Spondylodiscitis: Deciphering the next course of action

Key Takeaway
Your ultimate guide to Spondylodiscitis: Deciphering the next course of action starts here. For spondylodiscitis without neurological deficits, epidural abscess, or gross deformity, and with positive blood cultures for methicillin-sensitive *S. aureus*, the next course of action involves infectious disease consultation to optimize antibiotic therapy. Vancomycin is unnecessary; a more appropriate antibiotic should be selected based on sensitivity. Surgical debridement and fusion are generally not indicated at this time.
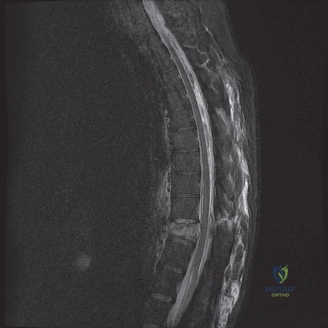
A 48-year-old female presents with severe, unrelenting low back pain, fevers, and chills. Her BMI is 43 and she has poorly controlled diabetes mellitus. You suspect spondylodiscitis. What is the most common underlying pathogenesis of this condition, and what specific anatomical structure facilitates bacterial seeding?
Candidate: The infection is usually caused by hematogenous spread of bacteria. The bacteria reach the spine through the blood and settle in the disc space, eventually infecting the vertebral bodies.
Failing to mention the subchondral endplate. Simply saying "the disc" is incorrect; the disc is avascular in adults, meaning the primary bacterial seeding site is the endplate's terminal arterial arcades.
The primary mechanism is hematogenous dissemination. The subchondral endplate is the critical site of bacterial seeding due to the sluggish blood flow in the terminal arterial arcades. From there, the infection breaches the endplate and invades the relatively avascular intervertebral disc, which serves as a nutrient-rich sanctuary shielded from the host immune response.
Your patient is neurologically intact with confirmed MSSA spondylodiscitis at L4-L5. Radiographs show stable alignment. What are the formal indications to proceed with surgical intervention in this case?

Candidate: Surgery is indicated if the patient has weakness, a big abscess, or if the spine is collapsing. Also if the antibiotics aren't working.
Using vague terms like "big abscess" or "antibiotics not working." An FRCS candidate must use precise clinical criteria: progressive neurological deficit, symptomatic compression (Cauda Equina), progressive kyphotic deformity (>15 degrees), or failure of medical management (persistent bacteremia/elevated inflammatory markers).
Surgery is indicated for: 1) Progressive neurological deficit or Cauda Equina Syndrome; 2) Symptomatic epidural abscess; 3) Failure of medical management (persistent bacteremia or rising CRP/ESR despite culture-directed antibiotics); 4) Progressive mechanical instability or focal kyphosis (>15 degrees); 5) Intractable pain unresponsive to rigid orthosis and analgesia.
When performing the surgical debridement, how do you handle the choice of interbody spacer in the setting of an active infection?

Candidate: You should avoid putting any metal in an infected spine because it will just harbor bacteria. I would use bone graft only, or wait until the infection is cleared before putting in a cage.
Outdated "dogma." Candidates often fear metal, but modern evidence demonstrates that titanium cages are safe in the infected setting following radical debridement and appropriate antibiotic coverage.
While historically cautioned against, the current standard of care supports the use of titanium interbody cages in the setting of infection. Titanium resists bacterial colonization compared to other materials and provides the necessary anterior column structural support to correct kyphosis. Success relies on radical debridement to bleeding bone and the administration of culture-directed, systemic antibiotics.
