Orthopedic Trauma 2026 MCQs: Board Review Questions & Answers (Part 4)
Key Takeaway
Here are the crucial details you must know about Orthopedic Trauma 2026 MCQs: Board Review Questions & Answers (Part 4). Top-rated Orthopedic Trauma 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Trauma 2026 MCQs: Board Review Questions & Answers (Part 4)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 30-year-old woman sustains a transverse amputation of the distal phalanx of the index finger, leaving exposed bone. What is the most appropriate management of the soft-tissue defect?
Explanation
Question 2
What is the best approach to reduce and stabilize a displaced volar lunate facet fracture of the wrist?
Explanation
Question 3
A 17-year-old man sustained a 5-mm laceration on the lateral aspect of the hindfoot while working on a farm. Examination in the emergency department revealed no fractures. Twenty-four hours later, he returns to the emergency department with increasing foot pain. Thin brown drainage is seen emanating from the wound. He has a temperature of 102.0 degrees F (38.9 degrees C), a pulse rate of 120, and a blood pressure of 80/40 mm Hg. Examination of the foot reveals diffuse swelling, ecchymosis, tenderness, and crepitus with palpation. Current radiographs are shown in Figures 40a and 40b. Management should now consist of
Explanation
Question 4
A healthy, active, independent 74-year-old woman fell and sustained the elbow injury shown in Figures 41a and 41b. Management should consist of
Explanation
Question 5
A 35-year-old man sustains a closed Monteggia fracture. Examination reveals that sensation, vascular status, and finger flexion are normal. When he extends his wrist, it deviates radially, and he is unable to extend his fingers or thumb. After reduction of the fracture, what is the next step in treatment for the extensor deficits of the thumb and fingers?
Explanation
Question 6
A 25-year-old man is brought to the emergency department following a motor vehicle accident. Extrication time was 2 hours, and in the field he had a systolic blood pressure by palpation of 90 mm Hg. Intravenous therapy was started, and on arrival in the emergency department he has a systolic blood pressure of 90 mm Hg with a pulse rate of 130. Examination reveals a flail chest and a femoral diaphyseal fracture. Ultrasound of the abdomen is positive. The trauma surgeons take him to the operating room for an exploratory laparotomy. At the conclusion of the procedure, he has a systolic pressure of 100 mm Hg with a pulse rate of 110. Oxygen saturation is 90% on 100% oxygen, and he has a temperature of 95.0 degrees F (35 degrees C). What is the recommended treatment of the femoral fracture at this time?
Explanation
Question 7
A 10-year-old girl has a right elbow deformity that is the result of trauma 5 years ago. She has no pain despite the arm deformity. The radiographs in Figures 42a and 42b show complete healing. This radiographic appearance demonstrates what complication?
Explanation
Question 8
A 64-year-old woman has left wrist pain and deformity after falling on her hand. Examination shows intact skin and no neurologic or vascular injuries. Radiographs are shown in Figures 43a and 43b. What is the most appropriate management for the injury?
Explanation
Question 9
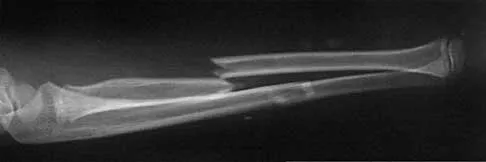
A 26-year-old man was thrown from a car and sustained the injury seen in Figures 44a and 44b. Nonsurgical management of this injury is recommended. Which of the following factors increases the risk of nonunion?
Explanation
Question 10
A 13-year-old girl was riding on an all-terrain vehicle when the driver struck a tree. She sustained the injury shown in Figures 45a through 45d. This injury is best described as what type of acetabular fracture pattern?
Explanation
Question 11
A woman injures the metacarpophalangeal (MCP) joint of her thumb while skiing. Examination reveals tenderness along the ulnar aspect of the MCP joint. Radially directed stress of the joint in full extension produces 5 degrees of angulation. When the MCP joint is flexed 30 degrees, a radially directed stress produces 45 degrees of angulation. Radiographs are otherwise normal. Management should consist of
Explanation
Question 12
A 37-year-old laborer falls 12 feet and sustains a comminuted tibial plafond fracture. Three years after treatment using standard techniques, what will be the most likely outcome?
Explanation
Question 13
A 45-year-old woman sustains an injury to her lower leg. Examination reveals that there is a deformity with no neurologic or vascular problems. The skin is intact. Radiographs are shown in Figures 46a and 46b. Which of the following factors would make closed management the least appropriate choice for this injury?
Explanation
Question 14
Which of the following medications may have a negative effect on bone healing following fracture?
Explanation
Question 15
A 16-year-old boy has abdominal and back pain after being involved in a high-velocity head-on motor vehicle accident. He was restrained in the rear of the automobile by a lap belt only. A radiograph and CT scan are shown in Figure 47. The patient has no other injuries. Optimal management should include
Explanation
Question 16
What inflammatory mediator has been most closely associated with the magnitude of the systemic inflammatory response to trauma and with the development of multiple organ dysfunction syndrome (MODS)?
Explanation
Question 17
An 8-year-old girl sustained a displaced fracture at the base of the femoral neck in a motor vehicle accident. Management should consist of
Explanation
Question 18
The plate seen in Figure 48a was applied to the fracture seen in Figure 48b, and is functioning in what capacity?
Explanation
Question 19
Which of the following findings is considered the strongest indication for surgical treatment of a mallet fracture of the distal phalanx?
Explanation
Question 20
A 20-year-old woman sustained the closed injury shown in Figures 49a and 49b in a motor vehicle accident. Examination reveals that this is an isolated injury; however, she has a complete radial nerve palsy. Management should consist of
Explanation
Question 21
The fracture shown in Figure 50 is most reliably treated with what form of fixation?
Explanation
Question 22
A man sustained the injury shown in Figures 51a and 51b. He underwent closed reduction of the radial head dislocation and open reduction and internal fixation of the ulnar fracture. What is the most common cause of persistent radial head subluxation?
Explanation
Question 23
Which of the following is an indication for surgical management of a Weber type B distal fibular fracture?
Explanation
Question 24
Locked plating techniques have been shown to have biomechanical advantages over standard plating in which of the following scenarios?
Explanation
Question 25
A 25-year-old man sustained a head injury after being ejected from his car. Examination reveals a Glasgow Coma Scale score of 7 and a swollen right knee. Clinical examination shows that the knee is very unstable, suggesting tears of the medial collateral and anterior and posterior cruciate ligaments, as well as the posterior lateral corner. What is the most appropriate first step to rule out a vascular injury?
Explanation
Question 26
A 35-year-old male is brought to the trauma bay after a high-speed motorcycle collision. His blood pressure is 80/50 mm Hg and heart rate is 125 beats/min. A FAST exam is negative for intra-abdominal fluid. An AP pelvic radiograph reveals an AP compression type III (APC-III) injury with severe symphyseal diastasis and disruption of both sacroiliac joints. A pelvic binder is appropriately applied. Following the administration of 2 liters of crystalloid and 2 units of uncrossmatched packed red blood cells, his blood pressure remains 85/55 mm Hg. What is the most appropriate next step in management?
Explanation
Question 27
A 65-year-old right-hand-dominant woman presents to the clinic 6 months after undergoing volar locking plate fixation for a displaced distal radius fracture. The fracture has healed well radiographically. She now reports a sudden inability to actively flex the interphalangeal (IP) joint of her thumb, though she has no pain. Which of the following technical errors during her index procedure is the most likely cause of this complication?
Explanation
Question 28
A 28-year-old male sustains a completely displaced transcervical femoral neck fracture following a fall from height. Radiographs demonstrate a vertical fracture line measuring 65 degrees relative to the horizontal (Pauwels type III). He undergoes closed reduction and internal fixation. Compared to a Pauwels type I fracture, what biomechanical environment predominates at the fracture site in this patient's injury?
Explanation
Question 29
A 42-year-old skier sustains a high-energy Schatzker VI tibial plateau fracture. On presentation, the leg is tense and markedly swollen. Compartment pressures are measured, yielding a delta P (diastolic blood pressure minus compartment pressure) of 15 mm Hg. A decision is made to perform a two-incision, four-compartment fasciotomy. During the anterolateral incision to release the anterior and lateral compartments, which of the following nerves is at greatest risk of iatrogenic injury?
Explanation
Question 30
A 68-year-old woman presents with a 4-part proximal humerus fracture. In evaluating the initial plain radiographs and CT scan, the surgeon assesses the risk of subsequent humeral head ischemia. According to the Hertel criteria, which of the following combinations of features is the most reliable predictor of avascular necrosis (AVN) of the humeral head?
Explanation
Question 31
A 24-year-old farm worker caught his leg in a tractor mechanism, sustaining a severely contaminated open diaphyseal tibia fracture with a 12-cm soft tissue defect and exposed bone (Gustilo-Anderson IIIB). Soil and organic matter are heavily ground into the wound. He is brought to the trauma center within 1 hour. According to evidence-based guidelines for initial antibiotic prophylaxis in this specific scenario, what is the most appropriate empiric intravenous regimen?
Explanation
Question 32
A 32-year-old male is 8 weeks post-operative from an open reduction and internal fixation of a displaced talar neck fracture (Hawkins type II). Routine follow-up radiographs demonstrate a subchondral radiolucent band in the dome of the talus on the AP view. What is the clinical significance of this radiographic finding?
Explanation
Question 33
A 45-year-old male falls from a ladder and sustains an acetabular fracture. The CT scan demonstrates a transverse fracture line across the acetabulum with a large, comminuted posterior wall fragment. The femoral head is subluxated posteriorly. The surgeon plans for open reduction and internal fixation. Which surgical approach provides the most direct access for anatomic reduction and plating of the involved columns in this fracture pattern?
Explanation
Question 34
A 30-year-old male presents to the emergency department after a direct blow to the leg during a rugby match. Radiographs show a closed, comminuted midshaft tibia fracture. He is complaining of agonizing pain despite receiving intravenous opioids. The nurse notes that his foot is swollen. Which of the following physical examination findings is the most sensitive early clinical indicator of acute compartment syndrome?
Explanation
Question 35
A 78-year-old woman with a history of a cemented left total hip arthroplasty performed 15 years ago falls from standing. Radiographs reveal a spiral periprosthetic femur fracture originating at the tip of the femoral stem and extending distally. The cement mantle is cracked, and the stem has subsided 1.5 cm into the canal, demonstrating gross radiographic loosening. However, the proximal femoral bone stock remains robust and circumferentially intact. According to the Vancouver classification, what is the classification of this fracture and the standard accepted treatment?
Explanation
Question 36
A 35-year-old male is brought to the emergency department after a high-speed motorcycle collision. His blood pressure is 70/40 mm Hg and heart rate is 135 bpm. A FAST exam is negative. An anteroposterior pelvic radiograph shows a widened pubic symphysis of 4 cm and widened bilateral sacroiliac joints. A pelvic binder is placed, and he receives 2 units of uncrossmatched packed red blood cells. His blood pressure improves transiently to 85/50 mm Hg. What is the next most appropriate step in management?
Explanation
Question 37
A 28-year-old man sustains a completely displaced, vertically oriented (Pauwels type III) femoral neck fracture after falling from a roof. He is taken to the operating room for closed reduction and internal fixation. Which of the following biomechanical constructs provides the most stable fixation for this specific fracture pattern?
Explanation
Question 38
A 42-year-old woman sustains a high-energy distal femur fracture. A CT scan of the knee reveals a displaced coronal plane fracture of the lateral femoral condyle. What is the most appropriate fixation strategy for this specific articular fragment?
Explanation
Question 39
A 33-year-old man sustains a Gustilo-Anderson Type IIIB open tibia fracture involving the distal third of the tibial diaphysis with a large 10x12 cm anterior soft tissue defect. After aggressive serial debridements and skeletal stabilization, he requires soft tissue coverage. Which of the following options is the most reliable soft tissue flap for this specific defect?
Explanation
Question 40
A 25-year-old snowboarder sustains a hyperdorsiflexion injury to his right ankle. Radiographs reveal a displaced fracture of the talar neck with subluxation of the subtalar joint. The tibiotalar and talonavicular joints remain congruent. According to the Hawkins classification, what is the approximate expected rate of avascular necrosis (AVN) of the talar body?
Explanation
Question 41
A 45-year-old male undergoes open reduction and internal fixation of a Schatzker VI tibial plateau fracture. Postoperatively, he requires rapidly increasing amounts of intravenous opioids. On examination, his leg is tense, and he experiences excruciating pain with passive stretch of his great toe. His dorsalis pedis pulse is palpable. Intracompartmental pressure testing shows an absolute pressure of 45 mm Hg in the anterior compartment, and his diastolic blood pressure is 65 mm Hg. What is the most appropriate next step?
Explanation
Question 42
A 62-year-old woman is evaluated 6 months after undergoing volar locked plating of a distal radius fracture. She reports the sudden inability to actively flex the interphalangeal joint of her thumb. She denies any new trauma. Lateral radiographs show that the distal edge of the volar plate is positioned prominent and distal to the watershed line. Which of the following is the most likely cause of her presentation?
Explanation
Question 43
A 78-year-old woman with a history of a cemented total hip arthroplasty performed 10 years ago falls and sustains a periprosthetic femur fracture. Radiographs demonstrate a fracture around the tip of the stem. The stem appears to be well-fixed with no evidence of cement mantle fracture or subsidence. According to the Vancouver classification, what is the most appropriate management for this injury?
Explanation
Question 44
A 22-year-old man presents to the emergency department after sustaining a single gunshot wound to the right knee. Radiographs reveal a retained bullet lodged entirely within the intra-articular space of the knee joint. There is no associated fracture. After appropriate initial tetanus prophylaxis and administration of antibiotics, what is the most appropriate definitive management of the retained bullet?
Explanation
Question 45
A 40-year-old construction worker sustains a displaced intra-articular calcaneus fracture (Sanders Type III). He is scheduled for open reduction and internal fixation utilizing a standard extensile lateral approach. Which of the following neurological structures is at greatest risk of iatrogenic injury during the creation and full-thickness elevation of this surgical flap?
Explanation
Question 46
A 45-year-old man is brought to the emergency department after a high-speed motorcycle collision. He is hemodynamically unstable with a blood pressure of 80/40 mm Hg and a heart rate of 125 beats/min. A FAST examination is negative. The anteroposterior pelvic radiograph reveals an Anteroposterior Compression Type III (APC-III) pelvic ring injury. A pelvic binder is ordered to assist with hemodynamic stabilization. What is the most appropriate anatomical landmark for the optimal placement of the pelvic binder to effectively reduce the pelvic volume?
Explanation
Question 47
A 38-year-old man sustains a closed, high-energy injury to his right knee. A computed tomography (CT) scan reveals a bicondylar tibial plateau fracture with a large, displaced posteromedial shear fragment. What is the most appropriate surgical approach to achieve anatomical reduction and stable buttress fixation of this specific posteromedial fragment?
Explanation
Question 48
A 75-year-old right-hand-dominant woman with a history of osteoporosis falls onto her shoulder. Radiographs demonstrate a displaced 4-part proximal humerus fracture with head-splitting components, severe comminution of the tuberosities, and a disrupted medial calcar hinge. Her pre-injury baseline was active and independent. Which of the following surgical options is associated with the most predictable restoration of forward elevation and pain relief in this patient?
Explanation
Question 49
A 25-year-old man sustains a vertical, displaced femoral neck fracture (Pauwels type III) after a fall from a height. He is taken to the operating room for closed reduction and internal fixation. Which of the following fixation constructs provides the greatest biomechanical stability against the predominant deforming forces for this specific fracture pattern?
Explanation
Question 50
A 32-year-old construction worker sustains a Gustilo-Anderson Type IIIB open tibia fracture. He undergoes immediate irrigation and debridement, and skeletal stabilization with an external fixator. Following sequential debridements, the wound bed is deemed clean, but there is exposed diaphyseal bone devoid of periosteum requiring a free tissue transfer. To minimize the risk of deep infection and flap failure, soft-tissue coverage should ideally be performed within what timeframe from the initial injury?
Explanation
Question 51
A 28-year-old man sustains a closed diaphyseal fracture of the tibia. Eight hours post-admission, he complains of worsening leg pain that is out of proportion to the injury and not relieved by intravenous opioids. Examination reveals tense calf compartments and excruciating pain with passive dorsiflexion of the hallux. His blood pressure is 110/70 mm Hg. Intracompartmental pressure monitoring is obtained. Which of the following pressure readings provides the strongest absolute indication for emergent fasciotomy?
Explanation
Question 52
A 40-year-old woman undergoes open reduction and internal fixation for an unstable pronation-external rotation ankle fracture. Intraoperatively, the external rotation stress test demonstrates widening of the medial clear space and the distal tibiofibular articulation. Syndesmotic fixation is planned. Which of the following statements is true regarding syndesmotic reduction and fixation?
Explanation
Question 53
An 82-year-old woman with severe rheumatoid arthritis and baseline limited household mobility sustains a highly comminuted, intra-articular distal femur fracture (OTA/AO 33-C3) after a fall. Her bone stock is extremely osteopenic. What is the primary advantage of choosing a distal femoral replacement (DFR) over open reduction and internal fixation (ORIF) with a lateral locking plate in this specific patient?
Explanation
Question 54
A 19-year-old competitive cyclist falls onto his left shoulder. Radiographs reveal a completely displaced midshaft clavicle fracture. Which of the following radiographic findings is the strongest relative indication for operative intervention (ORIF) over nonoperative management to optimize functional recovery and minimize the risk of symptomatic nonunion?
Explanation
Question 55
A 22-year-old man sustains a low-velocity handgun wound to the right thigh. His hemodynamics are stable, and neurovascular examination is entirely intact. Radiographs show a midshaft femur fracture with a retained bullet fragment situated within the vastus intermedius muscle belly. There is no evidence of intra-articular extension or compartment syndrome. What is the most appropriate initial management?
Explanation
Question 56
A 45-year-old man is brought to the trauma bay after a high-speed motorcycle collision. His blood pressure is 80/40 mm Hg and his heart rate is 135 bpm. Despite receiving 2 units of uncrossmatched packed red blood cells, he remains hemodynamically unstable. A pelvic binder has been applied. The FAST exam is negative. An AP pelvis radiograph reveals an APC-III (open-book) pelvic ring injury with wide disruption of the pubic symphysis and bilateral sacroiliac joints. What is the most appropriate next step in management?
Explanation
Question 57
A 28-year-old male sustains a vertically oriented, displaced femoral neck fracture (Pauwels type III) in a motor vehicle accident. He is scheduled for surgical fixation. According to biomechanical studies, which of the following constructs provides the greatest stability for this specific fracture pattern?
Explanation
Question 58
A 35-year-old construction worker sustains a highly comminuted midshaft tibia fracture with a 12 cm anterior soft-tissue defect exposing bone (Gustilo-Anderson type IIIB) after a crush injury. He undergoes emergent irrigation, debridement, and placement of an external fixator. Serial debridements render the wound bed clean. To minimize the risk of deep infection and flap failure, what is the optimal timing for definitive soft-tissue coverage?
Explanation
Question 59
A 65-year-old woman undergoes open reduction and internal fixation of a 3-part proximal humerus fracture using a lateral deltoid-splitting approach and a locking plate. Postoperatively, she demonstrates a positive Hornblower's sign (inability to actively maintain external rotation of the arm in 90 degrees of abduction). Which nerve is most likely to have been injured?
Explanation
Question 60
A 32-year-old male is admitted with a closed diaphyseal tibia fracture. Twelve hours later, he complains of severe, unrelenting leg pain that is exacerbated by passive stretch of his toes. The clinical suspicion for acute compartment syndrome is high, and continuous compartment pressure monitoring is initiated. Which of the following pressure measurements is the most widely accepted threshold indicating the need for an emergent fasciotomy?
Explanation
Question 61
An 80-year-old woman with severe osteoporosis presents to the emergency department after a fall. Radiographs reveal a highly comminuted, intra-articular distal femur fracture (AO/OTA 33-C3) with profoundly poor bone stock. Prior to the injury, she used a walker for short-distance ambulation. Which of the following surgical interventions will best allow for immediate, full weight-bearing in this patient?
Explanation
Question 62
A 34-year-old male who sustained a Hawkins type II talar neck fracture 8 weeks ago returns for a follow-up clinic visit. His AP ankle radiograph reveals a distinct subchondral radiolucent band in the dome of the talus. What does this radiographic finding indicate?
Explanation
Question 63
A 22-year-old collegiate football player sustains a high-energy foot injury. Advanced imaging reveals a purely ligamentous Lisfranc injury with complete disruption of the Lisfranc ligament complex and dorsal subluxation of the 1st, 2nd, and 3rd tarsometatarsal (TMT) joints. Based on recent prospective evidence, which of the following is the most appropriate primary surgical management?
Explanation
Question 64
A 28-year-old farmer sustains a Gustilo-Anderson Type IIIA open tibia fracture after his leg is caught in a tractor implement. The wound is heavily contaminated with soil and manure. He is brought to the emergency department for initial resuscitation. In addition to prompt surgical debridement, which of the following prophylactic antibiotic regimens is classically recommended for this specific injury pattern?
Explanation
Question 65
A 35-year-old man falls from a roof and sustains a severely comminuted, joint-depressed intra-articular calcaneus fracture (Sanders Type IV). Due to his heavy smoking history and poorly controlled diabetes, a shared decision is made to proceed with nonoperative management. What is the most common long-term clinical consequence of managing this displaced intra-articular fracture nonoperatively?
Explanation
Question 66
A 45-year-old man is brought to the trauma bay after a high-speed motorcycle collision. He has a heart rate of 130 bpm and a blood pressure of 80/50 mm Hg. A pelvic radiograph demonstrates an anteroposterior compression type III (APC-III) pelvic ring injury. A pelvic binder is applied, but his blood pressure remains 85/50 mm Hg after initial fluid resuscitation. A Focused Assessment with Sonography for Trauma (FAST) examination is negative. What is the next best step in management?
Explanation
Question 67
A 35-year-old woman sustains a high-energy Schatzker VI tibial plateau fracture. Upon admission, her leg is severely swollen and tense. Her current diastolic blood pressure is 60 mm Hg. Intracompartmental pressure measurement of the anterior compartment of the lower leg is 35 mm Hg. What is the most appropriate management of her lower extremity?
Explanation
Question 68
A 28-year-old man sustains a displaced, vertically oriented (Pauwels type III) femoral neck fracture after a fall from a height. He is an otherwise healthy construction worker. To minimize the risk of shear-related fixation failure and subsequent nonunion, which of the following is the most biomechanically appropriate surgical fixation construct?
Explanation
Question 69
A 42-year-old agricultural worker sustains a severe open tibia fracture (Gustilo-Anderson IIIB) that is heavily contaminated with soil and manure. He arrives at the emergency department within 1 hour of the injury. According to current trauma guidelines, what is the most appropriate initial intravenous antibiotic regimen?
Explanation
Question 70
A 22-year-old collegiate football player sustains a hyperplantarflexion injury to his midfoot. Radiographs demonstrate widening of the interval between the bases of the first and second metatarsals. Weight-bearing views confirm a 4-mm diastasis. MRI reveals complete disruption of the Lisfranc ligament complex without associated fractures. What is the most appropriate definitive surgical management?
Explanation
Question 71
A 60-year-old woman presents with persistent lower thigh pain 9 months after undergoing retrograde intramedullary nailing for a supracondylar distal femur fracture. Radiographs reveal a hypertrophic nonunion at the fracture site with abundant callus formation but a persistent fracture line. Laboratory markers for infection (CRP, ESR) are strictly normal. What is the most appropriate management?
Explanation
Question 72
A 34-year-old man sustains a Hawkins Type III fracture of the talar neck following a severe motor vehicle collision. In this specific injury pattern, which of the following blood vessels typically represents the ONLY remaining source of perfusion to the talar body?
Explanation
Question 73
A 45-year-old man falls onto an outstretched hand and sustains a distal radius fracture. CT imaging demonstrates a displaced volar marginal articular shear fracture (volar Barton's fracture) with associated volar subluxation of the carpus. What is the most appropriate surgical approach and fixation strategy?
Explanation
Question 74
A 72-year-old woman, who has been on alendronate therapy for 8 years, presents with atraumatic, persistent lateral thigh pain for the past 3 weeks. Radiographs reveal generalized cortical thickening and a transverse radiolucent line on the lateral cortex of the subtrochanteric femur. What is the most appropriate management to prevent a complete fracture?
Explanation
Question 75
A 50-year-old construction worker falls from a ladder, sustaining a severely comminuted, displaced intra-articular calcaneus fracture with a 3-cm laceration on the medial hindfoot exposing the fracture site. After immediate irrigation and debridement in the operating room, what is the most appropriate strategy for definitive fracture stabilization once the soft tissues permit?
Explanation
Question 76
A 28-year-old male presents with a hemodynamically unstable APC III pelvic ring injury following a high-speed motorcycle collision. Despite application of a pelvic binder and initiation of a massive transfusion protocol, he remains hypotensive. A Focused Assessment with Sonography for Trauma (FAST) exam is negative. He is taken emergently to the operating room for preperitoneal pelvic packing. Which of the following is the most likely anatomic source of his hemorrhage?
Explanation
Question 77
A 32-year-old female undergoes open reduction and internal fixation of a displaced talar neck fracture (Hawkins Type II). At her 8-week postoperative follow-up, an anteroposterior radiograph of the ankle is obtained. Which of the following radiographic findings serves as a reliable prognostic indicator that she will not develop clinically significant avascular necrosis (AVN) of the talar body?
Explanation
Question 78
A 42-year-old man sustains a complex acetabular fracture in a motor vehicle collision. Radiographs include an anteroposterior pelvis and Judet views. On the obturator oblique radiograph, a prominent "spur sign" is visualized. This pathognomonic finding is diagnostic of which fracture pattern, and what anatomical structure does the spur represent?
Explanation
Question 79
A 50-year-old woman is scheduled for open reduction and internal fixation of a medial tibial plateau fracture with posterior extension (Moore type I). The surgeon elects to use a posteromedial approach to the knee. The standard surgical interval for this approach is developed between which of the following two structures?
Explanation
Question 80
A 25-year-old male is admitted with a severe closed midshaft tibia fracture. Twelve hours later, he reports severe, escalating leg pain that is unresponsive to intravenous opioids and is exacerbated by passive stretch of his great toe. His compartment pressures are measured. Which of the following parameters represents an absolute indication for emergency four-compartment fasciotomy?
Explanation
Question 81
A 25-year-old healthy male sustains a vertically oriented basicervical femoral neck fracture (Pauwels type III) after a fall from a roof. The fracture is successfully closed reduced. Which of the following internal fixation constructs offers the highest biomechanical stability against vertical shear forces for this specific fracture pattern?
Explanation
Question 82
A 22-year-old collegiate football player sustains a hyperplantarflexion injury to his midfoot. Weight-bearing radiographs demonstrate a 3 mm diastasis between the base of the first and second metatarsals. Operative stabilization is planned. The primary stabilizing ligament of this articulation (the Lisfranc ligament) is correctly described by which of the following anatomic paths?
Explanation
Question 83
A 45-year-old male with poorly controlled type 2 diabetes presents with a highly comminuted, displaced tibial pilon fracture (OTA/AO 43-C3). On presentation, he has severe soft tissue swelling, skin tension, and fracture blisters. He undergoes initial spanning external fixation with fibular stabilization. What is the optimal clinical indicator that dictates the appropriate timing for definitive open reduction and internal fixation (ORIF) of the pilon?
Explanation
Question 84
A 28-year-old male presents with chronic radial-sided wrist pain 18 months after an untreated fall onto his outstretched hand. Imaging reveals a scaphoid waist nonunion with avascular necrosis of the proximal pole. He has an associated humpback deformity with a dorsal intercalated segment instability (DISI) pattern, but no radiocarpal arthritis. Which of the following surgical management strategies is most appropriate to restore carpal kinematics and achieve union?
Explanation
Question 85
During a standard volar (Henry) approach for open reduction and internal fixation of a distal radius fracture, the surgeon must carefully position the volar locking plate to minimize postoperative complications. Which of the following technical errors in plate placement is most strongly associated with late iatrogenic rupture of the flexor pollicis longus (FPL) tendon?
Explanation
Question 86
A 45-year-old male is brought to the trauma bay following a high-speed motorcycle collision. He is diagnosed with an APC III (Anteroposterior Compression type III) pelvic ring injury. Despite the application of a pelvic binder, 2 liters of warmed crystalloid, and 2 units of uncrossmatched packed red blood cells, his blood pressure remains 80/50 mm Hg with a heart rate of 130 bpm. A FAST (Focused Assessment with Sonography for Trauma) exam is negative. What is the most appropriate next step in the management of this patient?
Explanation
Question 87
A 28-year-old female sustains a vertical, displaced femoral neck fracture (Pauwels type III) during a fall from a height. She is taken to the operating room for definitive fixation. Which of the following fixation constructs provides the greatest biomechanical stability and highest load-to-failure for this specific fracture pattern?
Explanation
Question 88
A 78-year-old independent female with a 15-year history of severe rheumatoid arthritis falls onto her flexed elbow. Radiographs reveal a highly comminuted, intra-articular distal humerus fracture (OTA/AO type 13C3) with severe osteopenia. What is the most appropriate definitive management to maximize early function and minimize the need for revision surgery?
Explanation
Question 89
A 32-year-old man presents to the emergency department with severe ankle pain after an axial load injury. Radiographs show a displaced talar neck fracture with associated dislocation of both the subtalar and tibiotalar joints (Hawkins type III). What is the approximate reported rate of avascular necrosis (AVN) of the talar body associated with this specific injury pattern?
Explanation
Question 90
A 65-year-old woman with a 10-year history of alendronate use presents with a 3-month history of dull, aching right thigh pain. Plain radiographs reveal localized periosteal thickening of the lateral cortex of the subtrochanteric femur with a subtle transverse radiolucent line, but no complete fracture. What is the most appropriate prophylactic management?
Explanation
Question 91
A 40-year-old pedestrian is struck by a vehicle and sustains a severe, high-energy bicondylar tibial plateau fracture with metaphyseal-diaphyseal dissociation (Schatzker VI). Clinical examination reveals tense, severe swelling and extensive fracture blisters over the proximal leg. What is the most appropriate initial management?
Explanation
Question 92
A 25-year-old farmer sustains a severe open tibia fracture after a tractor rollover. The wound is 12 cm long with extensive muscle damage, heavy soil contamination, and exposed bone stripped of periosteum requiring a rotational flap for coverage (Gustilo-Anderson IIIB). Upon arrival in the emergency department, which of the following prophylactic antibiotic regimens is most traditionally appropriate?
Explanation
Question 93
A 35-year-old construction worker falls from a height of 15 feet, sustaining a closed, displaced, intra-articular calcaneus fracture (Sanders Type II). He is scheduled for ORIF via an extensile lateral approach. Which of the following strategies is most critical for decreasing the risk of postoperative wound complications?
Explanation
Question 94
A 55-year-old male presents with a pelvic injury following a motor vehicle collision. Standard AP and Judet views of the pelvis are obtained. On the obturator oblique radiograph, an intact segment of the ilium attached to the axial skeleton is visible, while the articular surface of the acetabulum is completely separated from it, creating a classic 'spur sign'. This radiographic finding is pathognomonic for which type of acetabular fracture?
Explanation
Question 95
A 24-year-old male undergoes intramedullary nailing of a closed diaphyseal tibia fracture. Six hours postoperatively, he complains of agonizing leg pain requiring rapidly escalating doses of IV narcotics. The pain is severely exacerbated by passive extension of the hallux. His blood pressure is 110/75 mm Hg. Intracompartmental pressure monitoring of the anterior compartment reveals a pressure of 55 mm Hg. What is the most appropriate definitive management?
Explanation
Question 96
A 32-year-old male sustains a closed, isolated Pauwels type III (vertical shear) femoral neck fracture following a high-energy fall. You are planning definitive surgical intervention. Which of the following internal fixation constructs provides the greatest biomechanical stability for this specific fracture pattern?
Explanation
Question 97
A 27-year-old male is involved in a high-speed motor vehicle collision and sustains a displaced talar neck fracture with subluxation of the subtalar joint. The tibiotalar and talonavicular joints remain congruent.
He undergoes urgent open reduction and internal fixation. At 8 weeks postoperatively, plain radiographs demonstrate a subchondral radiolucent band in the dome of the talus. What is the clinical significance of this radiographic finding?

Explanation
Question 98
A 42-year-old construction worker sustains an open middle-third tibia fracture (Gustilo-Anderson IIIB) after being struck by heavy machinery. Following serial thorough surgical debridements, the wound is clean and free of necrotic tissue, but there remains a 7 cm by 5 cm anterior soft tissue defect with exposed tibial bone devoid of periosteum.
What is the most appropriate method for providing soft-tissue coverage of this specific defect?

Explanation
Question 99
A 38-year-old male falls from a height of 20 feet and sustains a closed, highly comminuted intra-articular calcaneus fracture.
Surgical management with open reduction and internal fixation is planned utilizing a standard extensile lateral approach. During the surgical approach, creation of a full-thickness subperiosteal flap is critical to minimize wound healing complications. Which of the following structures is most at risk of injury and must be carefully identified and protected near the proximal aspect of the vertical limb of this incision?
Explanation
Question 100
A 72-year-old female with a 20-year history of severe rheumatoid arthritis presents to the emergency department after a mechanical fall onto her left arm. Radiographs demonstrate a closed, severely comminuted intra-articular fracture of the distal humerus (OTA/AO type 13C3) with profound osteopenia.
Given the patient's age, bone quality, and medical comorbidities, what is the most appropriate definitive surgical intervention?

Explanation
None
