Orthopedic Board Review: Mock Exam Set #936 - 100 Trauma MCQs

Key Takeaway
This page offers 100 high-yield orthopedic surgery multiple choice questions (MCQs) for ABOS, OITE, and FRCS board exams. Practice Set 936 helps surgeons master critical concepts, including multiple trauma care, and thoroughly prepare for certification and in-training assessments.
Multiple Trauma Patients: Essential Guide to ...
00:00
Start Quiz
A 50-year-old man with metastatic renal cell carcinoma has right hip pain. A radiograph and CT scan are shown in Figures 48a and 48b. The first step in management should consist of
Explanation
These lesions are extremely vascular and can cause uncontrolled intraoperative bleeding; therefore embolization is the appropriate first treatment. Because the radiograph and CT scan show a lytic lesion in the supra-acetabular region that affects the weight-bearing dome and medial wall, the next step in treatment would most likely be a total hip arthroplasty and acetabular reconstruction. Treatment with bisphosphonates and radiation therapy will not prevent an acetabular fracture. Cementoplasty is an emerging technique in which cement is injected percutaneously into a lesion, but no long-term results have been reported. Radiofrequency ablation of bone metastases is also an emerging technique that provides palliative pain control. Layalle I, Flandroy P, Trotteur G, Dondelinger RF: Arterial embolization of bone metastases: Is it worthwhile? J Belge Radiol 1998;81:223-225.
Question 3High Yield
A 52-year-old woman who is right hand-dominant sustains an injury to her elbow in a fall. A radiograph is shown in Figure 60. The preferred treatment of this injury pattern should include

Explanation
The patient has a Bado type 2 variant Monteggia fracture with a radial head fracture. The type 2 variant is associated with a higher nonunion rate and poorer outcomes compared to other Bado-type Monteggia fractures. While it is potentially acceptable to repair the radial head, factors such as higher degrees of comminution and older age lead toward replacement as the treatment of choice. Plate and screw fixation is favored over Kirschner wire/tension band fixation because this is not a simple olecranon fracture. Plate placement in a type 2 fracture is dorsal to counteract very high tensile forces associated with fixation failure. Egol KA, Tejwani NC, Bazzi J, et al: Does a Monteggia variant lesion result in a poor functional outcome? A retrospective study. Clin Orthop Relat Res 2005;438:233-238. Jupiter JB, Leibovic SJ, Ribbans W, et al: The posterior Monteggia lesion. J Orthop Trauma 1991;5:395-402.
Question 4High Yield
A 7-year-old girl who sustained a type III posteromedial extension supracondylar fracture underwent a closed reduction at the time of injury. Figure 27a shows the position of the fracture fragments prior to percutaneous medial and lateral pin fixation. Following surgery, healing was uneventful and the patient regained a full painless range of motion. Fifteen months after the injury, she now reports loss of elbow motion and moderate pain with activity. A current AP radiograph is shown in Figure 27b. What is the most likely cause of her symptoms?
Explanation
Explanation
27b The patient sustained a very distal supracondylar fracture of the humerus. Fractures in this area can disrupt the blood vessels supplying the lateral ossification center of the trochlea. With disturbance of the blood supply in this area, local osteonecrosis occurs and disrupts the support for the overlying articular surface, producing joint incongruity and localized degenerative arthritis. Haraldsson S: The interosseous vasculature of the distal end of the humerus with special reference to the capitellum. Acta Orthop Scand 1957;27:81-93.
References:
- Morrissy RT, Wilkins KE: Deformities following distal humeral fracture in childhood. J Bone Joint Surg Am 1984;66:557-562.
Question 5High Yield
Which of the following procedures is included in third-generation cement technique?
Explanation
Explanation
The so-called third-generation cement technique adds porosity reduction techniques, centralization devices, and surface modifications to the femoral component. The surgeon must be aware of the meaning of the various generations of cement technique when interpreting the results presented at meetings and in the literature. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 181-193.
References:
- Maloney WJ, Hartford JM: The cemented femoral component, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, vol 2, pp 959-979.
Question 6High Yield
Figures 3a through 3c show the radiographs and bone scan of a patient who reports increasing pain associated with activity for the past several months. Laboratory studies show an erythrocyte sedimentation rate of 14 mm/h and a C-reactive protein level of 0.4. Aspiration is negative for infection. Management should consist of
Explanation
Explanation
3b 3c The radiographs show polyethylene wear, but exchange of this will not necessarily provide pain relief. The presence of pain suggests the possibility of occult loosening, and the surgeon must be prepared for this option intraoperatively. There is little evidence of infection. Rand JA, Peterson LF, Bryan RS, Ilstrup DM: Revision total knee arthroplasty, in Anderson LD (ed): Instructional Course Lectures XXXV. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1986, pp 305-318.
References:
- Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 317-322.
Question 7High Yield
A 26-year-old man has had hand pain and progressive swelling in the knuckle for the past several months. He denies any trauma to the hand. The ring finger metacarpophalangeal joint is tender, and there is loss of motion in the digit. Figure 32a shows the radiograph and Figures 32b through 32d show the T1-weighted, T2-weighted, and gadolinium MRI scans, respectively. What is the most likely diagnosis?
Explanation
Explanation
32b 32c 32d The radiograph reveals a subchondral lesion in the metacarpophalangeal joint that is lytic and expansile. The MRI scans show a mass that is moderate in intensity on the T2-weighted image and has some gadolinium uptake. There are no cystic components in this lesion. The subchondral location and expansile nature are highly suggestive of giant cell tumor of bone. A lesion with this appearance might also represent an aneurysmal bone cyst, given the amount of expansion present. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 113-118.
References:
- Parsons TW: Benign bone tumors, in Fitzgerald R Jr, Kaufer H, Malkani A (eds): Orthopaedics. Philadelphia, PA, Mosby International, 2002, pp 1027-1035.
Question 8High Yield
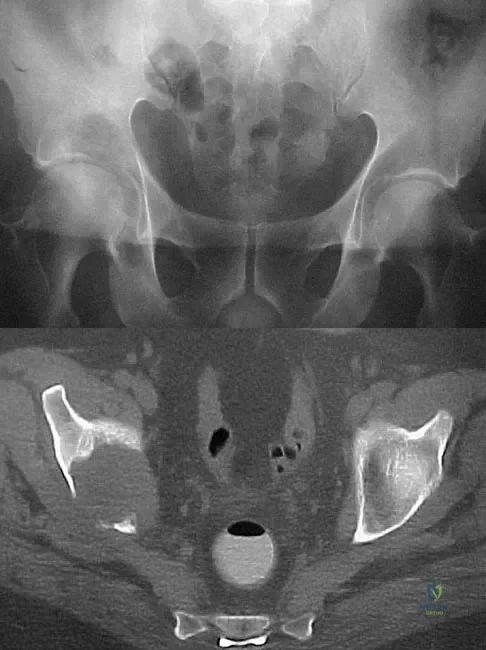
Where is the underlying defect in a rhizomelic dwarf with the findings shown in Figure 5?

Explanation
The radiograph shows the typical findings of achondroplasia. The defect is in fibroblast growth factor receptor 3. The pedicles narrow distally in the lumbar spine. The pelvis is low and broad with narrow sciatic notches and ping-pong paddle-shaped iliac wings. This is often called a champagne glass pelvis. Type I collagen abnormalities are typically found in osteogenesis imperfecta, and type II collagen defects are found in spondyloepiphyseal dysplasia and Kneist syndrome. COMP is defective in multiple epiphyseal dysplasia. Sulfate transport defects are seen in diastrophic dysplasia. Johnson TR, Steinbach LS: Essentials of Musculoskeletal Imaging. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 809-812.
Question 9High Yield
In displaced calcaneal fractures, what fragment is the only one that remains in its anatomic position?
Explanation
The sustentaculum tali remains in its anatomic position because of its supporting ligamentous structures. This provides the key to the reconstruction of the calcaneus. The posterior facet is reduced to the sustentaculum tali and then fixed to it for stability. All of the other components of the calcaneus are then reduced to this complex. Sanders R: Displaced intra-articular fractures of the calcaneus. J Bone Joint Surg Am 2000;82:225-250. Eastwood DM, Gregg PJ, Atkins RM: Intra-articular fractures of the calcaneum: Part I. Pathological anatomy and classification. J Bone Joint Surg Br 1993;75:183-188.
Question 10High Yield
What malignant disease most commonly develops in conjunction with chronic osteomyelitis?
Explanation
Explanation
The most common malignant disease to arise in conjunction with chronic osteomyelitis is squamous cell carcinoma particularly in patients with a long-standing draining sinus tract. Dell PC: Hand, in Simon MA, Springfield D (eds): Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, pp 405-420.
References:
- McGrory JE, Pritchard DJ, Unni KK, Ilstrup D, Rowland CM: Malignant lesion arising in chronic osteomyelitis. Clin Orthop 1998;362:181-189.
Question 11High Yield
A 14-year-old boy who is right handed reports right shoulder pain. Radiographs show a lucent lesion of the proximal humeral epiphysis with a narrow zone of transition. Results of an open biopsy confirm the presence of a chondroblastoma. Based on these findings, the next most appropriate step in management should consist of
Explanation
Explanation
The patient has a chondroblastoma of the proximal humerus; therefore, the treatment of choice is curettage and bone grafting. Surgical resection of the proximal humerus is not indicated in the initial treatment of an intraosseous chondroblastoma. Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, pp 589-623.
References:
- Springfield DS, Capanna R, Gherlinzoni F, Picci P, Campanacci M: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748-755.
Question 12High Yield
A 34-year-old man underwent a transtibial amputation as the result of a work-related injury. The amputation was performed at the inferior level of the tibial tubercle. The residual limb has a soft-tissue envelope composed of gastrocnemius muscle that is used as soft-tissue cushioning for the distal tibia. Despite undergoing several prosthetic fittings, he continues to report pain and instability. Examination reveals that the prosthesis appears to fit well with no apparent pressure points or areas of skin breakdown. He is not willing to have any further surgery. Which of the following modifications will most likely provide relief?
Explanation
While transtibial amputees can be fitted with a prosthesis with a residual limb as short as 5 cm, or with retention of the insertion of the patellar tendon, this patient has an unstable gait because of the limited ability of the prosthetic socket to maintain a snug and stable fit. While cumbersome and bulky, double metal uprights and a corset is the only predictable method of gaining stability. The other methods attempt to add an element of stability; however, they are unlikely to be successful. Bowker JH, Goldberg B, Poonekar PD: Transtibial amputation: Surgical procedures and postsurgical management, in Bowker JH, Michael JW (eds): Atlas of Limb Prosthetics. St Louis, MO, Mosby Year Book, 1992, pp 429-452.
Question 13High Yield
The relocation test is most reliable for diagnosing anterior subluxation of the glenohumeral joint when

Explanation
The relocation test is most accurate when true apprehension is produced with the arm in combined abduction and external rotation and then relieved when posterior pressure is placed on the humeral head. Pain with this test is a less specific response and may occur with other shoulder disorders such as impingement.
Question 14High Yield
The carpal tunnel canal is narrowest (smallest cross-sectional area) at what level?
Explanation
Explanation
The carpal tunnel canal has an hourglass shape in the coronal plane and is narrowest at the level of the hook of the hamate. Cobb TK, Dalley BK, Posteraro RH, et al: Anatomy of the flexor retinaculum. J Hand Surg Am 1993;18:91-99.
References:
- Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow and Shoulder. Rosemont, IL, American Society of Surgery of the Hand, 2003, p 300.
Question 15High Yield
A 30-year-old man has chronic pain, joint stiffness, and symmetrical polyarthropathy but no significant synovitis. Examination reveals enlargement of the second and third metatarsal heads. Radiographs show chondrocalcinosis of the ankles and bony enlargement of the midfoot; no marginal erosions are evident at the metatarsophalangeal level. What is the most likely diagnosis?
Explanation
Explanation
The patient's clinical picture is considered the classic presentation for hemochromatosis. Osteoarthritis and pseudogout more commonly affect an older age group. Rheumatoid arthritis is more common in women and is not commonly associated with chondrocalcinosis. The radiographic appearance of the forefoot in Reiter's syndrome is one of a pencil in cup deformity of the metatarsophalangeal joint, not enlargement. Stevens FM, Edwards C: Recognizing and managing hemochromatosis and hemochromatosis arthropathy. J Musculoskeletal Med 2004;4:212-225.
References:
- Baker ND, Jahss MH, Levanthal GH: Unusual involvement of the feet in hemochromatosis. Foot Ankle 1984;4:212-215.
Question 16High Yield
Figure 63 shows the radiographs of a 23-year-old man who sustained a twisting injury at work. Swelling, tenderness, and ecchymosis are noted about the entire midfoot. What associated injury is most likely to be problematic?

Explanation
This cuboid compression fracture ("nutcracker" injury) is associated with subtle injury to the Lisfranc complex. This diagnosis must be made to ensure proper treatment.
Question 17High Yield
Figure 43 shows the lateral radiograph of a patient who underwent anterior cruciate ligament reconstruction. Based on the tunnel placement shown in the radiograph, evaluation of postoperative knee range of motion will most likely show

Explanation
The radiograph shows the correct tibial tunnel and anterior femoral tunnel; therefore, range of motion will most likely show loss of flexion. Brown CH Jr, Carson EW: Revision anterior cruciate ligament surgery. Clin Sports Med 1999;18:109-171.
Question 18High Yield
A patient reports hyperesthesia over the base of the thenar eminence following volar locked plating of a distal radius fracture. A standard volar approach of Henry was used. What is the most likely cause of the hyperesthesia?

Explanation
The palmar cutaneous branch of the median nerve separates from the median nerve approximately 4 to 6 cm proximal to the wrist crease and travels between the median nerve and the flexor carpi radialis tendon. It supplies the skin of the thenar region. This nerve is at risk for injury with retraction of the digital flexor tendons in plating the distal radius. Wartenberg's syndrome is compression of the superficial radial nerve which innervates the dorsum of the thumb and the first dorsal web space. Carpal tunnel syndrome causes dysesthesias of the thumb, index, and/or middle fingers. C7 radiculopathy affects the index and middle fingers. Jupiter JB, Fernandez DL, Toh CL, et al: Operative treatment of volar intra-articular fractures of the distal end of the radius. J Bone Joint Surg Am 1996;78:1817-1828.
Question 19High Yield
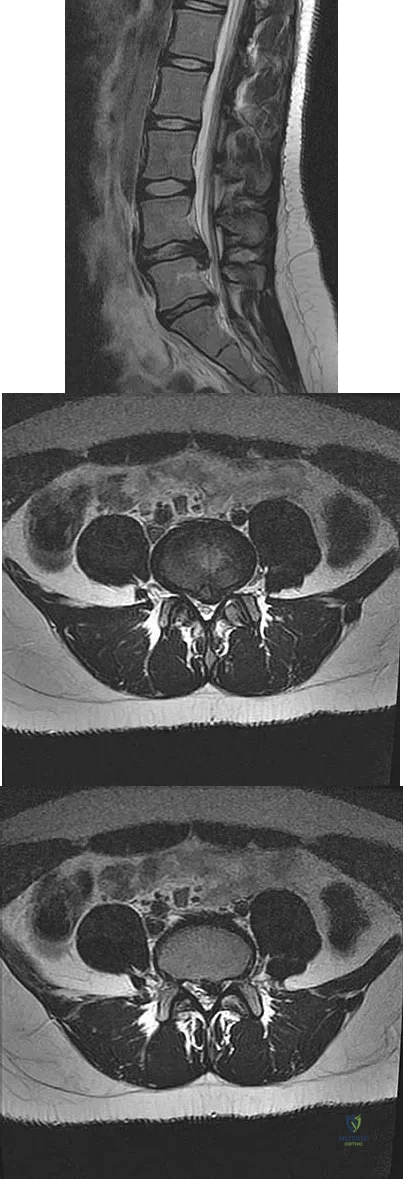
Which of the following findings is the best radiographic indicator of segmental instability at L4-L5?
Explanation
Explanation
Motion segments that demonstrate more than 4 mm of translation or 10 degrees of angulation compared with adjacent motion segments on flexion-extension radiographs have excessive motion and instability. Anterior marginal osteophytes form at the insertion of the annulus from increased forces but do not indicate increased motion. A spondylolisthesis or lateral listhesis is often static without increased motion. More than 3.5 mm of translation or 11 degrees of angulation is considered instability criteria for the cervical spine. Internal disk disruption does not denote instability. Boden SD, Wiesel SW: Lumbosacral segmental motion in normal individuals. Have we been measuring instability properly? Spine 1990;15:571-576.
References:
- Garfin SR, Rauschning W: Spinal stenosis. Instr Course Lect 2001;50:145-152.
Question 20High Yield
A 15-year-old diver has had persistent, activity-related low back pain for the past 2 months. He denies any history of trauma. Examination reveals that the pain is localized to the lumbosacral junction, and there are no radicular symptoms. The pain is worse with back extension. Neurologic examination is normal, as are AP, lateral, and oblique radiographs of the lumbosacral spine. Further evaluation should include
Explanation
Explanation
Spondylolysis may develop as a stress fracture resulting from repetitive hyperextension during athletic activities. In young people, the pars interarticularis is thin, the neural arch has not yet reached maximum strength, and the intravertebral disk is less resistant to shear. While clinical symptoms may lead to the suspicion of spondylolysis, radiographic confirmation may be difficult in early cases. Plain radiographs may be negative initially, and the plain MRI scan may not offer good visualization of the pars. A bone scan with SPECT is very sensitive initially. CT scans with regular axial and reverse-gantry angled cuts may help determine the type of fracture and the course of treatment. Congeni J, McCulloch J, Swanson K: Lumbar spondylolysis: A study of natural progression in athletes. Am J Sports Med 1997;25:248-253.
References:
- Harvey CJ, Richenberg JL, Saifuddin A, Wolman RL: The radiological investigation of lumbar spondylolysis. Clin Radiol 1998;53:723-728.
Question 21High Yield
Which is the best initial study for the diagnostic evaluation of diskogenic low back pain?
Explanation
Explanation
Radiography is the best initial study for the evaluation of diskogenic low back pain. The normal degenerative process can be evaluated. Vacuum phenomenon may be found within the disk space. Other possible sources for back pain should also be evaluated. The other tests may be beneficial but represent later imaging options.
Question 22High Yield
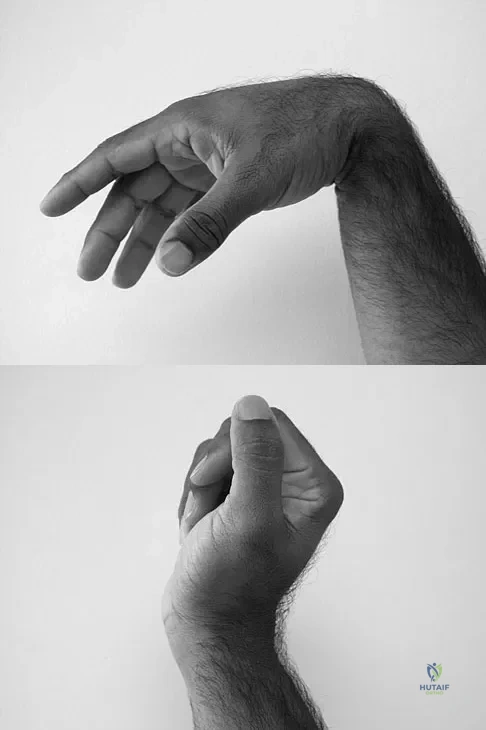
A 35-year-old man sustained a 1-inch stab incision in his proximal forearm while trying to use a screwdriver 2 weeks ago. The laceration was routinely closed, and no problems about the incision site were noted. He now reports that he has been unable to straighten his fingers or thumb completely since the injury. Clinical photographs shown in Figures 30a and 30b show the man passively flexing the wrist. What is the most appropriate management?
Explanation
The clinical photographs indicate that the tenodesis effect of digit flexion with passive wrist extension and digit extension with passive wrist flexion is intact, indicating no discontinuity of the extensor or flexor tendons. The most likely injury is a laceration of the posterior interosseous nerve.
Question 23High Yield
Which of the following findings is seen in the chest radiograph shown in Figure 13?
Explanation
Explanation
Orthopaedic surgeons are often responsible for interpreting radiographs of general examinations such as the chest radiograph shown. For accurate interpretation, it is important to systematically review all of the information available on the radiograph. Using this approach, the fracture of the left proximal humerus is readily recognized. Linear air soft-tissue density at the lung periphery would suggest a pneumothorax, but this finding is not shown on the radiograph. The upper thoracic spine is well aligned. The sternoclavicular and distal clavicles are normal.
References:
- Bone LB: Emergency treatment of the injured patient, in Browner BD, Jupiter JB, Levine AM, Trafton PG (eds): Skeletal Trauma. Philadelphia, PA, WB Saunders, 1992, pp 133-138.
Question 24High Yield
Which of the following factors is a significant predictor of reoperation following open reduction and internal fixation of intertrochanteric fractures with a sliding-compression hip-screw device?
Explanation
Explanation
As shown by Palm and associates from the Hip Fracture Study group, the integrity of the lateral femoral cortex in intertrochanteric hip fractures is a significant predictor of reoperation. Baumgartner and associates have shown that a tip-apex distance of greater than 25 mm is associated with a high risk of femoral head cut-out. Lastly, intertrochanteric hip fractures can be described as standard obliquity or reverse obliquity when describing the fracture pattern. Mechanistically, a reverse obliquity pattern is important to recognize because it reflects the presence or absence of a lateral buttress to which the proximal fracture fragment may compress. Palm H, Jacobsen S, Sonne-Holm S, et al: Integrity of the lateral femoral wall in intertrochanteric hip fractures: An important predictor of a reoperation. J Bone Joint Surg Am 2007;89:470-475. Sadowski C, Lübbeke A, Saudan M, et al: Treatment of reverse oblique and transverse intertrochanteric fractures with use of an intramedullary nail or a 95 degrees screw-plate: A prospective, randomized study. J Bone Joint Surg Am 2002;84:372-381.
Question 25High Yield
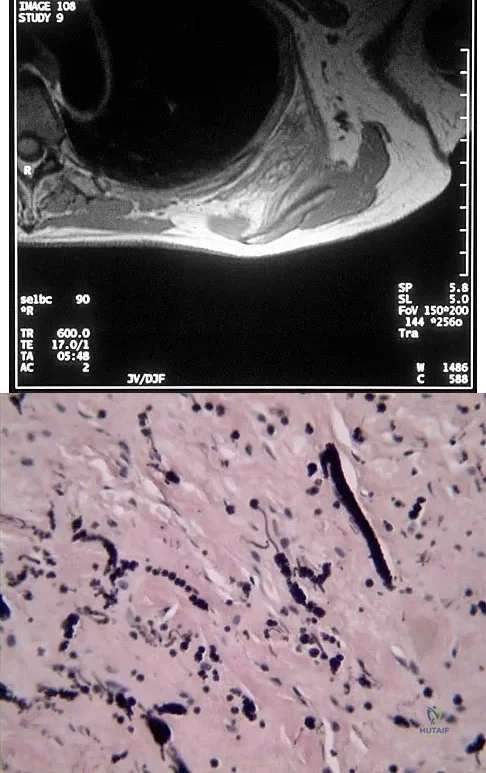
A 58-year-old woman has had a painless periscapular mass for the past year. An MRI scan and biopsy specimen are shown in Figures 4a and 4b. What is the most likely diagnosis?
Explanation
Elastofibroma is a rare tumor that most commonly occurs in adults who are older than age 55 years. The lesions usually grow between the chest wall and the scapula, and 10% are bilateral. Histologic analysis shows that they are composed of equal amounts of elastin and collagen with occasional fibroblasts. Briccoli A, Casadei R, Di Renzo M, Favale L, Bacchini P, Bertoni F: Elastofibroma dorsi. Surg Today 2000;30:147-152.
Question 26High Yield
An 18-year-old football player has intense pain and is unable to bear weight on the right knee after being tackled from the front. A posterior knee dislocation is reduced on the field. Because the game took place in a remote location, the patient is not examined in the emergency department until 5 hours after the injury. Examination now shows a grossly swollen knee with moderate ischemia in the lower leg. Posterior tibial and dorsalis pedis pulses are diminished. The best course of action should be to
Explanation
Explanation
Vascular injuries occur in approximately 20% to 35% of knee dislocations, of which one third are posterior. Recognition of the vascular injury is essential. Normal pulses or normal capillary refill do not preclude an arterial injury, and arteriography should be considered in all knee dislocations. If the leg is ischemic, the arteriogram should be circumvented and the patient taken directly to the operating room. The risk of muscle fibrosis, contracture, or vascular insufficiency, and the need for amputation increase significantly when ischemia exceeds 6 hours. This patient has ischemia and is considered a vascular emergency. As such, delays for a thorough examination of the ligament, MRI scans, and even an arteriogram are unwarranted. Concurrent ligamentous repair and reconstruction should be deferred until vascular stability has been achieved. Kremchek TE, Welling RE, Kremchek EJ: Traumatic dislocation of the knee. Orthop Rev 1989;18:1051-1057.
References:
- Reckling FW, Peltier LF: Acute knee dislocations and their complications. J Trauma 1969;9:181-191.
Question 27High Yield
A 36-year-old man has a moderate-sized left paracentral L5-S1 disk herniation with compression of the S1 nerve. Examination will most likely reveal sensory changes at what location?
Explanation
Explanation
Because the left paracentral L5-S1 disk herniation is compressing the left S1 nerve root, the patient will have numbness along the lateral border and plantar surface of the foot. Numbness along the anterior thigh stopping at the knee is consistent with an L3 radiculopathy. Sensory changes at the dorsum of the foot and great toe normally signify an L5 distribution; the medial leg signifies an L4 distribution. Perianal numbness involves the S2-S5 nerve roots. Wisneski RJ, Garfin SR, Rothman RH, Lutz GE: Lumbar disk disease, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman and Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, vol 1, pp 629-634.
References:
- Hoppenfeld S: Physical Examination of the Spine and Extremities. Norwalk, CT, Appleton- Century-Crofts, 1976, pp 249-254.
Question 28High Yield
A 24-year-old man who was involved in a high speed motor vehicle accident is transferred for definitive care after having been diagnosed with an acute spinal cord injury from a fracture-dislocation at C6-7. He has a complete C6 neurologic level and it is now approximately 10 hours from his injury. What is the most appropriate pharmacologic treatment at this time?
Explanation
Explanation
The standard practice in the pharmacologic treatment of a spinal cord injury in the United States has been the administration of methylprednisolone with an initial bolus of 30 mg/kg followed by 5.4 mg/kg for 24 hours, in accordance with the findings of the second and third National Acute Spinal Cord Injury Studies (NASCIS). Although the studies have subsequently drawn criticism for their methodology and outcomes, it has been generally accepted that beneficial neurologic outcomes were anticipated in patients who were able to start the protocol within 8 hours of their initial injury. Further improvement was noted in patients receiving the methylprednisolone within 3 hours of their injury and continuing an infusion for 48 hours. In this patient, who is outside the 8-hour treatment window, no studies have supported starting the methylprednisolone protocol at this time. Braken MB, Shepard MJ, Holford TR, et al: Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury: Results of the third National Acute Spinal Cord Injury Randomized Controlled Trial. National Acute Spinal Cord Injury Study. JAMA 1997;277:1597-1604.
Question 29High Yield
A 55-year-old woman with a 15-year history of systemic lupus erythematosus has had left shoulder pain for the past 3 months. She reports that the pain has grown progressively worse over the past few months, and her shoulder function is severely limited. She is presently being treated with azathioprine and has used corticosteroids in the past. AP and axillary radiographs are shown in Figures 19a and 19b, and MRI scans are shown in Figures 19c and 19d. Which of the following forms of management will yield the most predictable pain relief and return of shoulder function?
Explanation
Explanation
19b 19c 19d Prosthetic shoulder arthroplasty has been shown to provide predictable results for treating stage III and stage IV osteonecrosis of the humeral head. The decision to resurface the glenoid (total shoulder arthroplasty versus humeral hemiarthroplasty) usually is made based on the radiographic and intraoperative appearance of the glenoid. Core decompression of the humeral head has been reported to be effective for earlier stages (pre collapse) but would not be appropriate for a patient with stage IV disease. Hattrup SJ, Cofield RH: Osteonecrosis of the humeral head: Results of replacement. J Shoulder Elbow Surg 2000;9:177-182. L'Insalata JC, Pagnani MJ, Warren RF, et al: Humeral head osteonecrosis: Clinical course and radiographic predictors of outcome. J Shoulder Elbow Surg 1996;5:355-361.
References:
- Cruess RL: Steroid-induced avascular necrosis of the head of the humerus: Natural history and management. J Bone Joint Surg Br 1976;58:313-317.
Question 30High Yield
A 30-year-old patient has had severe left hip pain and difficulty ambulating, necessitating the use of a cane, for the past 6 months. A photomicrograph of the femoral head sectioned at the time of surgery is shown in Figure 31. What is the most likely diagnosis?
Explanation
The photomicrograph demonstrates a wedge-shaped infarct with femoral head collapse; therefore, the diagnosis is osteonecrosis of the femoral head. Perthes disease and osteoarthritis do not involve a wedge-shaped defect. Tuberculosis of the hip joint results in greater destruction of the articular cartilage. Basset LW, Mirra JM, Cracchiolo A III: Ischemic necrosis of the femoral head: Correlation between magnetic resonance imaging and histologic sections. Clin Orthop 1987;223:181-187.
Question 31High Yield
A 28-year-old man sustained numerous injuries in an accident including a dislocation of the elbow and a severe closed head injury that resulted in unconsciousness. The elbow was reduced in the emergency department. After 1 month of rehabilitation, the patient reports pain and stiffness. A radiograph is shown in Figure 23. Management should now consist of
Explanation
Explanation
In a young individual with a chronic dislocation of the elbow and heterotopic bone formation, the treatment of choice is open reduction, heterotopic bone excision, anterior and posterior capsular releases, and a dynamic hinged fixator to begin protected early postoperative range of motion. It is important to understand that the fixator protects the reconstruction and allows early range of motion, but it does not maintain the reduction and should not be expected to do so. Pin fixation across the elbow delays early motion and is not recommended. Total elbow arthroplasty is not indicated, and ulnohumeral arthroplasty is for a primary arthritic condition. Garland DE, Hanscom DA, Keenan MA, et al: Resection of heterotopic ossification in the adult with head trauma. J Bone Joint Surg Am 1985;67:1261-1269.
References:
- Moor TJ: Functional outcome following surgical excision of heterotopic ossification in patients with traumatic brain injury. J Orthop Trauma 1993;7:11-14.
Question 32High Yield
Figures 38a and 38b show the CT scans of a 64-year-old woman. What is the most likely diagnosis?
Explanation
Explanation
38b The CT scans show large cystic lesions in the talus and calcaneus with complete subluxation of the subtalar joint, allowing the calcaneus to slide laterally until it becomes blocked by the fibula. The cause of this subluxation is severe posterior tibial tendon dysfunction. Although no fibular fracture has yet appeared, it can occur with continued stress from the calcaneus. There is, however, a pathologic fracture in the medial calcaneus through a medial degenerative cyst. The joint space is irregular and not symmetrical as would be seen in an inflammatory arthropathy. Cystic lesions are not present in the tibia. No stress fracture is seen in the talus. Coughlin MJ: Sesamoids and accessory bones of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 437-499.
References:
- Anderson RB, Davis WH: Management of the adult flatfoot deformity, in Myerson M (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1017-1039.
Question 33High Yield
A 15-year-old girl who swims the breaststroke has had hip pain after training excessively for a national level competition. Based on the MRI scans shown in Figures 5a through 5c, what is the most likely diagnosis?
Explanation
Explanation
5b 5c The MRI scans reveal open physes but no evidence of a slipped capital femoral epiphysis, labral tear, or acetabular dysplasia. The femoral neck does not show evidence of a fracture. The muscle tear seen on the right side lies near the musculotendinous junction of the external rotators of the hip at the level of the lesser trochanter, representing the obturator externus. This is consistent with the forced motion required for the breaststroke kick. Grote K, Lincoln TL, Gamble JG: Hip adductor injury in competitive swimmers. Am J Sports Med 2004;32:104-108.
References:
- Clemente C: Anatomy: A Regional Atlas of the Human Body, ed 3. Baltimore-Munich, Urban and Schwarzenberg, 1987, Figures 429, 430.
Question 34High Yield
Examination of a 25-year-old man who was injured in a motor vehicle accident reveals a fracture-dislocation of C5-6 with a Frankel B spinal cord injury. He also has a closed right femoral shaft fracture and a grade II open ipsilateral midshaft tibial fracture. Assessment of his vital signs reveals a pulse rate of 45/min, a blood pressure of 80/45 mm Hg, and respirations of 25/min. A general surgeon has assessed the abdomen, and a peritoneal lavage is negative. His clinical presentation is most consistent with what type of shock?

Explanation
Assessment of the acutely injured patient follows the Advanced Trauma Life Support protocol. Cervical cord injury is often associated with a disruption in sympathetic outflow. Absent sympathetic input to the lower extremities leads to vasodilatation, decreased venous return to the heart, and subsequent hypotension. With hypotension, the physiologic response of tachycardia is not possible because of the unopposed vagal tone. This results in bradycardia. Patient positioning, fluid support, pressor agents, and atropine are used to treat neurogenic shock.
Question 35High Yield
A 62-year-old man who underwent total knee arthroplasty 6 months ago now reports pain after falling on the anterior portion of the knee. Examination reveals weakness of knee extension but no extensor lag. Flexion that had once measured 115 degrees is now limited to 70 degrees because of pain. A radiograph is shown in Figure 25. Management should now consist of

Explanation
The patient has a type IIIB patellar fracture (inferior pole fracture with an intact patellar tendon). Nonsurgical management is the treatment of choice if there is little displacement and the extensor mechanism is intact. Brown TE, Diduch DR: Fractures of the patella, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 3. Philadelphia, PA, Churchill Livingstone, 2001, vol 2, pp 1290-1312.
Question 36High Yield
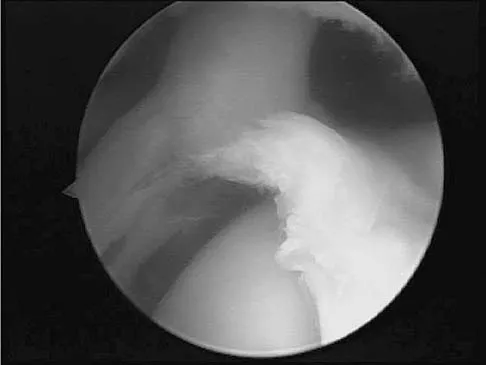
A baseball pitcher has intractable posterior and superior shoulder pain. The arthroscopic view seen in Figure 25 shows no Bankart or Hill-Sachs lesion and a negative drive-through sign. There are no signs of ligamentous laxity, but active compression and anterior slide tests are positive. Treatment should consist of
Explanation
According to Morgan and associates, a type II SLAP lesion can create or is associated with a superior instability pattern. They suggest that this can exist without a co-existing anteroinferior instability pattern. They reported that repair of the SLAP lesion alone resulted in satisfactory outcomes in 90% of patients and a return to throwing in more than 90% of pitchers. The arthroscopic findings in this patient do not support a diagnosis of anteroinferior laxity or instability; therefore, thermal capsular shift or capsular placation is not necessary. Morgan CD, Burkhart SS, Palmeri M, et al: Type II SLAP lesions: Three subtypes and their relationships to superior instability and rotator cuff tears. Arthroscopy 1998;14:553-565. Mileski RA, Snyder RJ: Superior labral lesions in the shoulder: Pathoanatomy and surgical management. J Am Acad Orthop Surg 1998;6:121-131.
Question 37High Yield
A 220-lb 20-year-old man was involved in a motor vehicle accident. His work-up reveals that he has multiple long bone fractures as well as a splenic injury that is currently being managed nonsurgically. His initial blood pressure in the trauma bay was 70/30 mm Hg. After receiving 4 liters of fluid and 3 units of packed red blood cells, his blood pressure is currently 110/70, his heart rate is 100, his urine output is 90 mL/h (normal 0.5 to 1 mL/kg/h), and his core temperature is 97.9 degrees F (36.5 degrees C). At this point, the patient's resuscitation can be described as which of the following?
Explanation
Explanation
Although the end points of resuscitation are still unclear, what is known is that normalization of the standard hemodynamic parameters (blood pressure, heart rate, and urine output) is not adequate. Up to 85% of patients with normal hemodynamic parameters can still have inadequate tissue oxygenation or uncompensated shock. The initial base deficit, lactate level, or gastric pHi can be used to stratify patients for resuscitation needs, risks of death, and multiple organ failure (level 1 evidence). The time it takes to normalize the base deficit, the lactate level, or gastric pHi, can predict survival (level 2 evidence). Patients who have been in uncompensated shock (abnormal vital signs) should have their resuscitation monitored using data other than vital signs. Tisherman SA, Barie P, Bokhari F, et al: Clinical practice guideline: Endpoints of resuscitation. J Trauma 2004;57:898-912. Moore FA, McKinley BA, Moore EE, et al: Inflammation and the Host Response to Injury, a large-scale collaborative project: Patient-oriented research core--standard operating procedures for clinical care. III. Guidelines for shock resuscitation. J Trauma 2006;61:82-89.
Question 38High Yield
Figure 13 shows the MRI scan of a 29-year-old rock climber who reports increasing shoulder pain and weakness. Based on these findings, atrophy will most likely occur in which of the following muscles?
Explanation
Explanation
The MRI scan shows a cyst at the spinoglenoid notch. These cysts are often associated with a labral injury, such as a superior labrum anterior and posterior (SLAP) lesion. The suprascapular nerve passes through the suprascapular notch and sends motor branches to the supraspinatus and sensory branches to the capsule. At the spinoglenoid notch, the infraspinatus branch of the suprascapular nerve is compressed by the cyst, leading to isolated infraspinatus atrophy. The teres minor and the deltoid are innervated by the axillary nerve. Fehrman DA, Orwin JF, Jennings RM: Suprascapular nerve entrapment by ganglion cysts: A report of six cases with arthroscopic findings and review of the literature. Arthroscopy 1995;11:727-734. Ianotti JP, Ramsey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
References:
- Tirman PF, Feller JF, Janzen DL, Peterfy CG, Bergman AG: Association of glenoid labral cysts and labral tears in glenohumeral instability: Radiologic findings and clinical significance. Radiology 1994;190:653-658.
Question 39High Yield
The vascular supply to the medial meniscus comes primarily from what artery?
Explanation
Explanation
The vascular supply to the medial and lateral menisci originates predominantly from the medial and lateral genicular arteries. The popliteal artery splits into the superior genicular, which splits into medial and lateral branches supplying the patellar cartilage and the posterior cruciate ligament. The middle genicular artery also supplies the anterior curciate ligament, posterior cruciate ligament, and collateral ligaments. The inferior genicular splits into medial and lateral branches and supplies the menisci and other knee ligaments. Despite propagation of incorrect terminology, there is no superior or lateral genicular artery.
References:
- Mow VC, Arnoczky SP, Jackson DW (eds): Knee Meniscus: Basic and Clinical Foundations. New York, NY, Raven Press, 1992, p 4.
Question 40High Yield
Figure 12 shows the lumbar CT scan of a 24-year-old man who was injured in a snowmobile accident. What is the mechanism of injury?

Explanation
A true compression fracture is a single-column injury that does not create canal compromise. A burst fracture is a two- or three-column injury that disrupts the middle column and thereby narrows the spinal canal. This patient has a burst fracture. The mechanism of injury is usually vertical compression or flexion compression. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-217.
Question 41High Yield
Which of the following is a long-term complication of ankle arthrodesis for posttraumatic arthritis?
Explanation
Ankle arthrodesis for posttraumatic ankle arthrosis provides reliable pain relief. However, the long-term sequela of joint arthrodesis is the development of arthrosis in the surrounding joints. Over time, following ankle arthrodesis, the ipsilateral hindfoot and midfoot joints show signs of joint space wear, and this may be symptomatic. With a stable ankle arthrodesis, progressive limb-length discrepancy or talar osteonecrosis is not expected. Ankle arthrodesis has not been definitively linked to ipsilateral knee arthritis or contralateral ankle arthritis. Coester LM, Saltzman CL, Leupold J, Pontarelli W: Long-term results following ankle arthrodesis for post-traumatic arthritis. J Bone Joint Surg Am 2001;83:219-228.
Question 42High Yield
What is the most common presenting sign or symptom in an adult with lumbar pyogenic infection?
Explanation
Explanation
Pain is very common but is often nonspecific; therefore, the diagnosis of spinal infection is often delayed. Fever and sepsis can occur but are not common. Neurologic manifestations also can occur but are absent in most patients. In findings reported by Carragee, the urinary tract is a common source for hematogenous spinal infection, but the source was found in only 27% of 111 patients. Direct inoculation during spinal surgery is uncommon. Carragee EJ: Pyogenic vertebral osteomyelitis. J Bone Joint Surg Am 1997;79:874-880. Frazier DD, Campbell DR, Garvey TA, et al: Fungal infections of the spine: Report of eleven patients with long-term follow-up. J Bone Joint Surg Am 2001;83:560-565.
References:
- Hadjipavlou AG, Mader JT, Necessary JT, et al: Hematogenous pyogenic spinal infections and their surgical management. Spine 2000;25:1668-1679.
Question 43High Yield
A 30-year-old patient reports chronic medial knee pain and swelling. Figure 9a shows an articular cartilage lesion observed during arthroscopy. The surgeon decides to treat the lesion with the microfracture technique seen in Figure 9b. A biopsy of the repaired tissue 1 year after treatment is likely to show which of the following findings?
Explanation
Explanation
9b Microfracture is a marrow stimulation technique where stem cells from the underlying subchondral bone marrow can form at the base of the lesion. The rationale for this technique is based on these cells differentiating into cells that will produce an articular cartilage repair. Biopsy findings in animals and humans have demonstrated primarily a fibrocartilagenous repair tissue and not articular cartilage. The collagen type found in hyaline or articular cartilage is of the type II variety. Fibrocartilage possesses mostly type I and III cartilage. Buckwalter JA, Mankin HJ: Articular cartilage: Degeneration and osteoarthritis, repair, regeneration, and transplantation. Instr Course Lect 1998;47:487-504.
References:
- Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 471-488.
Question 44High Yield
Which of the following malignant tumors most commonly contains soft-tissue calcifications seen on radiographs or CT?

Explanation
Focal calcifications causing small radiopacities are found in 15% to 20% of synovial sarcomas. Their irregular contours differentiate them from the phleboliths found in a benign hemangioma. Ewing's sarcoma, clear cell sarcoma, and malignant fibrous histiocytoma do not commonly have calcifications within the lesions. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 761.
Question 45High Yield
The parents of a 10-year-old boy with Down syndrome are seeking sports clearance for participation in the high jump at the Special Olympics. He is asymptomatic, and the neurologic examination is normal. The hips and patellae are clinically stable. Radiographs of the cervical spine in flexion and extension show a maximum atlanto-dens interval (ADI) of 6 mm. Based on these findings, what recommendation should be made?
Explanation
Explanation
In approximately 15% of children with Down syndrome, atlantoaxial instability develops because of ligament laxity, making them susceptible to spinal cord injury with relatively minor trauma. The American Academy of Pediatrics recommends lateral flexion-extension views of the cervical spine in any patient with Down syndrome who wishes to participate in sports. A normal ADI is up to 4 mm. Patients with Down syndrome with an ADI of more than 5 mm should not participate in contact sports or sports with a high risk for neck injury, such as diving, gymnastics, high jump, or butterfly stroke. Cervical fusion has a very high rate of complications in patients with Down syndrome and is recommended only for patients who have myelopathic signs or symptoms. Atlantoaxial instability in Down syndrome: Subject review. American Academy of Pediatrics Committee on Sports Medicine and Fitness. Pediatrics 1995;96:151-154. Tredwell SJ, Newman DE, Lockitch G: Instability of the upper cervical spine in Down syndrome. J Pediatr Orthop 1990;10:602-606.
References:
- Segal LS, Drummond DS, Zanotti RM, et al: Complications of posterior arthrodesis of the cervical spine in patients who have Down syndrome. J Bone Joint Surg Am 1991;73:1547-1554.
Question 46High Yield
Stability at the atlanto-occipital joint is provided mainly by
Explanation
The atlanto-occipital joint is inherently unstable and would easily dislocate without the supporting ligaments. The apical ligament attaches to the basion and tip of the dens but does not provide adequate stability to the joint. Werne demonstrated that dividing the tectorial membrane and the alar ligaments resulted in gross joint instability. The anterior longitudinal ligament turns into the anterior atlanto-occipital membrane. This is called a membrane rather than a ligament because it is not strong enough to support these two structures. Werne S: Studies in spontaneous atlas dislocation. Acta Orthopaedica Scandinavica 1977;23(supplement).
Question 47High Yield
Duchenne's muscular dystrophy is a genetic disorder that is transmitted by which of the following modes of inheritance?

Explanation
Patients with Duchenne's muscular dystrophy show progressive muscular weakness because of the absence of dystrophin and have the clinical picture of progressive muscle weakness. The condition is an X-linked genetic disease. Fitzgerald RH, Kaufer H, Malkani AL: Orthopaedics. St Louis, MO, Mosby Year Book, 2002, pp 1573-1583.
Question 48High Yield
Varus deformity after talar fractures is often seen due to collapse of the medial cortex. What artery supplies this portion of the talus?
Explanation
Explanation
The artery of the tarsal canal is a branch of the posterior tibial artery. Among the branches of the artery of the tarsal canal is the deltoid artery. This arterial complex supplies the medial one third of the talar body. Disruption of this artery may lead to osteonecrosis of the medial body and subsequent collapse into varus. This is most commonly seen with talar body fractures but may be seen in Hawkins type 3 talar neck fractures. The artery of the tarsal sinus arises from the dorsalis pedis, lateral malleolar, and perforating peroneal arteries. The peroneal artery anastomoses with the calcaneal branches of the posterior tibial artery to form a plexus of vessels that supplies the posterior tubercle of the talus. Disruption of this artery would not result in collapse of the medial body, and thus would not lead to a varus deformity. Halibruton RA, Sullivan CR, Kelly PJ, et al: The extra-osseous and intra-osseous blood supply of the talus. J Bone Joint Surg Am 1958;40:1115.
References:
- Mulfinger GL, Trueta J: The blood supply of the talus. J Bone Joint Surg Br 1970;52:160-167.
Question 49High Yield
In a patient who has had low back pain for less than 2 weeks, which of the following findings is an indication for continued observation and symptomatic treatment rather than more aggressive evaluation and/or treatment?
Explanation
An inability to participate in athletics generally is considered an indication for continued symptomatic treatment only. All of the other answers suggest the possibility of more significant pathology that may require more urgent treatment. Frymoyer JW: Back pain and sciatica. N Engl J Med 1988;318:291-300.
Question 50High Yield
A 28-year-old man who sustained an ankle fracture in a motor vehicle accident underwent open reduction and internal fixation 3 months ago. He continues to report significant ankle pain with ambulation. Radiographs are shown in Figure 26. What is the next most appropriate step in management?

Explanation
The patient sustained a bimalleolar ankle fracture with a syndesmosis disruption. The initial open reduction and internal fixation did not successfully reduce the distal tibiofibular joint. The patient may need a derotational distraction osteotomy of the fibula to reduce the syndesmosis. The other procedures do not address the primary problem of the fibular malunion and syndesmosis malreduction. There is no radiographic evidence of significant arthritis; therefore, ankle arthrodesis is not indicated.
Question 51High Yield
Which of the following findings is an indication for adjunctive use of high-dose steroids?
Explanation
Explanation
According to NASCIS III, the high-dose steroid protocol involves infusion of 30 mg/kg methylprednisolone followed by 5.4 mg/kg/h for 24 hours if the patient has sustained a spinal cord injury within the last 3 hours. The drip is continued for 48 hours if administration is started between 3 and 8 hours of the onset of neurologic deficit. No benefit has been conclusively demonstrated with steroids administered beginning 8 hours or longer after injury. Steroid use is not indicated for nerve root deficits, brachial plexus deficits, or gunshot wounds. Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 319-328.
References:
- Bracken MB, Shepard MJ, Holford TR, et al: Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury: Results of the Third National Acute Spinal Cord Injury randomized controlled trial. National Acute Spinal Cord Injury Study. JAMA 1997;277:1597-1604.
Question 52High Yield
Figures 20a and 20b show the radiographs of an obese 15-year-old boy who has severe left groin pain and is unable to bear weight following a minor injury. Treatment should consist of
Explanation
Explanation
20b The radiographs and history are consistent with an acute unstable slipped capital femoral epiphysis. Aronson and Loder documented an increased rate of osteonecrosis associated with manipulative reduction. They recommended bed rest with skin traction to allow the synovitis to resolve, followed by in situ pinning. They noted, however, that many of these slips reduced with anesthesia and positioning on a fracture table. Biomechanic studies have shown a slight increased resistance to shear stress when two screws are used, but it is unknown if this is significant in the clinical setting. Open epiphyseodesis does not provide postoperative stability; therefore, adjunctive fixation or immobilization is required. Numerous studies have noted the inadvisability of using multiple screws. Casting has a high rate of complications, including chondrolysis and progression of the slip. Aronson DD, Loder RT: Treatment of the unstable (acute) slipped capital femoral epiphysis. Clin Orthop 1996;322:99-110. Karol LA, Doane RM, Cornicelli SF, Zak PA, Haut RC, Manoli A II: Single versus double screw fixation for treatment of slipped capital femoral epiphysis: A biomechanical analysis. J Pediatr Orthop 1992;12:741-745.
References:
- Stanitski CL: Acute slipped capital femoral epiphysis: Treatment alternatives. J Am Acad Orthop Surg 1994;2:96-106.
Question 53High Yield
Figure 34 shows the standing AP radiograph of a 2-year-old girl who has a left bowleg deformity. Her mother states that she first noticed the problem when the child began walking at age 10 months, and the deformity has worsened over the past 6 months. Examination reveals a definite lateral thrust of the knee during the stance phase of gait. Management should consist of

Explanation
Infantile tibia vara is a developmental condition characterized by a varus angulation of the proximal end of the tibia that is caused by a growth disturbance of the proximal medial physis. In a study of 42 affected extremities in 24 children younger than age 3 years, it was found that daytime ambulatory brace treatment favorably altered the natural history of tibia vara. Another study of 27 patients with stage II Langenskiöld disease found a success rate of 70% (improved alignment without the need for osteotomy) using brace treatment. These authors also noted that children with unilateral disease were more likely to obtain correction of the deformity compared with those with bilateral disease. In this patient, observation is not warranted because untreated tibia vara has a significant risk for progressive worsening. Osteotomy is best reserved for those patients who, despite bracing, do not show satisfactory clinical and radiographic improvement by age 4 years. Elevation of the medial tibial plateau is a treatment option for older patients who have more advanced disease. An MRI scan would not provide any useful clinical information at this time. Zionts LE, Shean CJ: Brace treatment of early infantile tibia vara. J Pediatr Orthop 1998;18:102-109. Richards BS, Katz DE, Sims JB: Effectiveness of brace treatment in early infantile Blount's disease. J Pediatr Orthop 1998;18:374-380.
Question 54High Yield
Ganglion cysts about the wrist most commonly arise from what structure?
Explanation
Ganglion cysts are the most common mass or mass-like lesions seen in the hand and wrist. They arise in a variety of locations, including synovial joints or tendon sheaths. The most common location is the dorsal/radial wrist arising from the dorsal scapholunate interosseous ligament.
Question 55High Yield
A 25-year-old left hand-dominant man has severe left shoulder pain after being involved in a high-speed motor vehicle accident. Examination reveals that he is unable to move the left shoulder. His neurovascular status is intact in the entire left upper extremity. A radiograph is shown in Figure 19. What is the most appropriate surgical management of this injury?
Explanation
Explanation
In this young patient, every attempt must be made to retain the native proximal humerus; therefore, open reduction and internal fixation should be attempted of both the articular segment and tuberosities to the humeral shaft. This is best accomplished through an open approach. Shoulder arthroplasty should be reserved for the elderly and for failed internal fixation. Ko JY, Yamamoto R: Surgical treatment of complex fractures of the proximal humerus. Clin Orthop Relat Res 1996;327:225-237.
References:
- Aschauer E, Resch H: Four-part proximal humeral fractures: ORIF, in Warner JP, Iannotti JP, Flatow EL (eds): Complex and Revision Problems in Shoulder Surgery, ed 2. Philadelphia, PA, Lippincott Williams & Wilkins, 2005, pp 289-309.
Question 56High Yield
A 20-year-old man involved in a motor vehicle accident is brought to the emergency department with a C6-7 unilateral facet dislocation. His neurologic examination reveals a focal left-sided C7 nerve root palsy. He is awake and cooperative with questioning and has no other obvious traumatic injuries. What is the most appropriate treatment at this time?
Explanation
In the patient who is neurologically intact or has an incomplete injury from a cervical facet dislocation, a closed reduction with weighted tong traction is appropriate when the patient is awake, alert, and cooperative. Although there is a risk that a cervical facet dislocation could occur with an underlying cervical disk herniation, Vaccaro and associates have shown that closed reduction can be safely carried out in the awake, responsive patient. Closed reduction can be performed in the emergency department with traction with skull tongs or a halo ring. A slow stepwise application of weight is added until a reduction is achieved. Any worsening of the neurologic status of the patient requires immediate termination of the closed reduction and further diagnostic imaging before proceeding with further treatment. Vaccaro AR, Falatyn SP, Flanders AE, et al: Magnetic resonance evaluation of the intervertebral disc, spinal ligaments, and spinal cord before and after closed traction reduction of cervical spine dislocations. Spine 1999;24:1210-1217. Hart RA: Cervical facet dislocation: When is magnetic resonance imaging indicated? Spine 2002;27:116-117.
Question 57High Yield
The afferent pain innervation of the L3-L4 facet joint arises from the medial branch nerve of
Explanation
Explanation
Afferent pain fibers to the lumbar facet joints arise from the medial branch nerves originating from the next two cephalad levels. Therefore, innervation of the L3-L4 facet joint arises from the L2 and L3 medial branch nerves. This effect should be taken into account when considering a medial branch block or facet denervation. The medial branch nerve arises from the dorsal ramus of the exiting nerve root. Nade SL, Bell E, Wyke BD: The innervation of the lumbar spinal joint and its significance. J Bone Joint Surg Br 1980;62:255-261
References:
- Kornick C, Kramarich SS, Lamer TJ, et al: Complications of lumbar facet radiofrequency denervation. Spine 2004;29:1352-1354.
Question 58High Yield
Which of the following tendons is the primary antagonist of the posterior tibialis tendon?

Explanation
The primary action of the posterior tibialis tendon is inversion of the foot; secondarily, it plantar flexes the ankle. The anterior tibialis tendon also inverts the foot and only partially antagonizes the posterior tibialis tendon. The primary action of the peroneus longus is plantar flexion of the first ray. It secondarily everts the posterior tibialis tendon. The action of the flexor digitorum longus tendon is synergistic with the posterior tibialis tendon. The primary action of the peroneus brevis tendon is eversion; therefore, it is the primary antagonist of the posterior tibialis tendon. Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 550-551.
Question 59High Yield
Which of the following best describes the most common anatomic variation seen in the glenoid labrum and the middle glenohumeral ligament in the anterosuperior quadrant of the shoulder??
Explanation
Explanation
Wide variations in the anatomy of the anterosuperior portion of the labrum and the middle glenohumeral ligament have been reported and are more common than previously thought. The labrum attached to the glenoid rim and a flat/broad middle glenohumeral ligament is the most common "normal" variation. A cord-like middle glenohumeral ligament is often associated with the presence of a sublabral hole. An anterosuperior labrum confluent with a cord-like middle glenohumeral ligament and no labral attachment to bone is the configuration of the Buford complex. The prevalence of each variation from one recent study is as follows: #1: 86.6%; #2: 3.3%; #3: 8.6%; and #4: 1.5%. Rao AG, Kim TK, Chronopoulos E, et al: Anatomical variants in the anterosuperior aspect of the glenoid labrum. J Bone Joint Surg Am 2003;85:653-659. Ilahi OA, Labbe MR, Cosculluela P: Variants of the anterosuperior glenoid labrum and associated pathology. Arthroscopy 2002;18:882-886.
References:
- Williams MM, Snyder SJ, Buford D: The Buford complex-The "cord-like" middle glenohumeral ligament and absent anterosuprior labrum complex: A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.
Question 60High Yield
A 21-year-old man with neurofibromatosis and multiple cutaneous neurofibromas has a rapidly enlarging painless mass on his buttock. Examination reveals a nontender, well-defined 6- x 6-cm soft-tissue mass that is deep to the fascia. The best course of action should be to order
Explanation
Explanation
Patients with neurofibromatosis are at risk for development of soft-tissue sarcomas (most commonly malignant peripheral nerve sheath tumors). Clinical indications of development of a neurofibrosarcoma include a rapidly enlarging soft-tissue mass; therefore, this patient should be considered to have a neurofibrosarcoma until proven otherwise. MRI is superior to CT in characterizing the anatomic location of soft-tissue masses and the signal characteristics of the lesion. Areas of necrosis within the tumor may be apparent on MRI that cannot be appreciated on CT, suggesting a malignant tumor. Local imaging studies of suspected malignant tumors should be performed prior to needle or open biopsy so that the biopsy site can be excised at the time of definitive resection. Additionally, postbiopsy changes may lead to MRI artifacts that alter the interpretation of the MRI. Demas BE, Heelan RT, Lane J, Marcove R, Hajdu S, Brennan MF: Soft-tissue sarcomas of the extremities: Comparison of MR and CT in determining the extent of disease. Am J Roentgenol 1988;150:615-620.
References:
- Kransdorf MJ, Jelinek JS, Moser RP Jr, et al: Soft-tissue masses: Diagnosis using MR imaging. Am J Roentgenol 1989;153:541-547.
Question 61High Yield
A 17-year-old boy who fell on a pitchfork in a barn 1 day ago now has a painful, swollen forearm. Examination reveals erythema, exquisite tenderness, and crepitus to palpation of the forearm. He has a pulse rate of 110/min and a blood pressure of 80/60 mm Hg. Radiographs show subcutaneous air and no fractures. Gram stain of wound drainage reveals a gram-positive bacillus. The next most appropriate step in management should consist of
Explanation
Explanation
The successful treatment of necrotizing soft-tissue infections such as clostridial myonecrosis depends on prompt recognition and aggressive surgical debridement of all involved muscle, fascia, and soft tissue, resecting to a clearly normal healthy, viable margin. The effective antibiotic regimen for clostridial infection is high-dose penicillin; however, necrotizing infections are frequently polymicrobial so initially broad-spectrum antibiotics are indicated. Hyperbaric oxygen therapy may be used as an adjunct to surgical treatment but is insufficient as a primary therapy. Prolonged application of tourniquets and wound closure should be avoided. Pellegrini VD, Evarts CM: Complications, in Rockwood CA Jr, Green DP (eds): Fractures in Adults, ed 3. Philadelphia, PA, JB Lippincott, 1991, pp 365-370. Gerding DN, Peterson LR: Infections caused by anaerobic bacteria, in Shulman ST, Phair JP, Peterson LR, Warren JR (eds): Infectious Diseases, ed 5. Philadelphia, PA, WB Saunders, 1997, pp 416-417.
References:
- Stephens DC: Myositis and fascitis, in Root RK (ed): Clinical Infectious Diseases, ed 1. Oxford, England, Oxford Press University, 1999, pp 769-770.
Question 62High Yield
Which of the following is most predictive of a medial side ankle injury in the presence of a fibula fracture above the level of the joint?
Explanation
Explanation
Isolated Lauge-Hansen supination-external rotation-type ankle fractures comprise 20% to 40% of ankle fractures and nonsurgical management is effective for managing SER-2 ankle fractures. Tornetta and associates recently showed that medial ankle tenderness, ecchymosis, and swelling are not reliable findings when trying to determine deltoid competence. Stress radiographs showing a medial clear space of greater than 4 mm or one that is also 1 mm greater than the superior joint space, or any lateral talar subluxation are indicative of deltoid incompetence and indicative of a SER-4 ankle fracture. McConnell T, Creevy W, Tornetta P III: Stress examination of supination external rotation-type fibular fractures. J Bone Joint Surg Am 2004:86;2171-2178. Kristensen KD, Hansen T: Closed treatment of ankle fractures: Stage II supination-eversion fractures followed for 20 years. Acta Orthop Scand 1985;56:107-109.
Question 63High Yield
A 29-year-old woman was injured in a high-speed motor vehicle accident 3 hours ago. Radiographs are shown in Figures 7a through 7e. Her right foot injury is open and contaminated. Her associated injuries include a closed head injury and a ruptured spleen requiring resection. She has had 6 units of packed red blood cells and the trauma surgeon has turned her care over to you. Her current base deficit is 10 and her urinary output has averaged 0.4 mL/kg for the last 2 hours. What is the best treatment at this time?
Explanation
Explanation
7b 7c 7d 7e The patient appears to be a borderline or unstable surgical patient following her initial trauma and spleenectomy (high base excess and low urine output). She needs continued resuscitation and minimal additional blood loss. This is best accomplished with irrigation and debridement of the ankle, external fixation of the ankle, foot, and femur, and splinting of the forearm. A traction pin for the femoral fracture will not control bleeding as well as an external fixator. Intramedullary nailing of the femur and open reduction and internal fixation of the forearm would be appropriate in patients that are euvolemic and stable. Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopedic surgery. J Trauma 2002;53:452-461. Taeger G, Ruchholtz S, Waydhas C, et al: Damage control orthopedics in patients with multiple injuries is effective, time saving, and safe. J Trauma 2005;59:409-416. Harwood PJ, Giannoudis PV, van Griensven M, et al: Alterations in the systemic inflammatory response after early total care and damage control procedures for femoral shaft fracture in severely injured patients. J Trauma 2005;58:446-452.
Question 64High Yield
Figure 13 shows the radiographs of a 56-year-old woman who has pain and varus knee deformity after undergoing total knee arthroplasty 8 years ago. Aspiration and studies for infection are negative. During revision surgery, management of the tibial bone loss is best achieved by
Explanation
Explanation
Massive bone loss encountered in revision total knee arthroplasty remains a significant challenge. Recent reports have shown high success rates using structural allograft to reconstruct massive bone defects. Custom and hinged prostheses in this setting are no longer favored. The defect shown is segmental and is too large to be filled with cement or iliac crest bone graft. Mow CS, Wiedel JD: Structural allografting in revision total knee arthroplasty. J Arthroplasty 1996;11:235-241. Engh GA, Herzwurm PJ, Parks NL: Treatment of major defects of bone with bulk allografts and stemmed components during total knee arthroplasty. J Bone Joint Surg Am 1997;79:1030-1039.
References:
- Clatworthy MG, Ballance J, Brick GW, Chandler HP, Gross AE: The use of structural allograft for uncontained defects in revision total knee arthroplasty: A minimum five-year review. J Bone Joint Surg Am 2001;83:404-411.
Question 65High Yield
A coronal MRI scan through the shoulder joint is shown in Figure 26. The cyst indicated by the arrow will most likely cause compression of what nerve?
Explanation
Explanation
The MRI scan shows a ganglion cyst in the region of the spinoglenoid notch. These are difficult to diagnose clinically but are readily apparent on MRI. They usually cause compression of the suprascapular nerve and weakness of the infraspinatus and supraspinatus muscles. Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 306-309.
References:
- Iannotti JP, Ramsey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
Question 66High Yield
During the application of halo skeletal fixation, the most appropriate position for the placement of the anterior halo pins is approximately 1 cm above the superior orbital rim and
Explanation
Explanation
Halo fixation is the most rigid form of cervical orthosis, but complications can arise from improper placement of the initial halo ring. A relatively safe zone for anterior pin placement is located 1 cm above the orbital rim and superior to the lateral two thirds of the orbit. This position avoids the supraorbital and supratrochlear nerves and arteries over the medial one third of the orbit. The more lateral positions in the temporal fossa have very thin bone and can interfere with the muscles of mastication. Posterior pin site locations are less critical; positioning on the posterolateral aspect of the skull, diagonal to the contralateral anterior pins, is generally desirable. Botte MJ, Byrne TP, Abrams RA, et al: Halo skeletal fixation: Techniques of application and prevention of complications. J Am Acad Orthop Surg 1996;4:44-53.
Question 67High Yield
A 50-year-old man with no history of trauma reports new-onset back pain after doing some yard work the previous day. He reports pain radiating down his leg posteriorly and into the first dorsal web space of his foot. MRI scans are shown in Figures 3a through 3c. What nerve root is affected?
Explanation
The MRI scans clearly show an extruded L4-5 disk that is affecting the L5 nerve root on the left side. In addition, the L5 nerve root has a cutaneous distribution in the first dorsal web space. S1 affects the lateral foot. L4 affects the medial calf.
Question 68High Yield
Which of the following structures runs through the site indicated by the arrow in Figure 11?

Explanation
The vertebral artery traverses through the arcuate foramen after exiting the lateral aspect of C1 and before entering the skull. The foramen usually is not fully formed, but a complete foramen such as this one has been reported in up to 18% of patients. Stubbs DM: The arcuate foramen: Variability in distribution related to race and sex. Spine 1992;17:1502-1504.
Question 69High Yield
A 15-year-old girl has left knee pain and an enlarging mass in the distal thigh. AP and lateral radiographs are shown in Figures 52a and 52b, and a biopsy specimen is shown in Figure 52c. What is the most likely diagnosis?
Explanation
Explanation
52b 52c A bone-producing lesion in the metaphysis of an adolescent is most likely an osteosarcoma. The radiographs show a distal femoral bone-producing lesion extending into the surrounding soft tissues. The histologic appearance consists of pleomorphic cells producing osteoid. Ewing's sarcoma and metastatic neuroblastoma do not produce a matrix. Chondrosarcoma is a radiographically destructive lesion with calcification and cartilage cells on histologic section. An osteochondroma is a benign cartilage lesion that is continuous with the medullary cavity of the underlying bone and extends into a bony lesion and covered by a cartilage cap. Unni KK: Dahlin's Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 143-160.
References:
- Gibbs CP, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Question 70High Yield
Figures 20a and 20b show lateral and AP radiographs of a 49-year-old man who sustained a gunshot wound through the left shoulder. He reports neck pain and examination reveals weakness in all four extremities. What is the priority of evaluation?
Explanation
Explanation
20b The projectile entered the left shoulder and traveled to the right neck; therefore, a high incidence of suspicion must be directed to the airway, great vessels of the neck, and contents of the mediastinum. Immediate assessment of airway, breathing, and circulation takes priority, followed by examination of the neurologic status and other systems, as determined by the examination findings. Subcommittee on ATLS of the American College of Surgeons Committee on Trauma 1993-1997, Spine and Spinal Cord Trauma; Advanced Trauma Life Support Student Manual, ed 6, 1997. International Standards for Neurological and Functional Classification of Spinal Cord Injury. American Spinal Injury Association and International Medical Society of Paraplegia (ASIA/IMSOP).
Question 71High Yield
Figure 36 shows the radiograph of a 28-year-old man who injured his shoulder in a motocross race. Management should consist of
Explanation
Explanation
Fractures of the distal one third of the clavicle have a high incidence of delayed union (45% to 67%) and nonunion (22% to 33%) with nonsurgical management. Surgical stabilization with tension band techniques or a combination of plate and screw techniques is indicated, especially in young, active patients. In this patient, significant displacement of the fracture implies injury to the coracoclavicular ligaments with a higher risk of delayed union or nonunion. Various surgical treatments have been recommended, but the use of smooth wires is not indicated because of the potential for hardware migration. Jupiter JB, Ring D: Fractures of the clavicle, in Ianotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management, ed 1. Philadelphia, PA, Lippincott, Williams and Wilkins, 1999, pp 709-736.
References:
- Kona J, Bosse MJ, Staehli JW, Rosseau RL: Type II distal clavicle fractures: A retrospective review of surgical treatment. J Orthop Trauma 1990;4:115-120.
Question 72High Yield
The teardrop shape marked with an asterisk in Figure 61 represents what anatomic structure?
Explanation
Explanation
The teardrop can be visualized on the obturator outlet view of the pelvis and represents a thick column of bone that runs from the AIIS to the PSIS. Half pins for eternal fixation frames or screws can be inserted into this column for fixation of fractures. Gardner MJ, Nork SE: Stabilization of unstable pelvic fractures with supra-acetabular compression external fixation. J Orthop Trauma 2007;21:269-273. Haidukewych GJ, Kumar S, Prpa B: Placement of half-pins for supra-acetabular external fixation: An anatomic study. Clin Orthop Relat Res 2003;411:269-273.
Question 73High Yield
In a longitudinal study of children with spastic diplegia, analysis of long-term function will most likely reveal
Explanation
In a longitudinal study of 18 patients with spastic diplegia over a period of 32 months, three-dimensional gait analysis revealed a deterioration of gait stability with increases in double support time and decreases in single support time. Kinematic data also identified a loss of excursion about the knee, ankle, and pelvis. Interestingly, the static examination of the children showed a decrease in the popliteal angle over time. The authors concluded that ambulatory ability tends to worsen over time in children with spastic diplegia.
Question 74High Yield
Which of the following is considered the preferred approach to resect a lesion in the posterior one third of the proximal humerus?
Explanation
Explanation
At least 8 cm of the posterior aspect of the proximal region of the humeral diaphyseal cortex can be exposed through the interval between the lateral head of the triceps and the deltoid muscle. No nerves or blood vessels need to be exposed in the dissection. The deltoid muscle is innervated by the axillary nerve and the triceps muscle by the radial nerve. This is a true internervous plane.
References:
- Berger RA, Buckwalter JA: A posterior surgical approach to the proximal part of the humerus. J Bone Joint Surg Am 1989;71:407-410.
Question 75High Yield
Analysis of primary total hip arthroplasty using press-fit acetabular components without supplementary screw fixation reveals that screw fixation
Explanation
Using mechanical failure of fixation as the end point, Udomkiat and associates demonstrated a 12-year survivorship of 99.1% for titanium press-fit acetabular components without supplementary screw fixation. This study suggests that it is unlikely that the use of supplementary screws would lead to improved results. In addition, polyethylene wear debris tends to migrate through screw holes and along the course of screws. Screw holes also decrease the available surface for bone ingrowth. Screws that back up may be a source of backside polyethylene wear. This suggests that screw holes and the use of screws should be avoided when they are unnecessary for cup fixation.
Question 76High Yield
The use of multiagent adjuvant chemotherapy is associated with a clear survival benefit in which of the following diseases?
Explanation
Explanation
The use of multiagent chemotherapy has been shown to be associated with a survival benefit in patients with osteosarcoma. The use of chemotherapy in adults with soft-tissue sarcoma remains somewhat controversial. It has not been associated with improved survival rates in patients with renal carcinoma, dedifferentiated chondrosarcoma, or melanoma. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 53.
References:
- Link M, Goorin A, Miser A, et al: The effect of adjuvant chemotherapy and relapse free survival in patients with osteosarcoma of the extremity. N Engl J Med 1986;314:1600-1606.
Question 77High Yield
A 16-year-old ice hockey player is struck on the chest by the puck. He skates a few strides and then collapses. What is the most likely diagnosis?
Explanation
Sudden cardiac arrest following a blow to the chest in young athletes has been termed "commotio cordis." It is most common in Little League and other youth projectile sports (eg, ice hockey, lacrosse). The cause, although not completely determined, is most likely an arrhythmia related to the impact in a vulnerable time in the cardiac cycle. Resuscitation has proven to be exceedingly difficult, resulting in a high mortality rate. Maron BJ, Strasburger JF, Kugler JD, Bell BM, Brodkey FD, Poliac LC: Survival following blunt chest impact-induced cardiac arrest during sports activities in young athletes. Am J Cardiol 1997;79:840-841.
Question 78High Yield
A 45-year-old man who smokes reports the rapid onset of color changes and coolness in the fingers. Examination shows an abnormal Allen test. Plain radiographs of the hand and wrist are normal. Which of the following studies will best aid in diagnosis?

Explanation
The patient has symptoms typical of Raynaud's phenomenon secondary to underlying vascular disease. The next most appropriate step in the management of this patient should be to perform contrast angiography on the involved upper extremity to look for proximal or distal arterial lesions or insufficiencies. MRI and contrast CT are not as specific as angiography for the identification of vascular lesions of the upper extremity. Although patients with primary Raynaud's vasospastic disease can have normal angiographic findings, they typically are younger than age 40 years, are female, and have normal results on an Allen test. Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 2288-2290.
Question 79High Yield
What is the most common neurologic complication following an anterior cervical diskectomy and fusion?
Explanation
The recurrent laryngeal nerve provides innervation to the vocal cords and was the most common neurologic injury reported in a series of 36,000 patients. The nerve is felt to be more vulnerable during a right-sided approach because of its anatomic course. A recent study has also suggested a role for increased endotracheal cuff pressures in this nerve injury. Flynn TB: Neurologic complications of anterior cervical interbody fusion. Spine 1982;7:536-539.
Question 80High Yield
A 22-year-old cheerleader who fell from the top of a pyramid now reports anterior and posterior pelvic pain. A radiograph and CT scans are shown in Figures 43a through 43c. What is the best treatment for this injury?

Explanation
Symphyseal widening of greater than 2.5 cm and less than 5 cm denotes an AP II injury and a rotationally unstable pelvis. An AP II pelvic ring injury is best treated with anterior open reduction and internal fixation. Nonsurgical management is reserved for AP I injuries. Pelvic binders are used only acutely and should not be used for definitive management. Iliosacral screws usually are not necessary in the acute management of AP II injuries. Matta JM: Indications for anterior fixation of pelvic fractures. Clin Orthop Relat Res 1996;329:88-96. Templeman DC, Schmidt AH, Sems AS, et al: Diastasis of the symphysis pubis: Open reduction internal fixation, in Wiss D (ed): Masters Techniques in Orthopaedic Surgery-Fractures, ed 2. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 639-648.
Question 81High Yield
A 58-year-old reports pain and stiffness in his left shoulder following a seizure episode. Diagnosis at the time of the seizure is a frozen shoulder, and management consists of an aggressive physical therapy program of stretching exercises. Four months later he continues to have shoulder pain and has not gained any additional range of motion. A CT scan is shown in Figure 50. Management should now consist of

Explanation
Humeral arthroplasty is indicated for chronic posterior dislocations when the impression defect in the humeral head is greater than 45% to 50%. If the condition remains undiagnosed for more than 9 to 12 months, secondary degenerative changes on the glenoid may occur, necessitating total shoulder arthroplasty. Open reduction and transfer of the subscapularis and lesser tuberosity are used for impression defects that consist of 20% to 40% of the humeral articular surface. Closed reduction and immobilization with the arm in slight extension and external rotation is useful when the posterior dislocation is diagnosed within the first 6 weeks and the articular defect is less than 20%. Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Question 82High Yield
Figure 18a shows the clinical photograph of a 31-year-old man who has a slowly growing nodule on his right middle finger. It is minimally tender, and there is no erythema on examination. A biopsy specimen is shown in Figure 18b. What is the most likely diagnosis?
Explanation
Explanation
18b Epithelioid sarcoma is the most common soft-tissue sarcoma in the hand and most commonly occurs in young adults. The tumors can be superficial and may become ulcerated. Deeper lesions are often attached to tendons, tendon sheaths, or fascial structures. These are usually minimally symptomatic. The biopsy specimen reveals the typical appearance of a nodular pattern with central necrosis. They can mimic a necrotizing granulomatous process. Usually there are chronic inflammatory cells along the margin of the tumor nodules. This biopsy specimen does not have the clear cells necessary for a clear cell carcinoma or sarcoma. Nora's tumor is a bizarre parosteal osteochondromatous proliferation (BPOP) first described in 1983 by the pathologist, Nora. The lesion is defined as a reactive heterotopic ossification and is mostly found in the hands or feet of adults in the third decade of life. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 1074.
References:
- Halling AC, Wollan PC, Pritchard DJ, et al: Epithelioid sarcoma: A clinicopathologic review of 55 cases. Mayo Clin Proc 1996;71:636-642.
Question 83High Yield
Which of the following positions of immobilization has been shown to best approximate the anterior labrum against the glenoid rim following anterior dislocation of the shoulder?
Explanation
Explanation
Following anterior dislocation of the shoulder, the affected arm is typically placed in a sling with the shoulder in adduction and internal rotation. A recent study has shown that placement in this position actually results in laxity of the anterior supporting structures of the shoulder, allowing the postinjury hemarthrosis to push the labrum and capsular ligaments away from the anterior glenoid rim. Thus, immobilization in this position may actually impede healing of these structures. Alternatively, resting the arm in a position of adduction and external rotation allows the anterior supporting structures to abut against the anterior glenoid rim by forcing the hemarthrosis posteriorly. Placing the arm in this position following anterior dislocation is believed to allow for better healing of the anterior labrum and ligaments.
References:
- Itoi E, Sashi R, Minagawa H, et al: Position of immobilization after dislocation of the glenohumeral joint: A study with use of magnetic resonance imaging. J Bone Joint Surg Am 2002;84:873-874.
Question 84High Yield
A 43-year-old woman has had pain in the left hip for the past 2 months. A radiograph, CT scan, MRI scan, and biopsy specimens are shown in Figures 16a through 16e. What is the most likely diagnosis?
Explanation
Explanation
16b 16c 16d 16e The imaging studies are consistent with a chondrosarcoma. The radiograph shows a radiolucent lesion in the pelvis, and there are stippled calcifications on the CT scan. The histology shows a low-grade cellular hyaline cartilage neoplasm with stellate, occasionally binucleated chondrocytes. Enchondroma has a more benign histologic appearance.
References:
- Mirra JM, Gold R, Downs J, Eckardt JJ: A new histologic approach to the differentiation of enchondroma and chondrosarcoma of the bones: A clinicopathologic analysis of 51 cases. Clin Orthop 1985;201:214-237.
Question 85High Yield
Patients who have osteonecrosis of the humeral head and who have the best prognosis are those with which of the following conditions?
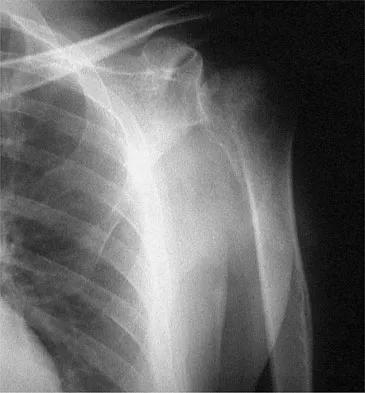
Explanation
The natural history of nontraumatic osteonecrosis varies greatly, so it is difficult to predict which patients will have severe arthrosis develop. Patients with sickle cell disease tend to have the most benign course. The most commonly reported cause of nontraumatic osteonecrosis is corticosteroid therapy. Fortunately, the incidence of osteonecrosis among patients treated with long-term systemic corticosteroids has fallen from more than 25% to less than 5% in recent years, owning to judicious steroid use and dosing. The interval between corticosteroid administration and the onset of shoulder symptoms is also variable, ranging from 6 to 18 months in one large series. This is comparable to the interval leading up to the onset of hip symptoms, which ranges from 6 months to 3 years or longer. The incidence of humeral head involvement has not been shown to vary with the underlying indication for steroid use. Hasan SS, Romeo AA: Nontraumatic osteonecrosis of the humeral head. J Shoulder Elbow Surg 2002;11:281-298.
Question 86High Yield
A patient who has recalcitrant medial plantar heel pain and pain directly over the medial side of the heel undergoes open release of the plantar fascia. After releasing a portion of the plantar fascia, the deep fascia of the abductor hallucis muscle is released to relieve pressure on which of the following structures?
Explanation
Explanation
The deep fascia of the abductor hallucis muscle is released to relieve pressure on the first branch of the lateral plantar nerve. The tibial nerve lies more proximal to this area. The medial plantar nerve has already passed dorsally and medially, while the sural nerve lies on the lateral side of the foot. The flexor hallucis brevis muscle lies deep to the plantar fascia, not the abductor fascia. Baxter DE, Pfeffer GB: Treatment of chronic heel pain by surgical release of the first branch of the lateral plantar nerve. Clin Orthop 1992;279:229-236.
References:
- Davies MS, Weiss GA, Saxby TS: Plantar fasciitis: How successful is surgical intervention? Foot Ankle Int 1999;20:803-807.
Question 87High Yield
Passive glycation of articular cartilage results in
Explanation
Passive glycation of articular cartilage occurs over decades. One of the consequences of this glycation appears to be the stiffening of collagen. This phenomenon appears to be associated with an increased collagen degradation and development of osteoarthrosis. Passive glycation also results in a relatively yellow appearance. Passive glycation does not directly influence chondrocyte proliferation. DeGroot J, Verzijl N, Wenting-van Wijk MJ, et al: Accumulation of advanced glycation end products as a molecular mechanism for aging as a risk factor in osteoarthritis. Arthritis Rheum 2004;50:1207-1215.
Question 88High Yield
A 28-year-old woman fell on her right wrist while rollerblading 2 days ago. She was seen in the emergency department at the time of injury and was told she had a sprain. Examination now reveals dorsal tenderness in the proximal wrist but no snuffbox or ulnar tenderness. Standard wrist radiographs are normal. What is the next most appropriate step in management?
Explanation
Explanation
When considering the diagnosis of scapholunate ligament injury, standard radiographic views of the hand will not always reveal widening of the scapholunate gap. Although MRI may reveal injury to the ligaments, the PA clenched fist view can be obtained in the office during the initial patient visit. Arthroscopy is not a first-line diagnostic tool. Walsh JJ, Berger RA, Cooney WP: Current status of scapholunate interosseous ligament injuries. J Am Acad Orthop Surg 2002;10:32-42.
References:
- Browner BD, Levine AM, Jupiter JB, et al (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1366-1367.
Question 89High Yield
Which of the following design features of a femoral component used in a total knee arthroplasty best minimizes the patellar component contact stresses?
Explanation
Explanation
Several studies have shown that design of the femoral component, especially the trochlear groove portion, largely influences patellar tracking and patellofemoral contact stresses. A deep, curved anatomic femoral trochlear groove has been shown to have the lowest contact stresses. Petersilge WJ, Oishi CS, Kaufman KR, Irby SE, Colwell CW Jr: The effect of trochlear design on patellofemoral shear and compressive forces in total knee arthroplasty. Clin Orthop 1994;309:124-130. Theiss SM, Kitziger KJ, Lotke PS, Lotke PA: Component design affecting patellofemoral complications after total knee arthroplasty. Clin Orthop 1996;326:183-187.
References:
- Healy WL, Wasliewski SA, Takei R, Oberlander M: Patellofemoral complications following total knee arthroplasty:. Correlation with implant design and patient risk factors. J Arthroplasty 1995;10:197-201.
Question 90High Yield
Figures 26a through 26c show the MRI scans of a 47-year-old man who underwent arthroscopic shoulder surgery 6 months ago and continues to have pain despite a prolonged course of rehabilitation. Management should now consist of
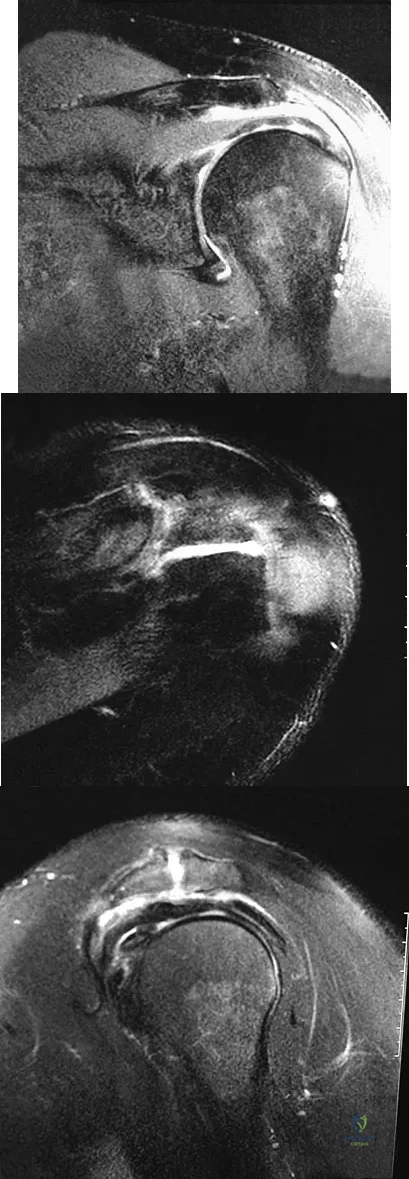
Explanation
The MRI scans show an os acromiale of the mesoacromion type. This represents an unfused acromial apophysis. Pain is thought to be caused by either motion at the site or downward displacement of the anterior aspect of the acromion onto the rotator cuff, causing impingement. Most patients can be treated nonsurgically as they are usually asymptomatic. In those patients with persistent symptoms of pain and tenderness over the acromion, surgery consisting of rigid internal fixation and bone grafting has yielded satisfactory results. Excision may be a viable treatment option for the preacromion type. Herzog RJ: Magnetic resonance imaging of the shoulder. Instr Course Lect 1998;47:3-20. Warner JP, Beim GM, Higgins L: The treatment of symptomatic os acromiale. J Bone Joint Surg Am 1998;80:1320-1326.
Question 91High Yield
A 24-year-old man sustains the injury shown in Figures 19a through 19e in a paragliding accident. He is neurologically intact. He also sustained fractures of his left femur and right distal radius. Which of the following represents the best option for management of the spinal injury?
Explanation
Explanation
19b 19c 19d 19e The injury pattern is that of a burst fracture at L1 contiguous with a compression fracture at T12. There is associated kyphosis and slight spondylolisthesis of T12 on L1. Treatment of this type of burst fracture in neurologically intact patients is somewhat controversial, with at least one study demonstrating equal long-term results comparing nonsurgical treatment to surgical treatment. In this study, however, body casts were used initially in the nonsurgical group. Moreover, because this patient has multiple fractures, spinal fracture stabilization should be considered to facilitate early mobilization. Surgical stabilization and fusion via a posterior approach is the best treatment option in this patient. Anterior decompression is not necessary since the patient is neurologically intact. McLain RF, Benson DR: Urgent surgical stabilization of spinal fractures in polytrauma patients. Spine 1999;24:1646-1654. Wood K, Butterman G, Mehbod A, et al: Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit: A prospective, randomized study. J Bone Joint Surg Am 2003;85:773-781.
Question 92High Yield
Which of the following radiographic views best depicts a Hill-Sachs defect?

Explanation
The Stryker notch view best shows this type of defect. An outlet view helps evaluate acromial shape, a true AP shows joint space narrowing, a serendipity view evaluates the sternoclavicular joint, and a Zanca view helps evaluate the acromioclavicular joint. An internal rotation AP may also depict a Hill-Sachs defect.
Question 93High Yield
A 42-year-old patient has had a fever and low back pain for several days. Laboratory studies show an elevated erythrocyte sedimentation rate and a WBC count of 9,500 mm3 with 75% neutrophils. A CT scan is shown in Figure 15. Examination will most likely reveal what other findings?

Explanation
The CT scan reveals a left-sided psoas abscess. Irritation of the saphenous division of the femoral nerve can cause paresthesias along the medial aspect of the knee. Pain is usually improved with hip flexion. Cellier C, Gendre JP, Cosnes J, et al: Psoas abscess complication Crohn's disease. Gastroenterol Clin Biol 1992;16:235-238.
Question 94High Yield
Why is tendon considered an anisotropic material?
Explanation
Explanation
Anisotropic materials have mechanical properties that vary based on the direction of loading. The relative values of Young's modulus for tendon, ligament, and bone are not relevant to isotropy. The mechanical properties of tendon do change with preconditioning, but this change is related to viscoelasticity. The intrinsic mechanical properties of tendon do vary with the rate of loading, but this variance is related to viscoelasticity. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 134-180.
References:
- Lu L, Kaufman KR, Yaszemski MJ: Biomechanics, in Einhorn TA, O'Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 95High Yield
Patients in compensated shock (normal vital signs) are thought to be at risk for which of the following?
Explanation
Patients who are in compensated shock have normal vital signs but still have hypoperfusion of organ beds such as the splanchnic circulation due to preferential perfusion of the heart and brain. The response to this continued hypoperfusion may be the development of a systemic inflammatory response that may lead to multiple organ failure. The patients are thought to be at risk for a "primed" immune system due to the ongoing stimulation of the immune system and may have an exaggerated response to a second stimulus such as surgery or infection. Other markers of resuscitation should be used besides vital signs to determine when resuscitation has been completed. The use of temporizing fixation has been shown to lower systemic complication rates, and the infection and union rate after staged fixation is not altered. Schulman AM, Claridge JA, Carr G, et al: Predictors of patients who will develop prolonged occult hypoperfusion following blunt trauma. J Trauma 2004;57:795-800.
Question 96High Yield
A 30-year-old woman injured her ankle playing soccer 3 months ago. She now reports popping and pain over the lateral side of her ankle. An MRI scan is shown in Figure 33. What structure needs to be repaired to alleviate the popping?
Explanation
Explanation
The symptoms and MRI scan indicate dislocated peroneal tendons. In this patient, the structure that needs to be repaired is the superior peroneal retinaculum. If the popping was coming from a torn peroneal tendon, repair would involve the peroneal longus or brevis tendon, but this is not shown in the MRI scan. The anterior talofibular ligament or the calcaneofibular ligament would need to be repaired if the patient had ankle instability due to an ankle sprain. Jones DC: Tendon disorders of the foot and ankle. J Am Acad Orthop Surg 1993;1:87-94.
Question 97High Yield
Figures 26a and 26b show the radiograph and MRI scan of a 22-year-old man with knee pain. What is the most likely diagnosis?
Explanation
Explanation
26b The lesion is an osteochondroma. This is demonstrated by a pedunculated bone-forming lesion where the medullary space of the lesion communicates with the medullary space of the host bone. The cortex of the exostosis is in continuity with the cortex of the underlying bone. The MRI scan reveals that there is no significant cartilage cap, alleviating concern for malignant conversion to a chondrosarcoma. Osteoblastoma and osteosarcoma typically have mixed areas of bone formation and bone destruction. Malignant fibrous histiocytoma of bone is usually purely lytic. Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 197-215.
References:
- Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Question 98High Yield
In the first dorsal compartment of the wrist, what tendon most frequently contains multiple slips?
Explanation
The first extensor compartment of the wrist typically contains a single extensor pollicis brevis tendon and the abductor pollicis longus tendon that nearly always has multiple tendon slips. The extensor pollicis brevis tendon is frequently found to be separated from the slips of the abductor pollicis longus tendon by an intracompartmental septum. During surgery, this septum must be divided to complete the release of the compartment. Jackson WT, Viegas SF, Coon TM, Stimpson KD, Frogameni AD, Simpson JM: Anatomical variations in the first extensor compartment of the wrist: A clinical and anatomical study. J Bone Joint Surg Am 1986;68:923-926.
Question 99High Yield
A 53-year-old woman has severe neck and left shoulder pain after a rollover motor vehicle accident. Radiographs and a CT scan of the cervical spine are shown in Figures 34a through 34c. Management should consist of
Explanation
Explanation
34b 34c The plain radiographs show a horizontal orientation of the C5 facet joint. The CT scan through C5 reveals an ipsilateral pedicle and lamina fracture (floating facet). This injury involves two adjacent motion segments and is extremely unstable. Lateral mass plates, with or without the purchase of the "floating facet," provide the best means of stabilization and should include the facet above (C4) and below (C6) the level of injury. Orthotic immobilization is insufficient for this particular injury. Halo vest treatment does not control the subaxial spine well and is of limited value. While simple midline (Rogers) wiring provides some tension band restoration, it is not optimal for rotational control. The use of lateral mass plates provides rotational stability. Another option would be anterior fusion and plating, which would save cervical segments. Levine AM, Mazel C, Roy-Camille R: Management of fracture separations of the articular mass using posterior cervical plating. Spine 1992;17:S447-S454. Levine AM: Facet fractures and dislocations, in Levine AM, Eismont FJ, Garfin S, Zigler JE (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 360-362. Whitehill R, Richman JA, Glaser JA: Failure of immobilization of the cervical spine by the halo vest: A report of five cases. J Bone Joint Surg Am 1986;68:326-332.
References:
- Garvey TA, Eismont FJ, Roberti LJ: Anterior decompression, structural bone grafting, and Caspar plate stabilization for unstable cervical spine fractures and/or dislocations. Spine 1992;17:S431-S435.
Question 100High Yield
What changes in muscle physiology would be expected in an athlete who begins a rigorous aerobic program for an upcoming marathon?
Explanation
Muscle fibers can be categorized grossly into two types. Type I muscle, also known as slow-twitch muscle, is responsible for aerobic, oxidative muscle metabolism. It has a much lower strength and speed of contraction than fast-twitch type II muscle but is significantly more fatigue resistant. With training for endurance sports, the type I muscle undergoes adaptive changes to the increased stress. Increases in capillary density, oxidative capacity, mitochondrial density, and subsequent fatigue resistance are all observed changes. Hypertrophy of type IIb muscle is seen in strength training. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 89-125.
