Thoracoscopic Anterior Release and Fusion for Scoliosis: An Operative Masterclass

Key Takeaway
This masterclass details thoracoscopic anterior release and fusion for scoliosis, guiding you through comprehensive patient assessment, meticulous preoperative planning, and precise intraoperative execution. We cover critical anatomical considerations, optimal patient positioning, advanced portal placement, and meticulous disc and endplate preparation. Learn to manage neurovascular structures, prevent complications, and ensure successful fusion. Postoperative rehabilitation and complication management are also thoroughly discussed, providing a complete surgical perspective.
Comprehensive Introduction and Patho-Epidemiology
Welcome, fellows, to the operating theater. Today, we are tackling a challenging yet incredibly rewarding procedure: the thoracoscopic anterior release and fusion for scoliosis. This is a powerful technique that allows us to achieve significant correction in complex spinal deformities, particularly in the thoracic spine, with the profound benefits of minimally invasive surgery. The paradigm of spinal deformity surgery has shifted dramatically over the last three decades. Historically, anterior spinal releases required extensive, morbid open thoracotomies, which carried significant risks of pulmonary compromise, severe post-operative pain, and shoulder girdle dysfunction. The advent of video-assisted thoracoscopic surgery (VATS) for spinal applications has revolutionized our approach, allowing us to achieve equivalent, if not superior, anterior column mobilization while dramatically reducing approach-related morbidity. Understanding the nuances, mastering the endoscopic technique, and anticipating potential pitfalls are paramount for any modern spinal deformity surgeon.
Scoliosis is defined as a complex, three-dimensional lateral curvature of the spine accompanied by obligate axial plane rotation and, frequently, sagittal plane alterations such as thoracic hypokyphosis. While curve progression can be slow—approximately 1 degree per year in skeletally mature patients—it can be explosive during periods of significant adolescent spine growth, particularly during the peak height velocity phase. Curves exceeding 80 to 90 degrees in the thoracic spine often lead to symptomatic pulmonary issues, right-sided heart strain, and restrictive lung disease. Furthermore, large curves progressing into adulthood are frequently associated with debilitating, asymmetric facet arthropathy and radicular pain.

The fundamental goal with an anterior release is to enhance the flexibility of the spinal column, allowing for greater coronal and sagittal correction during the subsequent posterior instrumentation and fusion. The release involves the meticulous, systematic removal of the annulus fibrosus, the anterior longitudinal ligament (ALL), the nucleus pulposus, and, when indicated, the rib head at the apex of the deformity. Fusion, the ultimate biological endpoint, is the solid arthrodesis of two adjacent vertebral bodies, typically achieved with autogenous bone graft, allograft, or a suitable osteoinductive bone graft substitute. Without a robust anterior fusion mass, even the most rigid posterior constructs are destined to fail via pseudoarthrosis or hardware fracture.
While adolescent idiopathic scoliosis (AIS) is the most common etiology we encounter, we must always stratify our approach based on pathogenesis. Congenital scoliosis, arising from failures of vertebral formation (e.g., hemivertebrae) or segmentation (e.g., unsegmented bars), presents unique anatomical challenges that often necessitate anterior intervention. Neuromuscular scoliosis, seen in patients with cerebral palsy or Duchenne muscular dystrophy, often results in long, sweeping, rigid curves extending to the pelvis. Neurogenic scoliosis, associated with conditions like neurofibromatosis or Chiari malformations, can present with sharp, dystrophic curves that are notoriously resistant to posterior-only correction. Recognizing the underlying patho-epidemiology dictates not only the necessity of the anterior release but also the choice of fusion levels and biological graft materials.

Detailed Surgical Anatomy and Biomechanics
The thoracic spine, extending from T1 to T12, is an anatomically complex and unforgiving region. Understanding its intricate osteology, discoligamentous structures, and adjacent visceral anatomy is the absolute foundation for safe and effective thoracoscopic surgery. The rib head attachment to the vertebral body is a critical anatomical landmark that dictates our dissection planes. In the proximal thoracic spine (T1-T5), the rib head articulates more anteriorly on the vertebral body compared to the distal thoracic spine (T6-T12), where it sits more posteriorly, bridging the disc space and the adjacent vertebral bodies. This subtle but crucial osteological difference impacts our approach to apical rib head resection, which is often necessary to achieve maximal derotation and coronal flexibility.
Deep within the intervertebral space lies the disc, composed of the tough, circumferential annulus fibrosus surrounding the gelatinous, hydrophilic nucleus pulposus. Ventrally, the strong, contiguous anterior longitudinal ligament (ALL) runs the entire length of the spine, providing significant resistance to extension and distraction. During our thoracoscopic release, we must meticulously incise the annulus and completely resect the ALL at the targeted levels. Failure to completely section the ALL, particularly on the contralateral side of the curve, will severely limit the flexibility gained from the discectomy and tether the spine during the posterior correction maneuver.
Crucially, the spinal surgeon must be acutely aware of the surrounding neurovascular anatomy. The segmental arteries and veins originate directly from the descending aorta and the inferior vena cava (or azygous/hemiazygous systems), respectively. They traverse the waist of the vertebral bodies horizontally. These vessels are critical for spinal cord perfusion via the radiculomedullary arteries, most notably the Artery of Adamkiewicz, which typically arises between T8 and L1 on the left side. The parietal pleura of the chest cavity intimately covers these segmental vessels, the intervertebral discs, and the vertebral bodies. Our initial dissection involves sharply incising this pleura to expose the underlying spinal column, requiring meticulous hemostasis.
From a biomechanical perspective, the anterior column is the primary load-bearing structure of the spine. In severe scoliosis, structural changes occur within the anterior column, including wedge-shaped deformation of the vertebral bodies and contracture of the discoligamentous complex on the concavity of the curve. An anterior release biomechanically destabilizes the spine in a controlled manner. By removing the anterior tether (the ALL and annulus) and creating a void (the discectomy), we convert a rigid, structural deformity into a flexible, non-structural one. This allows the subsequent posterior instrumentation to act as a powerful lever, translating and derotating the spine into a more physiological alignment, particularly restoring thoracic kyphosis which is often lost in AIS.

Exhaustive Indications and Contraindications
The decision to proceed with a thoracoscopic anterior release is highly nuanced and must be tailored to the individual patient's deformity characteristics, skeletal maturity, and overall physiological reserve. We reserve this advanced procedure for specific, well-defined indications where posterior-only approaches are deemed insufficient or carry an unacceptably high risk of failure.
| Category | Specific Criteria | Rationale |
|---|---|---|
| Indications | Severe Rigid Deformity (Cobb > 80-90°, Flexibility < 30%) | Posterior-only forces cannot overcome the anterior soft tissue and bony contractures. Anterior release dramatically improves the flexibility index. |
| Skeletal Immaturity (Risser 0, Open Triradiate Cartilage) | Prevents the "Crankshaft Phenomenon." In very young patients, posterior fusion tethers the posterior elements while the anterior column continues to grow, causing progressive rotational deformity. | |
| Deficient Posterior Elements (Spina Bifida, Post-Laminectomy) | Lack of posterior bone stock precludes adequate posterior instrumentation and fusion. Anterior fusion provides the necessary structural support and arthrodesis bed. | |
| Severe Thoracic Hypokyphosis/Lordosis | Anterior release allows for shortening of the anterior column and restoration of normal sagittal thoracic kyphosis during posterior compression. | |
| Contraindications | Severe Pulmonary Compromise (Absolute) | Inability to tolerate single-lung ventilation. Patients with severe restrictive lung disease may decompensate intraoperatively. |
| Prior Ipsilateral Thoracotomy/Pleurodesis (Relative) | Dense pleural adhesions obliterate the thoracoscopic working space and dramatically increase the risk of lung parenchymal injury. | |
| Bleeding Diatheses (Relative) | Thoracoscopic hemostasis can be challenging; severe coagulopathies must be corrected prior to surgery. | |
| High Thoracic Curves (T1-T3) (Relative) | Anatomical constraints (thoracic inlet, subclavian vessels) make thoracoscopic access to the uppermost thoracic vertebrae exceedingly difficult and dangerous. |
Severe spinal deformity remains the primary indication. When we evaluate a patient with a thoracic curve exceeding 80 to 90 degrees, or a kyphotic deformity greater than 100 degrees, we critically analyze the flexibility index on dynamic imaging (supine side-bending or traction films). If the curve demonstrates less than 30% to 50% flexibility, it is considered highly rigid. Attempting to correct such a stiff curve from a posterior approach alone places immense stress on the pedicle screws and bone-metal interface, risking catastrophic hardware pullout, pedicle fracture, or failure to achieve coronal balance. The anterior release effectively "unlocks" the spine.

Skeletal immaturity is another critical indication, particularly in children younger than 10 years of age. In these patients, the triradiate cartilage is widely open, and they are typically Risser grade 0, indicating immense remaining growth potential. If we perform a posterior-only fusion in this demographic, we halt posterior growth, but the anterior vertebral bodies continue to grow. This biomechanical mismatch leads to the "crankshaft phenomenon," where the spine twists around the posterior fusion mass, resulting in worsening rotational deformity and rib hump despite a solid posterior arthrodesis. An anterior release and fusion effectively arrests this anterior growth, preventing this devastating complication.

Conversely, we must rigorously respect the contraindications. The most absolute contraindication is the patient's inability to tolerate single-lung ventilation. During the thoracoscopic procedure, the ipsilateral lung must be completely deflated to create a working cavity. Patients with severe pre-existing restrictive or obstructive pulmonary disease may experience profound hypoxia or hemodynamic instability when dependent on a single lung. Thorough preoperative pulmonary function testing (PFTs) and consultation with a specialized pediatric or neuro-anesthesiologist are mandatory. Prior ipsilateral thoracotomy or empyema often results in dense pleural adhesions, making safe endoscopic port placement and lung retraction nearly impossible without causing severe parenchymal tears.
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Evaluation and Imaging
Before we even consider making an incision, a thorough, exhaustive understanding of the patient's history, physical findings, and imaging is crucial. This is where we build our roadmap for success. We begin with a detailed patient history, focusing not only on the deformity but on the character of any associated pain. Is it sharp, dull, or aching? Does it occur during activity or wake them from sleep? Night pain is a red flag that demands investigation for osteoid osteoma, osteoblastoma, or intraspinal tumors. Critically, we must ascertain if the pain radiates into the extremities, suggesting neural compression or tethering.

A comprehensive neurologic examination is non-negotiable. This includes rigorous motor strength testing, sensory mapping, and reflex evaluation of all extremities. The abdominal reflexes are a particularly important assessment in the scoliosis population. We assess them by stroking the skin adjacent to the umbilicus in all four quadrants. They should be symmetrically present. Any asymmetry, or the presence of pathological reflexes like a positive Babinski or sustained clonus, necessitates an immediate total spine MRI to evaluate for neural axis abnormalities such as a syrinx, tethered cord, or Chiari malformation.

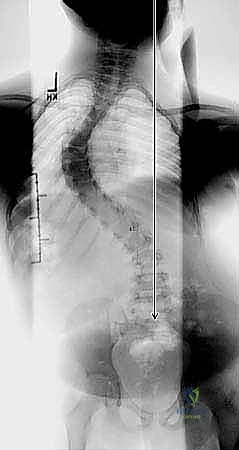
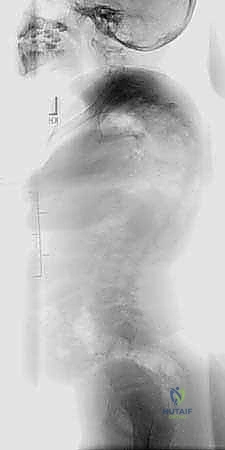
Our imaging workup begins with standing posteroanterior (PA) and lateral radiographs of the entire spine on a single 36-inch cassette. We meticulously measure coronal plane deformities using the Cobb method and assess overall trunk balance by evaluating the C7 plumb line in relation to the center sacral vertical line (CSVL). We determine skeletal maturity using the Risser stage (0 through 5). For severe deformities with significant rotation, the Stagnara view (an oblique view orthogonal to the true apical coronal curve) is invaluable for accurately assessing the true magnitude of the curve. Advanced imaging, specifically MRI, is routinely utilized to rule out intraspinal pathology, while high-resolution CT scanning provides a detailed 3D roadmap of the osseous anatomy, crucial for planning rib head resections and understanding distorted pedicle morphology.
Anesthetic Considerations and Positioning
The anesthetic management for thoracoscopic anterior spine surgery is highly specialized. The cornerstone of the procedure is achieving effective single-lung ventilation. Our anesthesiologist will intubate the patient with a double-lumen endotracheal tube or utilize a bronchial blocker (univent tube). Proper placement is confirmed via flexible bronchoscopy. We must ensure the ability to selectively and completely collapse the ipsilateral lung to expose the thoracic spine. Continuous intraoperative neuromonitoring, including somatosensory evoked potentials (SSEPs) and motor evoked potentials (MEPs), is standard of care to monitor spinal cord integrity throughout the release and subsequent correction.

The lateral decubitus position is the standard approach. The patient is positioned with the convexity of the curve facing upwards. For example, a typical right thoracic curve requires a left lateral decubitus position (right side up). An axillary roll is placed to protect the dependent brachial plexus, and all bony prominences are meticulously padded. The patient is secured to the operating table using deflatable bean bags and wide adhesive tape to allow for table tilting during the procedure. The surgeon and assistant typically stand facing the patient's anterior chest, while the endoscopic tower is positioned directly across from them, behind the patient's back.

Portal placement must be meticulously planned based on preoperative imaging and intraoperative fluoroscopy. We generally utilize three to four portals placed along the anterior, middle, and posterior axillary lines. The portals must be triangulated to allow for ergonomic instrument manipulation without "sword-fighting." The optical portal (for the 30-degree endoscope) is usually placed centrally, while working portals are placed superiorly and inferiorly. The exact intercostal spaces chosen depend on the specific levels requiring release; typically, portals are placed one or two intercostal spaces above and below the planned extremes of the release.

Step-by-Step Surgical Approach and Fixation Technique
Portal Placement and Initial Exposure
Following sterile prep and drape, local anesthetic is infiltrated at the planned portal sites. Small, 1.5 cm incisions are made, and blunt dissection is carried down over the superior margin of the rib to avoid the intercostal neurovascular bundle. We introduce a blunt trocar, followed by the 30-degree endoscope. Under direct visualization, the remaining working portals are established. The ipsilateral lung is deflated, and a fan retractor is introduced to gently retract the lung anteriorly and medially, exposing the posterior mediastinum and the scoliotic spine.

Initial orientation is critical. We identify the major vascular landmarks: the descending aorta (if on the left) or the azygous vein (if on the right). The sympathetic chain is visualized running longitudinally over the heads of the ribs. We confirm our spinal levels using fluoroscopy, marking the targeted discs. The parietal pleura overlying the spine is then incised longitudinally over the apex of the deformity. Using endoscopic blunt dissectors and Kittner sponges, we elevate anterior and posterior pleural flaps to expose the vertebral bodies and the intervening intervertebral discs.

As we expose the vertebral bodies, we encounter the segmental vessels traversing the waist of each vertebra. Management of these vessels is a subject of debate. While some surgeons advocate for routine ligation (using endoscopic clips or an ultrasonic scalpel) to maximize exposure, others prefer to mobilize them and work within the "safe zones" between the vessels to preserve collateral spinal cord blood flow. If ligation is necessary, the vessels must be isolated, doubly clipped, and transected cleanly. Care must be taken not to avulse these vessels from the aorta, which can lead to catastrophic, difficult-to-control hemorrhage.


Discectomy and Anterior Release
The core of the procedure is the discectomy and anterior release. We begin by incising the annulus fibrosus in a rectangular fashion using an endoscopic electrocautery or a long-handled annulotomy knife. The incision must extend from the posterior longitudinal ligament (PLL) to the anterior longitudinal ligament (ALL). Once the annulus is incised, we use endoscopic pituitary rongeurs and straight/angled curettes to aggressively remove the nucleus pulposus.

Endplate preparation is a meticulous process. We must remove all cartilaginous endplate material down to bleeding subchondral bone to create a biologically active bed for fusion. However, we must strictly avoid violating the structural integrity of the bony endplate. Excessive decortication can lead to graft subsidence and loss of correction. We utilize specialized Cobb elevators and ring curettes to scrape the endplates clean, working systematically from posterior to anterior.


To achieve a true "release," the ALL must be completely resected. This is often the most challenging part of the procedure, as the ALL is thick and closely related to the great vessels anteriorly. Using a combination of blunt dissection and electrocautery, the ALL is sectioned until the anterior margin of the contralateral annulus is visualized. At the apex of severe, rigid curves, we may also perform a rib head resection. The radiate ligament is incised, and the rib head is removed using a high-speed endoscopic burr or rongeurs. This disconnects the rib cage from the spine, providing profound rotational and coronal flexibility.

Fusion, Grafting, and Closure
Once the release is complete across all planned levels, the disc spaces must be grafted to ensure arthrodesis. The choice of graft material varies. Autogenous rib graft, harvested from the portal sites or via a separate small incision, is the gold standard. Alternatively, structural allograft, demineralized bone matrix (DBM), or bone morphogenetic protein (BMP) on a collagen sponge can be utilized. The graft material is tightly packed into the empty disc spaces using endoscopic tampers. Adequate volume is crucial; the disc space should be filled to provide structural support and a robust biological fusion mass.


Following grafting, meticulous hemostasis is obtained. The pleural cavity is irrigated with warm saline, and the fluid is suctioned to ensure no active bleeding from the epidural space or segmental vessels. We carefully inspect the lymphatic channels for any signs of a chyle leak, particularly when operating in the lower thoracic spine near the cisterna chyli. Some surgeons prefer to loosely reapproximate the parietal pleura over the grafted disc spaces using endoscopic suturing or clips to contain the graft material, though this is not strictly necessary if the graft is tightly packed.



