine injuries varies geographically but generally demonstrates a bimodal distribution. High-energy mechanisms, such as motor vehicle accidents (MVAs) and falls from height, account for the majority of injuries in younger, active populations. Conversely, low-energy falls represent a leading cause in the elderly, often superimposed on pre-existing degenerative conditions or osteopenia. Sports-related injuries, particularly those involving axial loading (e.g., diving accidents, football tackles), also contribute significantly. Complete SCI is estimated to occur in approximately 2-3% of all cervical spine fractures and dislocations, underscoring the urgency of accurate diagnosis and appropriate initial management. The socioeconomic burden associated with these injuries, including long-term care for SCI patients, is substantial. Advances in prehospital care, imaging modalities, and surgical techniques have significantly improved outcomes, emphasizing the need for a standardized, comprehensive approach to diagnosis and treatment.
Surgical Anatomy and Biomechanics
A profound understanding of cervical spine anatomy and biomechanics is foundational for effective clinical assessment and surgical intervention. The cervical spine, comprising seven vertebrae (C1-C7), is uniquely adapted for mobility while simultaneously protecting the spinal cord and exiting nerve roots.
Bony Anatomy
The atlas (C1) and axis (C2) are atypical vertebrae adapted for craniocervical rotation. C1 is a ring-like structure lacking a vertebral body, articulating with the occipital condyles superiorly and C2 inferiorly. C2 features the odontoid process (dens), which articulates with the anterior arch of C1, acting as a pivot. C3-C7 are typical cervical vertebrae, characterized by a small, rectangular vertebral body, short pedicles, bifid spinous processes (C3-C6), and transverse foramina for the vertebral arteries (C1-C6). The superior and inferior articular facets form apophyseal (facet) joints, which are oriented obliquely, facilitating flexion, extension, lateral bending, and rotation. The uncinate processes (of Luschka), unique to C3-C7, articulate with the superjacent vertebral body, forming uncovertebral joints that guide motion and help prevent disc herniation.
Ligamentous Anatomy
The inherent stability of the cervical spine is largely conferred by a complex array of ligaments. The anterior longitudinal ligament (ALL) and posterior longitudinal ligament (PLL) provide significant stability anteriorly and posteriorly, respectively. The ligamentum flavum, situated between adjacent laminae, and the interspinous and supraspinous ligaments contribute to posterior column stability. At the craniocervical junction, crucial ligaments include the transverse ligament of the atlas, which restrains the odontoid process against the anterior arch of C1; the alar ligaments, connecting the dens to the occipital condyles, limiting axial rotation and lateral bending; and the tectorial membrane, a superior extension of the PLL. Disruption of these ligaments, particularly the transverse ligament, can lead to profound instability.
Neurological Anatomy
The cervical spinal cord extends from the foramen magnum to approximately the C7-T1 level. Eight cervical nerve roots (C1-C8) exit above their corresponding pedicles (C1 exits above C1, C8 exits below C7). Knowledge of dermatomal and myotomal distribution is critical for localizing neurological deficits. The vertebral arteries ascend through the transverse foramina of C6 to C1, passing medially to enter the foramen magnum. Compression or dissection of these arteries, especially at the C1-C2 segment, can lead to vertebrobasilar insufficiency. The recurrent laryngeal nerve, part of the vagus nerve, is particularly vulnerable during anterior cervical approaches due to its proximity to the tracheoesophageal groove.
Biomechanics of Cervical Stability
The cervical spine functions as a flexible column, balancing mobility with stability. Panjabi's three-column model, adapted for the cervical spine, describes the anterior column (anterior part of vertebral body, ALL, anterior annulus), middle column (posterior part of vertebral body, PLL, posterior annulus), and posterior column (facet joints, pedicles, laminae, spinous processes, and posterior ligamentous complex). Injury to two or more columns generally indicates instability. Specific movements like flexion, extension, lateral bending, and axial rotation involve complex coupled motions, influenced by the orientation of the facet joints and the integrity of the disc-ligamentous complex. Understanding these biomechanical principles is essential for classifying injury patterns and determining appropriate stabilization strategies.
Indications and Contraindications
Effective management of cervical spine injuries begins with immediate, appropriate care in the emergency setting, followed by a thorough evaluation to determine the most suitable treatment pathway – non-operative or operative.
Initial Emergency Management
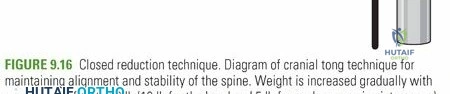
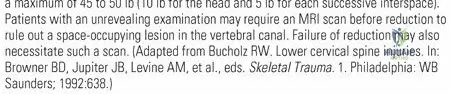
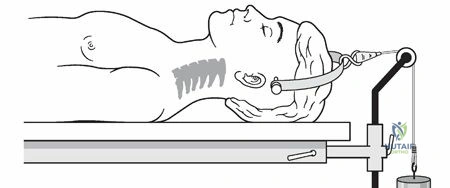
Upon presentation, all patients with suspected cervical spine trauma should be managed with strict spinal precautions. This involves immediate immobilization with a rigid cervical orthosis (e.g., Philadelphia, Miami J, Aspen) and a backboard to prevent secondary neurological injury. Skull traction using Gardner-Wells tongs or a halo-crown may be applied for unstable injuries, particularly those involving dislocations, to achieve reduction and maintain alignment prior to definitive imaging or surgical intervention. A halo-crown, when applied, can later be incorporated into a halo-vest for prolonged immobilization.
Vasopressor support is indicated for suspected neurogenic shock, characterized by hypotension and bradycardia resulting from disruption of sympathetic outflow (typically T6 or higher). Concomitant emergency assessment for potential intracranial trauma and other systemic injuries is paramount as polytrauma is common. The use of high-dose intravenous methylprednisolone per the NASCIS II and III protocols (30 mg/kg loading dose followed by 5.4 mg/kg/hour) has been highly controversial for years and is no longer considered the standard of care. Current evidence suggests no clear long-term benefit and a potential increase in complications, including infection and gastrointestinal bleeding. Therefore, its routine administration is not recommended.
Non-Operative Management
The majority of stable cervical spine fractures and many soft tissue injuries can be treated non-operatively with external immobilization. The goal is to reduce motion, promote healing, and protect the spinal cord.
Soft Cervical Orthosis
A soft cervical collar provides minimal immobilization and is primarily used for comfort and proprioceptive feedback. It is indicated for minor neck strains, whiplash injuries, or as a transitional brace after more rigid immobilization. It offers no significant mechanical support against fracture displacement.
Rigid Cervical Orthosis
Rigid cervical orthoses, such as the Philadelphia collar, Miami J collar, or Aspen collar, are more effective in controlling flexion and extension. However, they provide limited control of rotational and lateral bending movements. These are indicated for stable fractures (e.g., stable odontoid type II fractures in selected patients, stable C3-C7 compression fractures), post-operative stabilization, or stable ligamentous injuries. They decrease gross motion but do not achieve true immobilization, particularly at the occipitocervical junction, where motion may paradoxically increase with some collars.
Caption: Example of various cervical orthoses, illustrating different levels of immobilization and support.
Cervicothoracic Orthoses
Poster braces (e.g., Sterno-Occipital-Mandibular Immobilizer (SOMI), Minerva brace) and halo-vest systems provide superior immobilization compared to rigid collars, particularly for more unstable injuries or higher cervical spine involvement.
* SOMI brace: Effective in controlling mid-cervical flexion and extension but less so for C1-C2 rotation.
* Minerva brace: Offers excellent control of all cervical spine motions, often used for stable upper cervical fractures or severe mid-cervical injuries.
* Halo-vest: Considered the gold standard for non-operative immobilization of unstable cervical spine injuries, particularly those involving the craniocervical junction or C1-C2. It provides nearly complete immobilization in all planes. Indications include irreducible C1/C2 fractures, some stable odontoid fractures, and selected lower cervical spine injuries where surgical risk is prohibitive.
Operative Management Indications
Surgical intervention is indicated in cases of spinal instability, neurological compromise, or failure of non-operative treatment. The primary goals of surgery are decompression of neural elements, reduction of deformity, and stabilization of the spinal column.
- Neurological Deficit: Progressive or profound neurological deficit, particularly in the setting of ongoing spinal cord compression.
- Spinal Cord Compression: Radiographic evidence of spinal cord or nerve root compression by fracture fragments, hematoma, disc material, or bone.
- Spinal Instability: Mechanical instability (gross instability on dynamic imaging, significant ligamentous disruption, severe bony disruption) or neurological instability (risk of neurological deterioration).
- Irreducible Dislocations: Complete facet dislocations that cannot be reduced by closed traction.
- Failure of Non-Operative Treatment: Progressive deformity, nonunion, or persistent instability despite adequate external immobilization.
- Specific Fracture Patterns:
- Burst fractures with significant canal compromise.
- Unstable odontoid fractures (Type II in young, healthy patients; Type III).
- Teardrop fractures (flexion or extension type) with instability.
- Bilateral facet dislocations.
- Unstable C1 fractures (e.g., Jefferson fracture with significant transverse ligament disruption or atlanto-occipital dissociation).
- Ligamentous injuries leading to significant translational or angular deformity (e.g., distractive flexion injuries).
Contraindications for Operative Management
While rare, certain patient factors may contraindicate immediate or elective cervical spine surgery.
* Severe Comorbidities: Uncontrolled medical conditions (e.g., severe cardiac, pulmonary, or renal disease) that significantly increase anesthetic or surgical risk.
* High Anesthetic Risk: Patients unable to tolerate general anesthesia.
* Irreparable Spinal Instability: In rare, devastating injuries where fixation is not biomechanically feasible or offers no functional benefit.
* Complete Spinal Cord Injury (SCI) with Stable Spine: For patients with complete SCI where the spine is stable and there is no ongoing compression, further surgical decompression may offer no benefit and carries inherent risks.
* Patient Refusal: An informed patient's refusal of surgical intervention, assuming mental capacity.
| Indication Category | Non-Operative Management | Operative Management |
|---|---|---|
| Fracture Stability | Stable fractures (e.g., stable C3-C7 compression, Type I odontoid, selected Type II odontoid) | Unstable fractures (e.g., burst fractures with canal compromise, bilateral facet dislocations, Type II/III odontoid in unstable patients) |
| Ligamentous Integrity | Intact or minor ligamentous injury | Significant ligamentous disruption (e.g., transverse ligament, posterior ligamentous complex disruption leading to instability) |
| Neurological Status | Intact neurology or stable, non-progressive deficit | Progressive neurological deficit, acute spinal cord compression, irreducible neurological deficits |
| Alignment | Maintained or easily reducible and stable alignment | Irreducible deformity, significant kyphosis, persistent subluxation/dislocation |
| Patient Factors | High surgical risk comorbidities, patient preference (stable cases) | Otherwise healthy, good surgical candidate, failure of non-op treatment |
Pre Operative Planning and Patient Positioning
Meticulous preoperative planning is critical to optimizing outcomes and minimizing complications in cervical spine surgery. This phase encompasses thorough diagnostic workup, patient optimization, and precise intraoperative setup.
Diagnostic Workup
A comprehensive imaging evaluation is essential.
* Plain Radiographs: AP, lateral, and odontoid views are initial screening tools. Flexion-extension views may be obtained in stable patients to assess for occult instability, though they are often deferred in acute trauma.
* Computed Tomography (CT): The gold standard for bony detail, demonstrating fracture patterns, degree of canal compromise, and facet joint integrity. Multiplanar reconstructions and 3D reformations are invaluable.
* Magnetic Resonance Imaging (MRI): Essential for evaluating soft tissue injuries (ligamentous disruption, disc herniation), spinal cord edema or contusion, hematoma, and nerve root compression. It is crucial in assessing neurological status and guiding the need for decompression.
* CT Angiography (CTA) or Magnetic Resonance Angiography (MRA): Indicated if vertebral artery injury is suspected (e.g., fractures involving transverse foramina, C1-C2 dislocations, significant subluxation).
Surgical Goals
The primary surgical goals include:
1. Decompression: Relief of neural element compression (spinal cord or nerve roots) by removing bone fragments, disc material, or hematoma.
2. Reduction: Restoration of physiological spinal alignment.
3. Stabilization: Creation of a rigid construct to promote arthrodesis and prevent further deformity or neurological injury.
4. Fusion: Promotion of bony union across the unstable segment.
Patient Optimization
Patients must be medically optimized prior to surgery. This involves addressing comorbidities, ensuring adequate nutritional status, and implementing deep vein thrombosis (DVT) prophylaxis. Preoperative neurological assessment, including detailed motor, sensory, and reflex examination, is vital for baseline comparison.
Anesthesia Considerations
Airway management can be challenging in patients with cervical spine injuries. Awake fiberoptic intubation or video laryngoscopy (e.g., Glidescope) may be preferred in unstable patients to minimize neck manipulation. Neuromonitoring (somatosensory evoked potentials (SSEPs) and motor evoked potentials (MEPs)) is strongly recommended to detect any intraoperative neurological compromise, particularly during reduction maneuvers or hardware placement. Anesthetic agents, blood pressure management, and fluid balance must be carefully controlled to optimize spinal cord perfusion.
Patient Positioning
Precise and stable patient positioning is paramount for surgical access and prevention of iatrogenic injury.
Anterior Approach
For anterior cervical discectomy and fusion (ACDF) or corpectomy, the patient is typically positioned supine.
* Head Support: The head is secured in a Mayfield head holder or Gardner-Wells tongs, allowing for gentle manipulation and traction. Slight neck extension facilitates exposure.
* Shoulder Roll: A rolled blanket or pillow is placed transversely under the shoulders to aid neck extension and shoulder retraction.
* Shoulder Retraction: Shoulders are taped caudally to improve radiographic visualization of the cervicothoracic junction.
* Traction: If indicated, skeletal traction is maintained via the tongs or halo to assist with reduction and distraction. Continuous monitoring of traction weight is essential.
Caption: Intraoperative image demonstrating patient positioning for an anterior cervical approach, with the head stabilized in a head holder and shoulders taped for optimal exposure.
Posterior Approach
For posterior cervical fusion or laminectomy, the patient is positioned prone.
* Chest Roll/Frame: Chest rolls or a spinal frame (e.g., Jackson table, OSI Mizuho) are used to support the torso, allowing the abdomen to hang free. This reduces intra-abdominal pressure, minimizing epidural venous bleeding.
* Head Support: The head is secured in a Mayfield head holder or Gardner-Wells tongs, allowing for controlled neck flexion to optimize surgical exposure while maintaining sagittal alignment. Careful attention is paid to facial and ocular pressure points.
* Upper Extremities: Arms are tucked at the sides or positioned on arm boards, ensuring adequate padding to prevent peripheral nerve compression.
* Pressure Points: All bony prominences (e.g., knees, ankles, elbows) are meticulously padded to prevent pressure ulcers or nerve palsies.
Caption: Intraoperative fluoroscopic image showing appropriate screw placement during a posterior cervical fusion, confirming alignment and hardware trajectory.
Detailed Surgical Approach and Technique
Surgical techniques for cervical spine management aim to decompress neural elements, restore spinal alignment, and achieve stable fusion. The choice of approach (anterior, posterior, or combined) depends on the specific pathology, location of compression, and desired biomechanical construct.
Anterior Cervical Approach (Smith-Robinson)
The anterior approach is commonly used for disc herniations, osteophytes, fractures, and deformities requiring ventral decompression and fusion.
Incision and Dissection
A transverse skin incision is typically made in a Langer's line, usually at the level of the cricoid cartilage for mid-cervical pathology. The platysma muscle is divided transversely. The sternocleidomastoid (SCM) muscle is identified and retracted laterally. The strap muscles (sternohyoid, sternothyroid) are then retracted medially. This dissection proceeds through an avascular plane between the carotid sheath laterally and the tracheoesophageal complex medially. The recurrent laryngeal nerve (RLN) typically runs in the tracheoesophageal groove, with the right RLN more variable in its course. Careful blunt dissection to identify and protect these structures is paramount. The prevertebral fascia is incised longitudinally, exposing the longus colli muscles and the anterior vertebral bodies.
Exposure
The longus colli muscles are meticulously dissected from the anterior vertebral bodies and disc spaces to expose the desired levels. This subperiosteal dissection is carried out using electrocautery and periosteal elevators. Self-retaining retractors (e.g., Caspar, Cloward) are carefully placed, ensuring adequate exposure without excessive pressure on vital structures. Fluoroscopic guidance is used to confirm the correct spinal level.
Decompression
- Anterior Cervical Discectomy and Fusion (ACDF): For disc herniations or osteophytes, a complete discectomy is performed. The anterior annulus is incised, and disc material is removed using rongeurs and curettes. Meticulous care is taken to remove disc material posteriorly and decompress the spinal cord and nerve roots. The cartilaginous endplates are removed, leaving the cortical bone of the endplates intact to promote fusion.
- Corpectomy and Fusion (ACCF): For significant vertebral body pathology (e.g., burst fractures, tumor, multi-level osteophytes), a corpectomy is performed. The anterior longitudinal ligament is incised, and the vertebral body is progressively resected using a high-speed burr, rongeurs, and curettes. Decompression extends sufficiently to relieve all neural compression, including posterior osteophytes or migratory fragments. Posterior epidural venous plexuses should be managed carefully to avoid excessive bleeding.
Reconstruction and Fixation
After decompression, the intervertebral space (for ACDF) or corpectomy defect (for ACCF) is reconstructed.
* Graft Selection: Autograft (iliac crest), allograft (fibula, tricortical), or PEEK cages are commonly used for structural support. Cages may be filled with bone graft material (autograft, allograft, synthetic).
* Plate Application: A titanium plate is then applied to the anterior aspect of the vertebral bodies, spanning the fused segments. Screws are placed into the vertebral bodies above and below the fusion mass. Fixed-angle screws provide rigid stability, while variable-angle screws allow for minor adjustments in trajectory. Screw length and trajectory must be carefully selected to avoid spinal cord, vertebral artery, or posterior annulus perforation. Unicortical screw placement is generally sufficient to achieve biomechanical stability in the cervical spine.
Posterior Cervical Approach
The posterior approach is primarily used for decompression (laminectomy, laminoplasty), stabilization of posterior element injuries, reduction of dislocations, and fusion for instability or deformity.
Incision and Dissection
A midline incision is made from the external occipital protuberance to the desired caudal level. The superficial fascia and nuchal ligament are incised. Subperiosteal dissection of the paraspinal muscles (trapezius, splenius capitis, semispinalis capitis, multifidus) from the spinous processes and laminae is performed. At C1 and C2, preserving the muscle attachments to the spinous process and arch of C1 is often desirable to minimize muscle denervation and bleeding, though subperiosteal dissection of the C2 spinous process and lamina is standard for exposure.
Decompression (Laminectomy, Laminoplasty)
- Laminectomy: Resection of the laminae and spinous processes is performed to decompress the spinal cord, typically for multi-level stenosis or posterior compression from a tumor. Care is taken to protect the dura and nerve roots.
- Laminoplasty: This technique involves creating a hinge on one side of the lamina and cutting the opposite side, allowing the lamina to be expanded (open-door laminoplasty) or split centrally and spread (French-door laminoplasty). The expanded laminae are then secured with small plates or sutures. Laminoplasty decompresses the spinal cord while preserving the posterior tension band and reducing the risk of post-laminectomy kyphosis. It is indicated for multi-level cervical spondylotic myelopathy without significant kyphotic deformity.
Fusion and Fixation
Posterior cervical fusion techniques involve placing screws into the lateral masses or pedicles, connecting them with rods.
* Lateral Mass Screws: The most common method for subaxial cervical fusion (C3-C7). Various techniques exist (e.g., Magerl, Roy-Camille, An, Ebraheim), all aiming to place screws into the lateral mass safely, avoiding nerve roots and vertebral arteries. Screw trajectory typically involves a 30-45 degree angulation laterally and slightly superiorly.
* Pedicle Screws: Offer superior biomechanical pullout strength but require meticulous technique due to the proximity of the vertebral artery, spinal cord, and nerve roots. They are increasingly used in selected cases, particularly at C7, or in cases of severe osteoporosis.
* C1-C2 Fixation:
* Harms Technique (C1 lateral mass and C2 pedicle/pars screws): The most biomechanically rigid C1-C2 construct, indicated for unstable odontoid fractures, C1 ring fractures, or C1-C2 instability.
* Magerl Technique (C1-C2 transarticular screws): Requires reduction of the C1-C2 subluxation prior to screw insertion and carries a higher risk of vertebral artery injury.
* Gallie or Brooks fusion: Older techniques using wire fixation for C1-C2 fusion.
* Occipitocervical Fixation: Used for unstable injuries involving the occipitocervical junction or severe upper cervical instability. Screws are placed into the occipital bone (supra/infra-nuchal lines) and connected to rods extending into the lower cervical spine.
* Rod Contouring: Rods are contoured to restore physiological lordosis, and set screws are tightened to create a rigid construct. Bone graft (autograft, allograft) is placed over the decorticated posterior elements to promote fusion.
Complications and Management
Cervical spine surgery, despite advances, carries inherent risks. A thorough understanding of potential complications and their management is crucial for all orthopedic spine surgeons.
Intraoperative Complications
- Vertebral Artery Injury: Incidence 0.3-0.5% in subaxial cervical surgery. Can occur during screw placement (especially pedicle or transarticular screws), lateral mass dissection, or corpectomy. Management involves direct pressure, packing, or embolization. Neurological sequelae (stroke) are devastating.
- Spinal Cord Injury (New or Worsening Deficit): Incidence 0.1-0.5%. Can result from excessive manipulation, malreduction, direct cord trauma during decompression, or ischemia. Immediate cessation of instrumentation, careful reassessment of alignment, and potential removal of offending hardware are critical. Intraoperative neuromonitoring aids early detection.
- Nerve Root Injury: Incidence 1-5%. More common with posterior lateral mass screw placement or aggressive decompression. Manifests as motor weakness or sensory deficit in the affected dermatome/myotome. Management involves careful review of hardware position, potential removal of malpositioned screws.
- Esophageal Perforation: Rare but serious, primarily with anterior approaches. Can occur during retraction or direct injury. Presents with dysphagia, odynophagia, fever, or retropharyngeal air. Immediate recognition, surgical repair, and broad-spectrum antibiotics are necessary.
- Recurrent Laryngeal Nerve (RLN) Injury: Incidence 1-10% (transient), 0.1-1% (permanent) with anterior approach. Causes hoarseness or dysphonia. More common on the right side. Usually transient due to retraction. Persistent symptoms may require vocal cord injection.
- Dural Tear/CSF Leak: Incidence <1%. Can occur during decompression (laminectomy/corpectomy) or removal of osteophytes. Management includes primary repair with suture, dural substitutes, and tissue sealants. Postoperative bed rest and CSF diversion (lumbar drain) may be necessary.
- Hemorrhage: Can be significant, particularly from epidural venous plexuses or if major vessels are injured. Careful hemostasis and maintenance of normotension are key.
Early Postoperative Complications
- Infection: Superficial wound infection (2-5%), deep surgical site infection (0.5-2%). Risk factors include prolonged surgery, immunocompromise, and extensive dissection. Management involves antibiotics, wound debridement, and potentially hardware removal in chronic cases.
- Hematoma (Epidural, Retropharyngeal): Epidural hematoma can cause neurological deterioration post-op, requiring emergent re-exploration. Retropharyngeal hematoma (anterior approach) can cause acute airway compromise, potentially necessitating intubation or emergent tracheostomy.
- Dysphagia: Common after anterior cervical surgery (up to 70% transient, 1-5% persistent). Caused by direct trauma, recurrent laryngeal nerve injury, pharyngeal edema, or esophageal dysmotility. Management involves dietary modification, speech therapy, and occasionally, steroid administration.
- Airway Compromise: Can result from swelling (retropharyngeal edema, hematoma), recurrent laryngeal nerve palsy, or severe dysphagia leading to aspiration. Close postoperative monitoring and early intervention (e.g., re-intubation) are crucial.
- Nonunion/Pseudarthrosis: Failure of bony fusion. Incidence varies (5-20%) depending on patient factors, number of levels, and graft type. May present with persistent pain or hardware failure. Requires revision surgery (re-fusion, bone graft augmentation).
- Hardware Failure: Screw pullout, plate fracture, or migration. Often associated with nonunion or poor bone quality. Requires revision.
- C5 Palsy: Transient postoperative C5 radiculopathy (motor weakness in deltoid/biceps) affecting 5-10% of patients, particularly after posterior decompression for myelopathy. Etiology is multifactorial, including re-equilibration of neural tension. Usually resolves spontaneously within weeks to months.
Late Postoperative Complications
- Adjacent Segment Disease (ASD): Degeneration at levels adjacent to a fused segment, leading to pain, radiculopathy, or myelopathy. Incidence 2-4% per year. May eventually require surgery at the adjacent level.
- Chronic Pain: Persistent axial neck pain or radicular symptoms despite successful fusion.
- Deformity (Kyphosis): Can occur after extensive laminectomy without fusion, particularly in the pediatric population, or due to severe nonunion.
- Persistent Dysphagia: Rare but debilitating, may require long-term dietary modification or surgical intervention.
| Complication Category | Incidence (Approximate) | Salvage Strategies |
|---|---|---|
| Neurological Deficit | 0.1-0.5% (new/worsening SCI) | Immediate re-exploration, decompression, hardware adjustment; Neuromonitoring |
| Vertebral Artery Injury | 0.3-0.5% | Direct pressure, packing, embolization, urgent neurovascular consultation |
| Esophageal Perforation | <0.1% | Primary repair, drainage, broad-spectrum antibiotics; GI consultation |
| Recurrent Laryngeal Nerve Injury | 1-10% (transient) | Expectant management; Speech therapy; Vocal cord injection (persistent) |
| Dural Tear/CSF Leak | <1% | Primary repair, dural substitute, sealant; Lumbar drain; Bed rest |
| Airway Compromise/Hematoma | 0.5-2% | Emergent re-intubation, tracheostomy; Hematoma evacuation |
| Infection | 0.5-2% (deep) | Antibiotics, debridement, washout; Hardware removal (chronic) |
| Nonunion/Pseudarthrosis | 5-20% | Revision fusion, bone graft augmentation, re-instrumentation |
| Hardware Failure | 2-10% | Revision surgery, hardware replacement, re-fusion |
| C5 Palsy | 5-10% | Expectant management, physical therapy |
| Adjacent Segment Disease | 2-4% per year | Non-operative management; Revision surgery (decompression, fusion at new level) |
| Dysphagia (Persistent) | 1-5% | Speech therapy, dietary modification, steroid trial, possible surgical intervention |
Post Operative Rehabilitation Protocols
Postoperative rehabilitation is an integral component of cervical spine treatment, aiming to optimize recovery, restore function, and prevent recurrence or secondary complications. Protocols are individualized based on the surgical procedure, extent of injury, and patient factors.
Immobilization
The use of postoperative external immobilization varies. Following a single-level ACDF with stable plating, many surgeons allow early mobilization without a rigid collar. For multi-level fusions, corpectomies, posterior fusions, or unstable fracture fixations, a rigid cervical orthosis (e.g., Miami J, Aspen) is typically prescribed for 6-12 weeks to protect the construct during early healing. Halo-vest immobilization may be indicated after complex upper cervical fusions or highly unstable injuries for a prolonged period (3-6 months). Periodic radiographic evaluation confirms stability and progression of fusion.
Early Mobilization
Within the limits of external immobilization, patients are encouraged to ambulate and perform activities of daily living as tolerated. Emphasis is placed on proper posture and body mechanics. Early initiation of physical therapy focuses on pain management, reduction of muscle spasm, and gentle range of motion exercises for non-immobilized segments.
Physical Therapy
- Phase 1 (Protective Phase - 0-6 weeks): Focus on wound care, pain control, and education on spinal precautions. Gentle isometric neck exercises, scapular stabilization, and postural awareness are initiated. Avoidance of heavy lifting, twisting, and bending.
- Phase 2 (Intermediate Phase - 6-12 weeks): Once radiographic evidence of early fusion is apparent and clinical stability is achieved, supervised gentle active range of motion (AROM) exercises for the cervical spine are introduced. Strengthening of neck musculature (isometric progressing to isotonic) and upper extremity strengthening is advanced. Proprioceptive exercises and balance training may be incorporated.
- Phase 3 (Advanced Strengthening and Return to Activity - 12+ weeks): Gradual progression to full AROM, advanced strengthening, and endurance exercises. Functional training specific to the patient's occupational or recreational demands. High-impact activities or contact sports are typically restricted until complete radiographic fusion is confirmed (typically 6-12 months post-op) and sufficient strength and flexibility are regained.
Pain Management
A multimodal approach to pain management, including scheduled analgesics, muscle relaxants, and neuropathic pain medications, is crucial for patient comfort and participation in rehabilitation. Patient education on pain expectations and coping strategies is important.
Return to Activity and Sport
Return to full activity, particularly strenuous work or sport, is a phased approach and is highly individualized. It is contingent upon achieving solid radiographic fusion, resolution of pain, and restoration of adequate strength and flexibility. Serial imaging (flexion-extension radiographs, CT scans) may be used to confirm fusion prior to clearance for unrestricted activity. For athletes, a gradual return-to-sport protocol under supervision is recommended.
Summary of Key Literature and Guidelines
The management of cervical spine injuries has evolved significantly, driven by landmark studies and consensus guidelines from professional organizations.
The NASCIS II and III trials ignited a longstanding debate regarding the use of high-dose methylprednisolone for acute spinal cord injury. While initially suggesting some benefit, particularly if administered within 8 hours, subsequent re-analyses and larger reviews have largely refuted its routine use, citing lack of clear long-term neurological recovery benefit and increased complication rates. Current guidelines from the American Association of Neurological Surgeons (AANS) and the Congress of Neurological Surgeons (CNS) no longer recommend its routine administration but acknowledge it as an option if started within 8 hours of injury, after shared decision-making with the patient.
Regarding surgical timing, strong evidence supports early surgical decompression (within 24 hours) for acute cervical spinal cord injury, particularly in incomplete lesions, to improve neurological outcomes. This recommendation is supported by guidelines from AOSpine International and NASS (North American Spine Society).
For specific fracture types, randomized controlled trials and large observational studies inform treatment decisions:
* Odontoid Fractures: Type II odontoid fractures in elderly or osteoporotic patients, or those with significant displacement, often have poor nonunion rates with external immobilization and are frequently managed surgically with C1-C2 fusion (e.g., Harms technique) or odontoid screw fixation.
* Cervical Spondylotic Myelopathy: ACDF and posterior laminoplasty have demonstrated comparable clinical outcomes for multi-level myelopathy, with the choice influenced by sagittal alignment, number of levels, and specific morphology of compression. ACDF is generally favored for localized ventral compression with kyphosis, while laminoplasty is preferred for multi-level posterior compression with maintained lordosis.
* Adjacent Segment Disease (ASD): A common long-term sequela after cervical fusion. Studies suggest that biomechanical alterations and increased stress at adjacent levels contribute to its development. Newer motion-preserving devices (total disc arthroplasty) are being investigated as potential alternatives to fusion to mitigate ASD, with promising short- and mid-term results in selected patients, particularly for single-level disease in younger individuals.
Current practice emphasizes a patient-centric, evidence-based approach, integrating precise diagnostic imaging, appropriate surgical techniques when indicated, and structured rehabilitation protocols. Continuous research into biomechanics, novel fixation techniques, biological augmentation, and advanced neurological monitoring continues to refine the standard of care for cervical spine injuries and degenerative conditions.
Clinical & Radiographic Imaging