
After Reduction: Securing Your Fracture with ...
00:00
Start Quiz
A 53-year-old man has a 4- x 5-cm high-grade soft-tissue sarcoma in the midthigh. As part of the staging evaluation, regional nodes should be assessed by

Explanation
In general, soft-tissue metastases to regional nodes are a relatively rare occurrence (less than 5% overall). The incidence of lymphatic metastasis is highest for synovial sarcoma, rhabdomyosarcoma, clear cell sarcoma, and epithelioid sarcoma. Regional nodes should be assessed clinically. CT is not used to routinely assess regional nodes. Evaluation of a sentinal node is not indicated because of the low incidence of regional nodal involvement. Fine needle aspiration may be indicated to assess clinically suspicious nodes. Prophylactic inguinal node dissection is contraindicated because it may lead to unnecessary complications such as lymphedema.
- Bottoni CR, Wilckens JH, DeBerardino TM, et al: A prospective, randomized evaluation of arthroscopic stabilization versus nonoperative treatment in patients with acute, traumatic, first-time shoulder dislocations. Am J Sports Med 2002;30:576-580.
Question 3High Yield
A 26-year-old man sustains a displaced bimalleolar fracture by sliding into second base while playing baseball. Following initial closed reduction and splinting of the fracture, moderate swelling is noted. What is the safest time to perform surgery?
Explanation
Explanation
Following any closed fracture, the most important determinant for the timing of surgery is the condition of the soft tissues and especially the skin. The best determinant of appropriate soft-tissue condition is the presence of wrinkling of the skin (wrinkle sign) at the site of the incision. A wrinkle sign is present when all the interstitial edema has left the skin; this may take up to 14 to 21 days of elevation. Any abrasion must be epithelialized so that there are no bacteria left at the site. To date, no other method of soft-tissue viability measurement has been shown to be of any clinical benefit. Stover MD, Kellam JF: Articular fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 105-119. Hahn DM, Colton CL, Malleolar fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 559-581.
References:
- Tile M: Fractures of the ankle, in Schatzker J, Tile M (eds): Rationale of Operative Fracture Care, ed 2. Berlin, Springer-Verlag, 1998, pp 523-561.
Question 4High Yield
A toddler is brought in by his parents for evaluation of gait problems. Birth history and neurologic examination are unremarkable. After evaluating femoral torsion, tibial torsion, and foot contour, the diagnosis is excessive internal tibial torsion. The parents should be advised to expect which of the following outcomes?
Explanation
Explanation
Excessive internal tibial torsion is a common cause of intoeing in toddlers. In most children, this resolves spontaneously by 3 to 4 years of age. Intoeing in elementary age children is usually the result of excessive femoral anteversion. Studies have shown that active intervention (casting, splinting, and shoe modifications) has no demonstrable effect on the natural history or resolution of tibial torsion. Surgery is rarely indicated in adolescents with severe internal tibial torsion that has not resolved and is resulting in cosmetic and functional problems. Canale ST, Beaty JH: Operative Pediatric Orthopaedics. St Louis, MO, Mosby Year Book, 1991, pp 357-385.
Question 5High Yield
Patients in compensated shock (normal vital signs) are thought to be at risk for which of the following?
Explanation
Patients who are in compensated shock have normal vital signs but still have hypoperfusion of organ beds such as the splanchnic circulation due to preferential perfusion of the heart and brain. The response to this continued hypoperfusion may be the development of a systemic inflammatory response that may lead to multiple organ failure. The patients are thought to be at risk for a "primed" immune system due to the ongoing stimulation of the immune system and may have an exaggerated response to a second stimulus such as surgery or infection. Other markers of resuscitation should be used besides vital signs to determine when resuscitation has been completed. The use of temporizing fixation has been shown to lower systemic complication rates, and the infection and union rate after staged fixation is not altered. Schulman AM, Claridge JA, Carr G, et al: Predictors of patients who will develop prolonged occult hypoperfusion following blunt trauma. J Trauma 2004;57:795-800.
Question 6High Yield
In a longitudinal study of children with spastic diplegia, analysis of long-term function will most likely reveal
Explanation
In a longitudinal study of 18 patients with spastic diplegia over a period of 32 months, three-dimensional gait analysis revealed a deterioration of gait stability with increases in double support time and decreases in single support time. Kinematic data also identified a loss of excursion about the knee, ankle, and pelvis. Interestingly, the static examination of the children showed a decrease in the popliteal angle over time. The authors concluded that ambulatory ability tends to worsen over time in children with spastic diplegia.
Question 7High Yield
Figures 32a and 32b show the AP and lateral radiographs of an 11-year-old boy who has a severe limp, a fever, and swelling and tenderness of the thigh. Aspiration of the bone reveals purulent material. The patient has most likely been symptomatic for

Explanation
In patients with an osteomyelitic infection, radiographic findings at 1 to 5 days usually show soft-tissue swelling only. Seven to 14 days after symptoms begin, radiographs will most likely show the classic signs of acute osteomyelitis. Reactive bone formation would be expected by 6 months. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 149-161.
Question 8High Yield
Figure 24 shows an axial MRI scan of the ankle. The arrowhead is pointing to what structure?
Explanation
Explanation
The peroneus brevis is easily identified by its location behind the fibula and its distal muscle belly. Axial MRI images provide a reliable guide even when one of the peroneals is completely ruptured, subluxated out of the peroneal groove, or absent. Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. New York, NY, Lippincott, 1993, pp 234-235.
References:
- Sammarco GJ: Peroneus longus tendon tears: Acute and chronic. Foot Ankle Int 1995;16:245-253.
Question 9High Yield
A 21-year-old man has mild but persistent aching pain in his left proximal thigh during impact loading activities. He denies pain at rest and has no other symptoms. Figures 34a through 34e show the radiographs and T1-weighted, T2-weighted, and gadolinium MRI scans of the left hip. What is the most likely diagnosis?
Explanation
Explanation
34b 34c 34d 34e The radiographs show a centrally located radiolucent lesion with cortical thinning and mild osseous expansion; these findings are the hallmarks of a simple bone cyst. Whereas this particular lesion does not demonstrate sclerosis, the distinct margin of this lesion with sharp transition to normal bone is common. The MRI scans reveal a purely cystic lesion with bright T2 signal, and the gadolinium image shows the classic rim enhancement of cystic lesions. Fibrous dysplasia with cystic degeneration might have a very similar appearance and should be considered in the differential diagnosis. Parsons TW: Benign bone tumors, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1027-1035. May DA, Good RB, Smith DK, et al: MR imaging of musculoskeletal tumors and tumor mimickers with intravenous gadolinium: Experience with 242 patients. Skeletal Radiol 1997;26:2-15.
References:
- Resnick D, Kyriakos M, Greenway GD: Tumors and tumor-like lesions of bone: Imaging and pathology of specific lesions, in Resnick D (ed): Diagnosis of Bone and Joint Disorders, ed 4. Philadelphia, PA, WB Saunders, 2002, vol 4, pp 4023-4034.
Question 10High Yield
A 69-year-old man sustains a traumatic amputation to the distal phalanx of his little finger while working with power tools. Radiographs are shown in Figures 27a and 27b. The patient was instructed how to perform wet-to-dry dressing changes in the emergency department. Clinical pictures taken in the office are shown in Figures 27c through 27e. What is the most appropriate management of this soft-tissue wound?
Explanation
Explanation
27b 27c 27d 27e The clinical photographs and radiographs reveal a distal phalangeal amputation with soft-tissue coverage over nonexposed bone. This is an ideal circumstance to allow healing by secondary intention with wet-to-dry dressing changes. There are few complications and the aesthetics surpass that of any soft-tissue reconstruction procedure. Volar advancement flaps (Moberg flaps) are limited to small defects about the thumb. A thenar flap will provide good coverage; however, the results are not comparable to simple dressing changes. A V-Y flap is useful when there is more tissue loss dorsally. Jebson PL, Louis DS: Amputations, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green's Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 1947.
Question 11High Yield
Examination of a 7-year-old boy reveals 20 degrees of valgus following a lawn mower injury to the lateral femoral epiphysis. Treatment consists of total distal femoral epiphyseodesis and varus osteotomy. Following surgery, he has a limb-length discrepancy of 3 cm and 5 degrees of genu valgum. Assuming that he undergoes no further treatment, the patient's predicted limb-length discrepancy at maturity would be how many centimeters?
Explanation
The distal femoral epiphysis grows approximately 1 cm per year and in boys, growth ceases at approximately age 16 years. Therefore, the patient's limb-length discrepancy at maturity would be 12 cm (9 cm plus the 3-cm discrepancy he has from the previous surgery). Little DG, Nigo L, Aiona MD: Deficiencies of current methods for the timing of epiphyseodesis. J Pediatr Orthop 1996;16:173-179.
Question 12High Yield
An 80-year-old woman notes a painless mass posterior to her left knee. MRI scans are shown in Figures 31a and 31b. What is the best course of action?
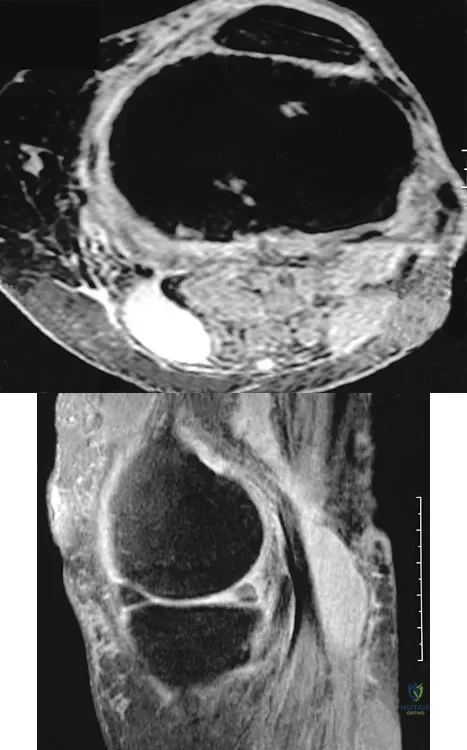
Explanation
The MRI scans show a popliteal cyst (Baker's cyst) in its most common location. The cyst emerges from the knee joint between the medial head of the gastrocnemius muscle and the tendon of the semimembranosus muscle. These images are diagnostic; therefore, no further work-up is indicated. Since the patient is asymptomatic, no treatment is necessary. Dlabach JA: Nontraumatic soft tissue disorders, in Canale ST (ed): Campbell's Operative Orthopaedics, ed 10. Philidelphia, PA, Mosby, 2003, vol 1, pp 885-969.
Question 13High Yield
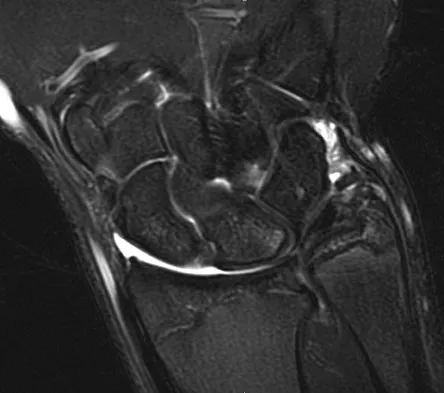
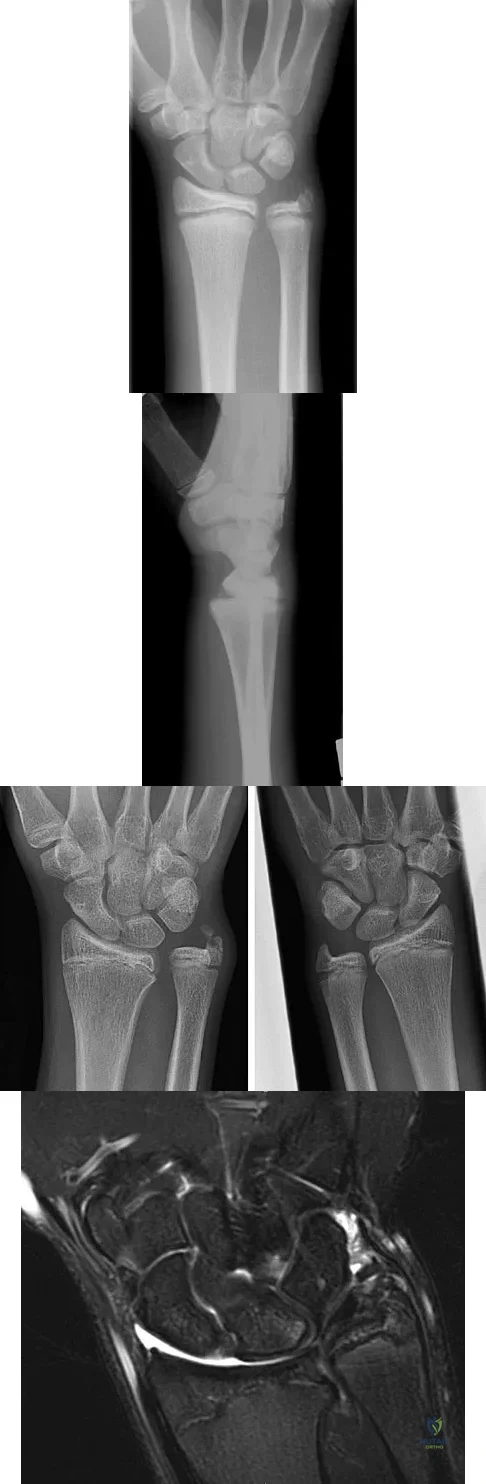
A 21-year-old man who was injured in a snowboarding accident 18 months ago now reports wrist pain. An MRI scan is shown in Figure 37. Based on the image findings, what is the most likely diagnosis?
Explanation
Explanation
The coronal MRI scan of the wrist shows the scaphoid. There is a subtle fracture line with a step-off at the radial surface consistent with a nonunion. The signal intensity is markedly different between the two fragments of the scaphoid. This strongly suggests osteonecrosis. Preiser's disease is osteonecrosis typically involving most or all of the scaphoid. Kienbock's disease involves the lunate. Intraosseous ganglia are easily diagnosed on MRI but typically have a fluid-filled area surrounded by denser bone in the periphery. Scapholunate dissociation can be seen on MRI as an injury to the scapholunate ligament and widening of the scapholunate interval, neither of which is seen on this image.
References:
- Perlik PC, Guilford WB: Magnetic resonance imaging to assess vascularity of scaphoid nonunions. J Hand Surg Am 1991;16:479-484.
Question 14High Yield
A 20-year-old football player has immediate pain in the midfoot and is unable to bear weight after an opposing player lands on the back of his plantar flexed foot. AP and lateral radiographs are shown in Figures 4a and 4b. Management should consist of
Explanation
Explanation
4b The history and radiographs indicate a Lisfranc fracture-dislocation of the foot. The radiographs show the classic "fleck sign," which is an avulsion of the Lisfranc ligament from the base of the second metatarsal. Most authors recommend open reduction and internal fixation of this injury. Closed reduction can be attempted, but anatomic reduction is unlikely because of the interposed bone fragments and soft tissues. Standard radiographs are not reliable in identifying 1 to 2 mm of subluxation of the tarsometatarsal joint. The tarsometatarsal joint has a poor tolerance to even mild subluxation, and the resulting decrease in joint contact area increases the likelihood of posttraumatic arthritis. Open reduction with the joint visible allows more anatomic reduction and internal fixation of larger osteochondral fragments or excision of smaller interposed fragments. Bellabarba C, Sanders R: Dislocations of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 2, pp 1539-1558.
References:
- Murphy GA: Fractures and dislocations of the foot, in Canale ST (ed): Campbell's Operative Orthopaedics, ed 9. St Louis, MO, Mosby, 1998, vol 2, pp 1956-1960.
Question 15High Yield
When compared to smokers who do not quit, an improvement in the rate of lumbar fusion is seen in patients who cease smoking for at least how many months postoperatively?
Explanation
Explanation
The effects of cigarette smoking and smoking cessation on spinal fusion have been studied extensively. Although permanent smoking cessation is ideal, significant improvements in fusion rates are seen in patients who avoid smoking for greater than 6 months postoperatively.
Question 16High Yield
What is the most common surgical cause of the foot deformity shown in Figure 9?

Explanation
The radiograph shows a hallux varus deformity. Iatrogenically acquired hallux varus is most often the result of excessive lateral soft-tissue release, sesamoidectomy, or both. It also can be caused by a medial tibial sesamoid subluxation in conjunction with excessive postoperative dressing application, overcorrection of the intermetatarsal angle, or excessive medial eminence resection. Donley BG: Acquired hallux varus. Foot Ankle Int 1997;18:586-592.
Question 17High Yield
A farmer is seen in the emergency department after falling out of a hay loft onto the barn floor below. He is unable to bear weight. Exploration of a 0.5 cm laceration over the anterior tibia reveals bone. Radiographs reveal oblique displaced midshaft tibial and fibular fractures. Based on these findings, what is the most appropriate antibiotic prophylaxis?
Explanation
Explanation
A farm injury is automatically considered a grade III (Gustillo classification) injury regardless of size, energy, or additional soft-tissue injury due to the likelihood of substantial contamination. Antibiotic recommendations for grade III injuries include a first- or second-generation cephalosporin with an aminoglycoside or fluoroquinolone within 3 hours of injury, with penicillin added for farm injuries. Okike K, Bhattacharyya T: Trends in the management of open fractures: A critical analysis. J Bone Joint Surg Am 2006;88:2739-2748.
Question 18High Yield
A 30-year-old woman injured the ring finger of her nondominant hand while playing baseball 5 weeks ago. She now reports pain and limited motion of the proximal interphalangeal (PIP) joint. A lateral fluoroscopy image is shown in Figure 36. Treatment of the PIP joint should consist of
Explanation
Explanation
The patient has a neglected PIP joint fracture-dislocation with comminution involving more than 40% of the volar articular surface of the middle phalanx. Volar plate arthroplasty has been advocated for the treatment of acute unstable and chronic dorsal fracture-dislocations. The volar plate is incised laterally and released from the collateral ligaments. The volar fragments of the middle phalanx are removed and a trough is created for advancement of the volar plate, which is secured with sutures secured on the dorsum of the middle phalanx beneath the extensor mechanism. Dionysian E, Eaton RG: The long-term outcome of volar plate arthroplasty of the proximal interphalangeal joint. J Hand Surg Am 2000;25:429-437. Eaton RG, Malerich MM: Volar plate arthroplasty of the proximal interphalangeal joint: A review of ten years' experience. J Hand Surg Am 1980;5:260-268.
Question 19High Yield
Figures 17a and 17b show the radiographs of a 32-year-old professional athlete who sustained an injury to the first metatarsal. A view of the opposite noninjured side is shown in Figure 17c. Management of the fracture should consist of
Explanation
Explanation
17b 17c Parameters for first metatarsal fracture management are different than for shaft fractures of the central second, third, and fourth metatarsals. The first metatarsal carries a greater load and if malunited, can create transfer lesions by virtue of uneven weight distribution; therefore, nonsurgical management is not indicated for this patient. Percutaneous pinning is not as likely to result in an anatomic reduction as open reduction and internal fixation. As his livelihood depends on an expeditious return to function, the choice of open reduction and internal fixation allows for earlier motion and rehabilitation. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 64-65.
References:
- Shereff MJ: Compartment syndromes of the foot. Instr Course Lect 1990;39:127-132.
Question 20High Yield
In a patient who has had low back pain for less than 2 weeks, which of the following findings is an indication for continued observation and symptomatic treatment rather than more aggressive evaluation and/or treatment?
Explanation
An inability to participate in athletics generally is considered an indication for continued symptomatic treatment only. All of the other answers suggest the possibility of more significant pathology that may require more urgent treatment. Frymoyer JW: Back pain and sciatica. N Engl J Med 1988;318:291-300.
Question 21High Yield
A 58-year-old woman has had a painless periscapular mass for the past year. An MRI scan and biopsy specimen are shown in Figures 4a and 4b. What is the most likely diagnosis?
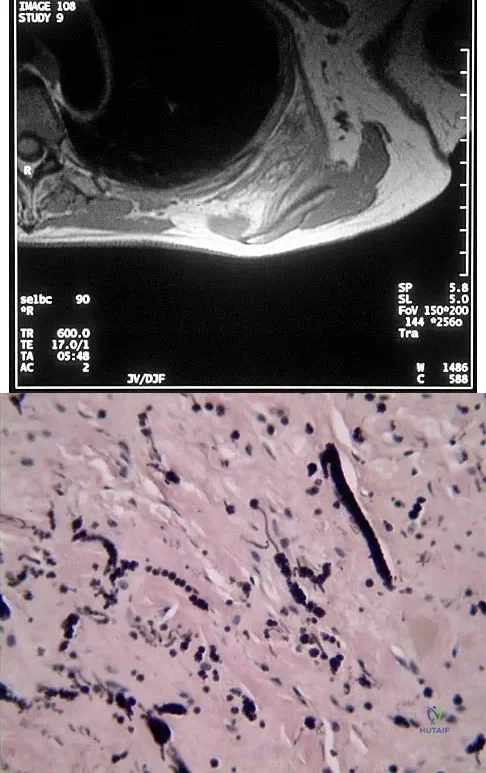
Explanation
Elastofibroma is a rare tumor that most commonly occurs in adults who are older than age 55 years. The lesions usually grow between the chest wall and the scapula, and 10% are bilateral. Histologic analysis shows that they are composed of equal amounts of elastin and collagen with occasional fibroblasts. Briccoli A, Casadei R, Di Renzo M, Favale L, Bacchini P, Bertoni F: Elastofibroma dorsi. Surg Today 2000;30:147-152.
Question 22High Yield
Which of the following is considered a contraindication to cement injection techniques, such as kyphoplasty or vertebroplasty, in the treatment of osteoporotic compression fractures?
Explanation
Explanation
When retropulsion of the posterior vertebral wall is present, nothing prohibits the cement from following the path of least resistance into the canal or from pushing a bone fragment further into the canal; most clinicians consider it a contraindication to these techniques. Patient age itself is not a contraindication as long as there are no medical contraindications to surgery. An acute fracture in a patient who remains immobile and hospitalized because of pain may be a good indication for such a technique. Prior compression fracture and older compression fractures are not contraindications, but pain relief may be less predictable. Phillips FM, Pfeifer BA, Leiberman IH, et al: Minimally invasive treatment of osteoporotic vertebral compression fractures: Vertebroplasty and kyphoplasty. Instr Course Lect 2003;52:559-567. Truumees E, Hilibrand A, Vaccaro AR: Percutaneous vertebral augmentation. Spine J 2004;4:218-229.
References:
- Rao RD, Singrakhia MD: Painful osteoporotic vertebral fracture: Pathogenesis, evaluation, and roles of vertebroplasty and kyphoplasty in its management. J Bone Joint Surg Am 2003;85:2010-2022.
Question 23High Yield
A soccer player who sustained a twisting injury to the right ankle while making a cut is unable to bear weight and has diffuse tenderness over the anterior and lateral aspects of the ankle. Examination also shows a positive squeeze test. Plain radiographs and a stress radiograph are shown in Figures 26a through 26c. Radiographs of the leg and knee are normal. What is the most appropriate management?
Explanation
Explanation
26b 26c The mechanism of injury, physical examination, and radiographs indicate a "high" ankle sprain with disruption of the distal tibiofibular ligaments and interosseous membrane. These injuries typically involve pronation and external rotation forces. In addition, recovery is significantly delayed, often requiring 6 to 8 weeks to heal. Radiographs obtained months after recovery often show calcification within the distal syndesmosis, which is not typically symptomatic. This patient has gross instability, resulting in a high incidence of chronic diastasis and subluxation leading to impaired function. Treatment should consist of reduction and stabilization with a transsyndesmotic screw because this injury demonstrates a widened syndesmosis. Boytim MJ, Fisher DA, Neumann L: Syndesmotic ankle sprains. Am J Sports Med 1991;19:294-298.
References:
- Miller CD, Shelton WR, Barrett GR, et al: Deltoid and syndesmosis ligament injury of the ankle without fracture. Am J Sports Med 1995;23:746-750.
Question 24High Yield
An 18-year-old football player sustains a contact injury to his right lower leg, and radiographs show a closed transverse fracture of the middle third of the tibia. Based on the clinical examination, a compartment syndrome is suspected. When measuring compartment pressures, the highest tissue pressure is recorded how many centimeters proximal or distal to the fracture site?
Explanation
Explanation
Measurements of compartment pressures in patients with tibial fractures and compartment syndrome reveal that the highest tissue pressures are recorded at the level of the fracture or within 5 cm of the fracture. Tissue pressures show a statistically significant decrease when they are recorded at increasing distances proximal and distal to the site of the highest pressure recorded. To reliably determine the location of the highest tissue pressure in patients with tibial fractures, measurements should be obtained, at a minimum, in both the anterior and deep posterior compartments at the level of the fracture, as well as at locations proximal and distal. The highest tissue pressure recorded should serve as a basis for determining the need for fasciotomy. Heckman MM, Whitesides TE Jr, Grewe SR, Rooks MD: Compartment pressure in association with closed tibial fractures: The relationship between tissue pressure, compartment, and the distance from the site of the fracture. J Bone Joint Surg Am 1994;76:1285-1292.
References:
- Whitesides TE Jr, Heckman MM: Acute compartment syndrome: Update on diagnosis and treatment. J Am Acad Orthop Surg 1996;4:209-218.
Question 25High Yield
Which of the following is the preferred treatment for symptomatic localized pigmented villonodular synovitis (PVNS) of the knee?
Explanation
Explanation
Localized PVNS is a variant of the disease process where the synovial proliferation occurs in one area and usually presents as a discrete mass. It has been effectively treated with complete excision. This may be performed arthroscopically or with arthrotomy. Complete synovectomy and radiation therapy are unnecessary to eradicate the localized form of PVNS. Tyler WK, Vidal AF, Williams RJ, et al: Pigmented villonodular synovitis. J Am Acad Orthop Surg 2006;14:376-385.
References:
- Kim SJ, Shin SJ, Choi NH, et al: Arthroscopic treatment for localized pigmented villonodular synovitis of the knee. Clin Orthop Relat Res 2000;379:224-230.
Question 26High Yield
What term best describes the process involved when a growth factor produced by an osteoblast stimulates the differentiation of an adjacent undifferentiated mesenchymal cell during fracture repair?
Explanation
Explanation
Growth factors are proteins secreted by cells that can act on target cells to produce certain biologic actions. These actions can be described as autocrine, paracrine, and endocrine. Autocrine actions are those in which the growth factor influences an adjacent cell of its origin or identical phenotype. Paracrine actions are those in which the protein influences an adjacent cell that is different in its origin or phenotype. Endocrine actions are those in which the factor influences a cell located at a distant anatomic site. Lieberman J, Daluiski A, Einhorn TA: The role of growth factors in the repair of bone: Biology and clinical applications. J Bone Joint Surg Am 2002;84:1032-1044.
References:
- Zuscik MJ, Drissi MH, Reynolds PR, et al: Molecular and cell biology in orthopaedics, in Einhorn TA, O'Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 27High Yield
A patient with a below-the-knee amputation is being evaluated for a new prosthesis. He wants to improve his ability to walk on uneven surfaces. What modification to the prosthesis can be made to accommodate this request?
Explanation
Changing from a solid keel to a keel with a sagittal split allows an amputee to navigate uneven terrain more easily. Changing the length of the keel affects the responsiveness of the prosthesis but does not address the surface conditions for ambulation. The SACH is not used as frequently anymore, because overload problems to the nonamputated foot have been observed. Koval K (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 31-45.
Question 28High Yield
A 13-year-old girl is referred for a painful progressive valgus deformity of the right knee. Examination reveals an antalgic gait with an obvious valgus deformity. The right distal femur has a palpable, tender mass with erythema and warmth. Figures 4a and 4b show a clinical photograph and a radiograph. Management should consist of
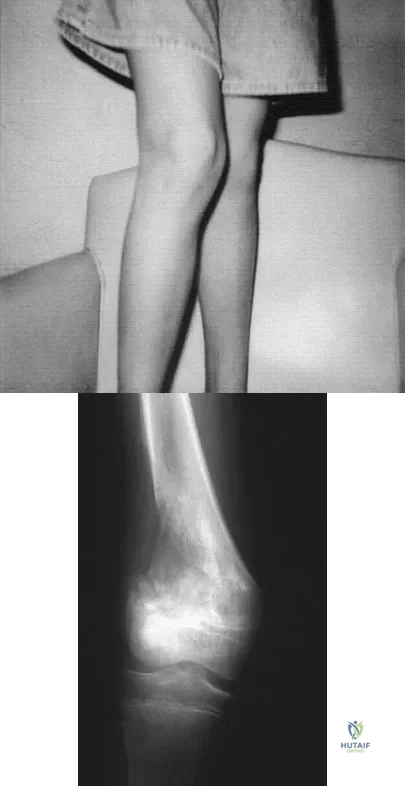
Explanation
The radiograph shows a pathologic fracture through a destructive lesion of the distal femur metaphysis with osteolytic and osteoblastic features. The lateral cortex is destroyed, and there is periosteal new bone formation. These findings are consistent with malignancy, most likely an osteogenic sarcoma. Patients with suspected malignant tumors are best managed by surgeons with specific expertise in orthopaedic oncology. The biopsy of a malignant lesion should be deferred to the surgeon who is capable of definitive management of the patient. Enneking W: Principles of musculoskeletal oncologic surgery, in Evarts C (ed): Surgery of the Musculoskeletal System. New York, NY, Churchill Livingston, 1990.
Question 29High Yield
What neurovascular structure is at greatest risk when creating a proximal anterolateral elbow arthroscopy portal?
Explanation
Explanation
The radial nerve is 4 to 7 mm from the anterolateral portal, which is placed 1 cm anterior and 3 cm proximal to the lateral epicondyle. The posterior interosseous nerve can lie 1 to 14 mm from the portal site. Andrews JR, Carson WG: Arthroscopy of the elbow. Arthroscopy 1985;1:97-107.
References:
- Lynch G, Meyers JF, Whipple TL, et al: Neurovascular anatomy and elbow arthroscopy: Inherent risks. Arthroscopy 1986;2:190-197.
Question 30High Yield
What neurologic structure is most at risk when performing intramedullary screw fixation of a fifth metatarsal base fracture?
Explanation
Explanation
The sural nerve and its terminal branches course through the lateral hindfoot and midfoot area and are directly at risk in surgeries involving the peroneal tendon complex and the fifth metatarsal. The first branch of the lateral plantar nerve originates in the tarsal tunnel region and courses across the plantar heel area to innervate the abductor digiti minimi; it is not at direct risk with fifth metatarsal surgery. The saphenous, superficial peroneal, and deep peroneal nerves are not at risk anatomically with a lateral midfoot incision. Donley BG, McCollum MJ, Murphy GA, Richardson EG: Risk of sural nerve injury with intramedullary screw fixation of fifth metatarsal fractures: A cadaver study. Foot Ankle Int 1999;20:182-184.
References:
- Lawrence SJ, Botte MJ: The sural nerve in the foot and ankle: An anatomic study with clinical and surgical implications. Foot Ankle Int 1994;15:490-494.
Question 31High Yield
A 58-year-old man has persistent pain and weakness of his right shoulder after undergoing primary rotator cuff repair 1 year ago. A clinical photograph is shown in Figure 11. Which of the following factors might make functional improvement problematic with revision rotator cuff surgery?
Explanation
Explanation
Functional improvement after revision rotator cuff surgery is most likely to occur in patients with an intact deltoid, good-quality rotator cuff tissue, preoperative active elevation alone to 90 degrees, and only one prior rotator cuff repair. In this patient, the compromised deltoid origin might make functional improvement less likely. Djurasovic M, Marra G, Arroyo JS, et al: Revision rotator cuff repair: Factors influencing results. J Bone Joint Surg Am 2001;83:1849-1855. Bigliani LU, Cordasco FA, McIlveen SJ, et al: Operative treatment of failed repairs of the rotator cuff. J Bone Joint Surg Am 1992;74:1505-1515.
References:
- Neviaser RJ, Neviaser TJ: Operation for failed rotator cuff repair: Analysis of fifty cases. J Shoulder Elbow Surg 1992;1:283-286.
Question 32High Yield
Which of the following radiographic views best depicts a Hill-Sachs defect?

Explanation
The Stryker notch view best shows this type of defect. An outlet view helps evaluate acromial shape, a true AP shows joint space narrowing, a serendipity view evaluates the sternoclavicular joint, and a Zanca view helps evaluate the acromioclavicular joint. An internal rotation AP may also depict a Hill-Sachs defect.
Question 33High Yield
A 14-year-old boy has a midshaft fibular lesion. Biopsy results are consistent with Ewing's sarcoma. Following induction chemotherapy, local control typically consists of
Explanation
Explanation
Current treatment regimens for Ewing's sarcoma typically involve induction chemotherapy followed by local control and further chemotherapy. Local control consists of surgery alone, radiation therapy alone, or a combination of the two. In bones that are easily resectable (or expendable) with wide margins, surgery alone is usually recommended. For areas that are unresectable (ie, large, bulky pelvic tumors), radiation therapy alone is sometimes the preferred method of local control. If surgery is chosen and margins are close, radiation therapy can be used as an adjuvant. Amputation rarely is required for an isolated fibular lesion. Observation without adequate local therapy results in local recurrence. Nesbit ME Jr, Gehan EA, Burgert EO Jr, et al: Multimodal therapy for the management of primary, nonmetastatic Ewing's sarcoma of bone: A long-term follow-up of the First Intergroup study. J Clin Oncol 1990;8:1664-1674.
References:
- Simon MA, Springfield DS, et al: Ewing's Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 287-297.
Question 34High Yield
Figures 32a and 32b show the radiographs of a 13-year-old right hand-dominant boy who sustained a closed Salter-Harris type II fracture of the proximal humerus during a hockey game. The shoulder has significant swelling, but is neurovascularly intact. What treatment offers the best chance of reestablishing normal shoulder motion?

Explanation
The patient has a significantly angulated proximal humerus fracture with a high degree of varus angulation, and rotational malalignment is likely. Failure to correct the varus angulation will result in permanent loss of shoulder abduction because the patient's age limits bony remodeling. These fractures are inherently unstable due to the inability to control the proximal fracture alignment. Shoulder spica casts have a high rate of redisplacement after treatment. Adequate open or closed reduction and pin fixation in the operating room optimizes alignment and all but eliminates the chance of redisplacement. Dobbs MB, Luhmann SJ, Gordon JE, et al: Severely displaced proximal humerus epiphyseal fractures. J Pediatr Orthop 2003;23:208-215. Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, p 701.
Question 35High Yield
Figure 30 shows the radiograph of a 38-year-old man who reports persistent pain laterally and plantarly about the fifth metatarsal head. Examination reveals calluses dorsolaterally and plantarly about the fifth metatarsal head. Nonsurgical management has failed to provide relief. Surgical treatment should include

Explanation
The patient has painful lateral and plantar keratoses with metatarsus quintus valgus deformity. This combination of problems is best addressed with an oblique mid-diaphyseal osteotomy that allows the distal metatarsal to be displaced medially and dorsally. Lateral eminence resection alone will not address the painful plantar keratosis. A distal chevron osteotomy has a more limited ability to address the plantar keratosis (if translated medially and slight dorsally). Proximal diaphyseal osteotomies of the fifth metatarsal are associated with an increased risk of delayed union or nonunion secondary to the relative hypovascularity in the proximal diaphysis. Excision of the fifth metatarsal head can result in a floppy fifth toe and transfer metatarsalgia. Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Question 36High Yield
A 12-year-old boy who has had a 1-month history of right thigh pain and a limp reports worsening of the pain after a fall, and he can no longer walk or bear weight on the involved extremity. Radiographs of the pelvis reveal a slipped capital femoral epiphysis with moderate to severe displacement. While positioning the patient on the fracture table for screw fixation, partial reduction of the slip is achieved. No further reduction maneuvers are attempted, and the epiphysis is stabilized with a single cannulated screw. What complication is most likely to develop following this procedure?
Explanation
Explanation
Traditional classification of slipped capital femoral epiphyses is based on the following temporal criteria: acute (symptoms that persist for less than 3 weeks); chronic (symptoms that persist for more than 3 weeks); or acute on chronic (acute exacerbation of long-standing symptoms). A newer classification differentiates between a stable slip where weight bearing is possible, and an unstable slip if it is not. Reduction of an unstable slip often occurs unintentionally with induction of anesthesia and positioning of the patient for surgery. The rate of satisfactory results is lower primarily because of a much higher incidence of osteonecrosis following internal fixation of an unstable slip. Loder RT, Richards BS, Shapiro PS, Reznick LR, Aronson DD: Acute slipped capital femoral epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140.
References:
- Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 151-159.
Question 37High Yield
Figures 56a through 56c show the radiograph, CT scan, and biopsy specimen of a 44-year-old man who underwent chemotherapy and radiation therapy for lymphoma of the distal femur 20 years ago. His current problem is most likely related to
Explanation
Explanation
56b 56c The patient has changes consistent with radiation therapy to the femur, including osteopenia and an aggressive appearing neoplasm. The tumor is most likely a radiation-induced sarcoma. This is more likely than recurrent lymphoma at this late date. It is not related to steroid use or a primary lung tumor. Mirra J (ed): Bone Tumors: Clinical, Radiologic and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, p 353.
References:
- Huvos A, Woodard H, Cahan W, et al: Postradiation osteogenic sarcoma of bone and soft tissue. A clinical pathologic study of 66 Patients. Cancer 1985;55:1244.
Question 38High Yield
Figure 39 shows the AP radiograph of a 62-year-old man with degenerative osteoarthritis secondary to trauma. History reveals that he underwent total elbow arthroplasty 3 years ago. He continues to report instability and constant pain. A complete work-up, including aspiration and cultures, is negative. Treatment should consist of removal of the components and

Explanation
An unconstrained prosthesis dislocation is a disconcerting problem that is not easily resolved; however, revision to a semiconstrained prosthesis would best achieve both pain relief and stability. Removal of the components and distraction arthroplasty or conversion to a resection arthroplasty are options, but the results would be unpredictable with regards to pain relief, postoperative motion, or elbow stability. Arthrodesis is poorly tolerated. With revision to another unconstrained prosthesis, there is the risk of continued redislocation because of chronic ligamentous insufficiency. Linscheid RL: Resurfacing elbow replacement arthroplasty: Rationale, technique and results, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 602-610.
Question 39High Yield
Polyethylene wear of the bearing surface has been recognized as a mode of failure in total knee arthroplasty; therefore, many patients are offered polyethylene exchange. In terms of success rates, this surgical procedure has been reported to have a
Explanation
Explanation
Engh and associates reported on the results of 63 knees (56 patients) following polyethylene exchange. The mean interval between exchange and the index total knee arthroplasty was 59 months. The mean follow-up after exchange was 7.4 years. Seven of 48 knees with adequate follow-up failed. Greater failure occurred if there was more severe wear before the exchange. Greater undersurface wear also resulted in a higher failure rate. Perioperative osteolysis or intraoperative observation of metallosis did not have an impact on the failure of polyethylene exchange. The risk of infection is no different from other total knee arthroplasty revisions. Wasielewski RC, Parks N, Williams I, et al: Tibial insert undersurface as a contributing source of polyethylene wear debris. Clin Orthop 1997;345:53-59.
References:
- Engh GA, Koralewicz LM, Pereles TR: Clinical results of modular polyethylene insert exchange with retention of total knee arthroplasty components. J Bone Joint Surg Am 2000;82:516-523.
Question 40High Yield
A 30-year-old firefighter sustained a longitudinal pulling injury to the arm while attempting to move a heavy object during a fire. Figure 45 shows an MRI scan of the elbow. Initial management should consist of
Explanation
Explanation
Because the MRI scan shows a complete rupture of the distal biceps tendon, the preferred treatment is anatomic repair of the tendon to the radial tuberosity either with the use of suture anchors or transosseous sutures through a two-incision technique. Several studies have documented superior results with anatomic repair of the distal biceps tendon when compared with results of nonsurgical management or repair of the tendon by attachment to the brachialis muscle. Patients undergoing anatomic repair of the distal biceps tendon through a two-incision technique typically regain a functional range of motion and nearly normal strength. D'Alessandro DF, Shields CL Jr, Tibone JE, Chandler RW: Repair of distal biceps tendon ruptures in athletes. Am J Sports Med 1993;21:114-119. Boyd JB, Anderson LD: A method for reinsertion of the distal biceps brachii tendon. J Bone Joint Surg Am 1961;43:1041-1043. Morrey BF, Askew LJ, An KN, Dobyns JH: Rupture of the distal tendon of the biceps brachii: A biomechanical study. J Bone Joint Surg Am 1985;67:418-421.
References:
- Failla JM, Amadio PC, Morrey BF, Beckenbaugh RD: Proximal radioulnar synostosis after repair of distal biceps brachii rupture by the two-incision technique: Report of four cases. Clin Orthop 1990;253:133-136.
Question 41High Yield
Figure 37 shows the radiograph of a 23-year-old football player who sustained a blow to the anterior aspect of his shoulder. Examination reveals pain and limited rotation. He is unable to flex the arm above the shoulder. Management should include which of the following studies?

Explanation
The patient has a posterior dislocation. The radiograph reveals marked internal rotation, but fails to show whether the humeral head is posteriorly displaced. Therefore, an axillary radiograph should be obtained to help confirm the diagnosis. Transverse view CT or MRI scans also may be useful. The other studies will not help confirm the diagnosis. In addition to a direct posterior blow, a shoulder dislocation may be caused by a seizure disorder or electrocution. Bloom MH, Obata WG: Diagnosis of posterior dislocation of the shoulder with the use of Velpeau axillary and angle-up roentgenographic views. J Bone Joint Surg Am 1967;49:943-949.
Question 42High Yield
A 16-year-old female swimmer reports several episodes of atraumatic glenohumeral instability that occur with different arm positions. Examination reveals generalized ligamentous laxity and a positive sulcus sign, and her shoulder can be subluxated both anteriorly and posteriorly. Initial management should consist of

Explanation
The patient has multidirectional instability (MDI). It has been reported that a high percentage of patients with MDI respond to a properly structured exercise program that is continued for at least 3 to 6 months. If nonsurgical management fails to provide relief, stabilization with an inferior capsular shift procedure has been effective in a high percentage of patients. Unidirectional repairs, such as the Putti-Platt procedure, are unsuitable for correcting MDI. Thermal capsulorrhaphy has been reported to have a very high failure rate (greater than 50%) for treating MDI. Burkhead WZ Jr, Rockwood CA Jr: Treatment of instability of the shoulder with an exercise program. J Bone Joint Surg Am 1992;74:890-896. Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908. Pollock RG, Owens JM, Flatow EL, et al: Operative results of the inferior capsular shift procedure for multidirectional instability of the shoulder. J Bone Joint Surg Am 2000;82:919-928.
Question 43High Yield
The postoperative neurologic prognosis of a patient who has a tumor that is compressing the spinal cord and causing a neurologic deficit depends primarily on the
Explanation
Explanation
The tumor biology, location, and pretreatment neurologic status are the best predictors of a patient's postoperative neurologic prognosis. Between 60% to 90% of patients who are ambulatory at the time of diagnosis will retain this ability after treatment. Location is important in that less space is available for the cord in the thoracic spine. Lesions located in vascular watershed regions may disrupt the vascular supply of the cord. Weinstein JN: Differential diagnosis and surgical treatment of primary benign and malignant neoplasms, in Frymoyer JW (ed): The Adult Spine: Principles and Practice. New York, NY, Raven Press, 1991, vol 1, pp 829-860.
References:
- Siegal T, Siegal T: Current considerations in the management of neoplastic spinal cord compression. Spine 1989;14:223-228.
Question 44High Yield
Figures 45a and 45b show the radiographs of a 14-year-old boy who sustained a distal radius fracture while playing hockey. After 1 year the patient is asymptomatic. Follow-up and comparison radiographs and an MRI scan are shown in Figures 45c and 45d. What is the next most appropriate step in management?
Explanation
The patient sustained a growth plate fracture of the distal radius and ulna. Although treated with closed reduction and casting, the follow-up radiographs demonstrate shortening of the radius in comparison to the ulna, and the MRI scan confirms thinning of the distal radius growth plate and bony bars consistent with a growth arrest. At this time, the discrepancy in length is too minor to consider lengthening of the radius; in addition, excision of a physeal bar with minimal growth potential is not likely to restore the gross discrepancy. Ulnar styloid fractures are rarely symptomatic and do not require treatment in the asymptomatic patient. Closure of the distal ulna growth plate will prevent further discrepancy between the radius and ulna. Vanheest A: Wrist deformities after fracture. Hand Clin 2006;22:113-120.
Question 45High Yield
A 24-year-old man who works at a local oyster and clam farm sustained a laceration on his hand at work. Examination reveals a cellulitic index finger without evidence of tenosynovitis. After appropriate irrigation and debridement, what antibiotic is most appropriate?
Explanation
Explanation
Injuries involving brackish water and shellfish can have devastating consequences caused by Vibrio vulnificus infections. Patients may have a severe invasive infection, with three main clinical features: primary septicemia, wound infection, and gastroenteritis. Antibiotic administration is crucial because mortality rates of up to 50% have been observed with Vibrio septicemia. The current recommendation is to give a third-generation cephalosporin such as ceftazadime. Chiang SR, Chuang YC: Vibrio vulnificus infection: Clinical manifestations, pathogenesis, and antimicrobial therapy. J Microbiol Immunol Infect 2003;36:81-88.
References:
- Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 240-259.
Question 46High Yield
A previously healthy 35-year-old man was involved in a rollover motor vehicle accident 2 days ago. He was placed in a semi-rigid cervical orthosis. He now reports mostly axial neck pain with attempted range of motion. Examination reveals the mechanical neck pain but no obvious neurologic deficits. AP, flexion, and extension radiographs are shown in Figures 10a through 10c, and sagittal and coronal CT scans are shown in Figures 10d and 10e. What is the most appropriate management at this time?

Explanation
Odontoid fractures can be classified based on the anatomic position of the fracture within the dens itself. Type I is an oblique fracture through the upper part of the odontoid process. Type II is a fracture that occurs at the base of the odontoid as it attaches to the body of C2; type III occurs when the fracture line extends through the body of the axis. Type 1 fractures typically can be treated nonsurgically with 6 to 8 weeks of immobilization with a semi-rigid cervical orthosis. Nondisplaced, deep type III fractures generally are treated with skeletal halo fixation. Deep, displaced, and angled type III fractures can be treated with closed reduction and skeletal halo fixation. Shallow type III fractures are sometimes amenable to anterior odontoid screw fixation. Type II fractures can be managed nonsurgically or surgically. Treatment options include halo immobilization, internal fixation (odontoid screw fixation), and posterior atlantoaxial arthrodesis. Management with the halo vest usually is considered if the initial dens displacement is less than 6 mm, the reduction is performed within 1 week of the injury and is able to be maintained, and the patient is younger than age 60 years. Halo vest immobilization can lead to a healing rate of more than 90%. Posterior surgical fusion techniques provide high fusion success rates but do so at the expense of cervical rotation. Up to 50% of rotation is lost with these techniques. Anterior odontoid single screw fixation is often tolerated better than skeletal halo fixation and also is noted to preserve the normal rotation at C1/C2. Studies have shown less of a malunion and nonunion rate in the treatment of type II odontoid fractures with anterior odontoid screw fixation. Osteoporosis, short neck and barrel-chested anatomy, and fractures that are more than 4 weeks old preclude anterior odontoid fixation. Shilpakar S, McLaughlin MR, Haid RW Jr, et al: Management of acute odontoid fractures: Operative techniques and complication avoidance. Neurosurg Focus 2000;8:e3. Subach BR, Morone MA, Haid RW Jr, et al: Management of acute odontoid fractures with single-screw anterior fixation. Neurosurgery 1999;45:812-819.
Question 47High Yield
Six weeks after onset, what is the most clearly accepted indication for surgical management for lumbar disk herniation?
Explanation
Explanation
In the absence of a cauda equina syndrome or progressive weakness, the best indication for surgical management is refractory radicular pain. Surgical decision-making should not be based on the size of the herniation. Large extruded herniations tend to resolve more predictably than smaller herniations. Stable motor weakness and numbness resolve similarly in both surgical and nonsurgical management, although surgery hastens the process. When intractable radicular pain is the strict indication for surgery, surgical intervention provides substantial and more rapid pain relief than nonsurgical care. Rhee JM, Schaufele M, Abdu WA: Radiculopathy and the herniated lumbar disc: Controversies regarding pathophysiology and management. J Bone Joint Surg Am 2006;88:2070-2080.
Question 48High Yield
A 7-year-old boy has had chronic left leg pain that is worse at night but is not activity related. Use of nonsteroidal anti-inflammatory drugs for the past 6 months has failed to provide relief. A CBC count with differential, erythrocyte sedimentation rate, and C-reactive protein are within normal limits. Radiographs and a CT scan are shown in Figures 31a through 31c. Management should consist of
Explanation
Explanation
31b 31c Osteoid osteomas are painful bone lesions, with radiographs revealing a dense sclerotic cortex surrounding a small radiolucency or nidus. Symptoms often are worse at night but usually are not activity related. While treatment in the past has consisted of open en bloc excision, current means of removal include percutaneous drilling under CT guidance and percutaneous radiofrequency coagulation. Success rates of percutaneous treatment are comparable to those seen following open procedures. The characteristic radiographic appearance of this lesion usually obviates the need for biopsy. Because the lesion is not caused by pyogenic organisms, antibiotics are not indicated. Donahue F, Ahmad A, Mnaymneh W, Pevsner NH: Osteoid osteoma: Computed tomography guided percutaneous excision. Clin Orthop 1999;366:191-196.
References:
- Rosenthal DI, Hornicek FJ, Wolfe MW, et al: Percutaneous radiofrequency coagulation of osteoid osteoma compared with operative treatment. J Bone Joint Surg Am 1998;80:815-821.
Question 49High Yield
What is the recommended insertion torque for halo pins in adults?

Explanation
Garfin and associates have shown that halo pins inserted with 8 in-lb of insertion torque results in significantly less loosening with cyclical loading than pins inserted with 6 in-lb of torque. Moreover, Botte and associates reported that 8 in-lb of torque is clinically safe and effective in lowering the incidence of pin loosening and infection. Botte MJ, Byrne TP, Garfin SR: Application of the halo device for immobilization of the cervical spine utilizing an increased torque pressure. J Bone Joint Surg Am 1987;69:750-752. Garfin SR, Lee TO, Roux RD, et al: Structural behavior of the halo orthosis pin-bone interface: Biomechanical evaluation of standard and newly designed stainless steel halo fixation pins. Spine 1986;11:977-981.
Question 50High Yield
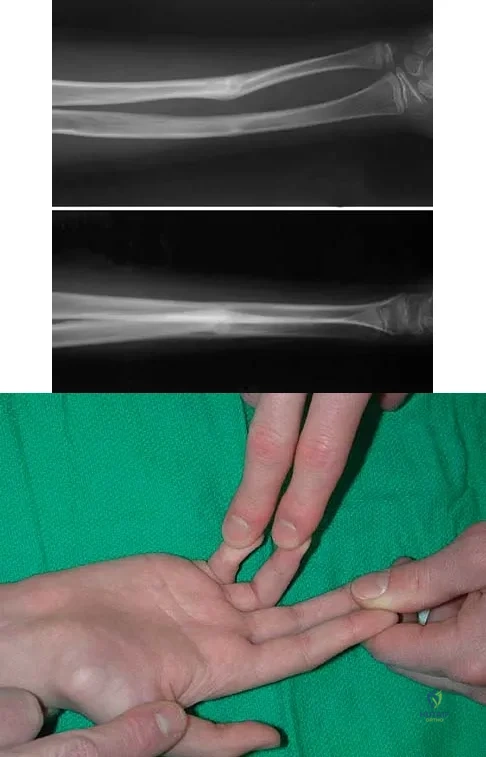
A 12-year-old boy sustained a both bone forearm fracture 10 weeks ago and underwent closed reduction and casting. Examination now reveals that the injury is healed, but he is unable to extend his little and ring fingers of the injured hand with his wrist extended. Full extension is possible with the wrist flexed. A radiograph and clinical photograph are shown in Figures 15a and 15b. The remainder of his hand and wrist examination and neurologic evaluation in the hand are normal. What is the most likely diagnosis?
Explanation
In this patient, examination reveals an inability to extend the fingers with the wrist extended, but full extension is possible with wrist flexion. These findings demonstrate isolated tenodesis of the flexor digitorum to the ring and little fingers. These findings are not consistent with compartment syndrome or nerve injury. Scarring or entrapment of tendons in forearm fractures can occur. Watson PA, Blair W: Entrapment of the index flexor digitorum profundus tendon after fracture of both forearm bones in a child. Iowa Orthop J 1999;19:127-128. Shaw BA, Murphy KM: Flexor tendon entrapment in ulnar shaft fractures. Clin Orthop 1996;330:181-184. Kolkman KA, van Niekerk JL, Rieu PN, et al: A complicated forearm greenstick fracture: Case report. J Trauma 1992;32:116-117.
Question 51High Yield
Figure 33 shows the AP and lateral radiographs of an obese 58-year-old man who underwent a cementless total hip arthroplasty 6 years ago. He reports no pain, and examination reveals a normal gait and painless hip range of motion. What is the most likely diagnosis?
Explanation
Osteolysis of an otherwise well-functioning total hip arthroplasty is a recognized complication, and its radiographic appearance is typical, as shown here. Distal osteolysis, such as that shown here, is more prevalent when there is noncircumferential sealing of the proximal femoral canal. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 175-180.
Question 52High Yield
The force generated by a muscle is most highly dependent on its
Explanation
Explanation
The cross-sectional area of a muscle determines to a great extent the force generated by the muscle. The force of a muscle contraction is controlled by the amount of myofibrils that contract; the greater the amount of contracting myofibrils, the greater the force of contraction. Fiber types have less to do with the force of contraction and more to do with the duration and speed of contraction. Muscle length affects contraction force through the Blix curve. The morphology of a muscle can affect the cross-sectional area by varying the angle of the fibers in relation to the force vector. Conditioning mostly affects duration and fatigability. Buckwalter JA, Mow VC, Ratcliffe A: Restoration of injured or degenerated articular cartilage. J Am Acad Orthop Surg 1994;2:192-201.
References:
- Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 683-716.
Question 53High Yield
A 35-year-old man reports forefoot pain with weight-bearing activities. He reports that he has had high arches since adolescence but has never been treated. Examination reveals stiff cavus feet. He has no plantar callus or hammer toe formation. The ankle can be passively dorsiflexed 10 degrees. Initial management should consist of
Explanation
Explanation
The patient has cavus feet with minimal clinical symptoms. At this stage, conservative management is preferred. The use of a molded orthosis will allow better support of the midfoot and provide cushioning of the forefoot. This will most likely result in long-term relief. In more advanced cases with forefoot callus formation, Achilles tendon lengthening or calcaneal osteotomy and Steindler stripping are effective in correcting the cavus deformity. In the presence of arthritic changes in the hindfoot, a triple arthrodesis with corrective bone resection may be necessary. Janisse DJ: Indications and prescriptions for orthoses in sports. Orthop Clin North Am 1994;25:95-107.
References:
- Franco AH: Pes cavus and pes planus: Analyses and treatment. Phys Ther 1987;67:688-694.
Question 54High Yield
A 35-year-old man sustained a 10% compression fracture of the C5 vertebra in a diving accident. Radiographs show good alignment, and examination reveals no neurologic compromise. An MRI scan reveals no significant soft-tissue disruption posteriorly. Management should consist of
Explanation
Explanation
The patient has a stable flexion-compression injury of the cervical spine. The fracture occurs as a result of compression failure of the vertebral body. If the force continues, a tension failure of the posterior structures occurs, leading to potential dislocation. Immobilization in a rigid cervical orthosis will allow this fracture to heal. Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 457-464.
References:
- Allen GL, Ferguson RL, Lehmann TR, O'Brien RP: A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine 1982;7:1-27.
Question 55High Yield
A 32-year-old man has a closed oblique displaced fracture at the junction of the lower and middle third of the humeral shaft and a complete radial nerve palsy. Closed reduction is performed and is felt to be acceptable. Management of the radial nerve palsy should consist of
Explanation
Explanation
In patients who have radial nerve dysfunction associated with a closed humeral fracture, nerve function usually will return to normal without surgical exploration. If clinical findings or electromyographic studies show no improvement at 3 months, surgical exploration and repair can be performed. Tendon transfers are performed if nerve repair is deemed unsuccessful. Pollock FH, Drake D, Bovill EG, et al: Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am 1981;63:239-243.
References:
- Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 237-247.
Question 56High Yield
What is the most common cause for poor outcomes in patients who undergo total shoulder arthroplasty?

Explanation
In an article in the Journal of Shoulder and Elbow, 431 total shoulder arthroplasties were performed with a cemented all-polyethylene glenoid component between 1990 and 2000. Follow-up averaged 4.2 years. In total, 53 surgical complications occurred in 53 patients (12%). Of these, 32 were major complications (7.4%), with 17 of these requiring reoperation. Index complications in order of frequency included rotator cuff tearing, postoperative glenohumeral instability, and periprosthetic humeral fracture. Notably, glenoid and humeral component loosening requiring reoperation occurred in only one shoulder. Data from the contemporary patient group suggest that there are fewer complications of shoulder arthroplasty and less need for reoperation. Especially striking is the near absence of component revision because of loosening or other mechanical factors. Complications involving the brachial plexus have been reported following total shoulder arthroplasty but are not as common of a cause for failure. Chin PY, Sperling JW, Cofield RH, et al: Complications of total shoulder arthroplasty: Are they fewer or different? J Shoulder Elbow Surg 2006;15:19-22.
Question 57High Yield
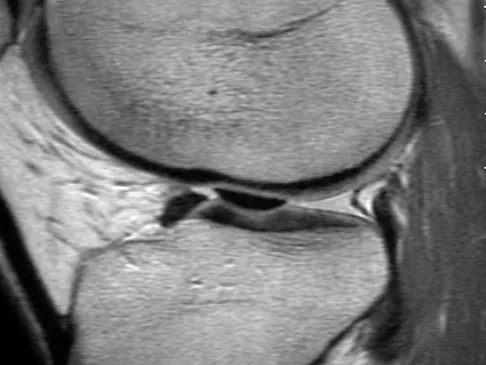
A 21-year-old soccer player reports pain and is unable to straighten his knee following an acute injury during a game. He is unable to continue to play. An MRI scan is shown in Figure 3. What is the next most appropriate step in management?
Explanation
The patient has a locked knee that cannot be fully extended. This is most likely the result of the mechanical block of a bucket-handle tear that has flipped into the notch. Also, the pain may be so severe that the muscle spasm prevents the knee from straightening out. When the patient is anesthetized, the muscle spasm relaxes and the meniscus can be reduced out of the notch. Arthroscopy is the treatment of choice. A meniscal repair is usually possible in large bucket-handle tears because the meniscus is torn in the red-red zone where most of the vascular supply is located. If the handle portion is badly frayed or damaged, a partial meniscectomy should be performed. The classic finding on MRI is a "double PCL sign." This is due to the flipped portion of the meniscus in the notch. Critchley IJ, Bracey DJ: The acutely locked knee: Is manipulation worthwhile? Injury 1985;16:281-283.
Question 58High Yield
The pathophysiology of a claw toe deformity includes muscular imbalance caused by which of the following relatively strong structures?

Explanation
The dynamic forces acting to maintain the position of the proximal phalanx at the head of the metatarsal are a balance between the extensor digitorum longus and the weaker intrinsic muscles. With hyperextension at the metatarsophalangeal joint, the intrinsic muscles become less efficient as plantar flexors. Consequently, the hyperextension deformity progresses in the metatarsophalangeal joint as the opposition of the intrinsic muscles to the extensor tendon lessens. This is in contrast to the situation in the interphalangeal joints, where the stronger flexors overpower the weaker intrinsic muscles, which act as the extensors. This combination of events leads to hyperextension at the metatarsophalangeal joint and flexion deformities at the interphalangeal joints, resulting in claw toe. Mizel MS, Yodlowski ML: Disorders of the lesser metatarsophalangeal Joints. J Am Acad Orthop Surg 1995;3:166-173.
Question 59High Yield
What is the most common foot deformity associated with myelomeningocele?
Explanation
Explanation
All of the above can be associated with myelomeningocele, but talipes equinovarus occurs in 50% to 90% of patients with myelomeningocele. Congenital vertical talus is rarely associated with any neuromuscular diseases other than myelomeningocele but is not the most common deformity in myelomeningocele. Stans AA, Kehl DK: The pediatric foot, in Baratz ME, Watson AD, Imbriglia JE (eds): Orthopaedic Surgery: The Essentials. New York, NY, Thieme, 1999, pp 702-703.
References:
- Lindseth RE: Myelomeningocele, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott, Williams & Wilkins, 2001, pp 622-628.
Question 60High Yield
What assay most directly assesses gene expression at the posttranslational level?
Explanation
Explanation
Gene expression at the posttranslational level refers to proteins, as opposed to DNA or RNA. The only assay above that targets protein expression directly is the Western blot. Standard PCR is amplification of targeted DNA segments, regardless of whether or not they are actively expressed. Real-time PCR, Northern blot, and microarray expression profile analysis all quantify RNA as a means to determine posttranscriptional gene expression. Brinker MR: Cellular and molecular biology, immunology, and genetics in orthopaedics, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 81-94.
References:
- Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 19-76.
Question 61High Yield
Which of the following imaging modalities is most accurate in locating a toothpick in the plantar arch of the foot?

Explanation
Ultrasound is best at imaging abrupt changes in the density of adjacent tissue and therefore is best at imaging wood in the soft tissues of the foot. Mizel MS, Steinmetz ND, Trepman E: Detection of wooden foreign bodies in muscle tissue: Experimental comparison of computed tomography, magnetic resonance imaging, and ultrasonography. Foot Ankle Int 1994;15:437-443.
Question 62High Yield
A 12-year-old child with spina bifida paraplegia requires brace management for ankle stability. Which of the following principles applies to brace management in this individual?
Explanation
Explanation
Bracing for spina bifida paraplegia provides both support and improved function of the movable limb. An orthosis has value in controlling unstable joints. The three-point pressure effect applies a force above and below the joint to prevent it from buckling. A four-point pressure effect is only required for a two-joint system (this patient has problems only at the ankle). A longer lever arm brace and a brace with a greater area of support provide better stability. Finally, a straighter limb, without contracture, applies less pressure to the brace and lessens overload to the skin. Gage JR: An overview of normal walking. Instr Course Lect 1990;39:291-303. Bleck EE: Current concepts review: Management of the lower extremities in children who have cerebral palsy. J Bone Joint Surg Am 1990;72:140-144.
References:
- Harris MB, Banta JV: Cost of skin care in the myelomeningocele population. J Pediatr Orthop 1990;10:355:361.
Question 63High Yield
An 80-year-old man has had increasing shoulder pain for the past 4 months. He reports that it began with soreness and stiffness after chopping some wood. A coronal MRI scan is shown in Figure 16. Initial management should consist of

Explanation
The MRI scan shows a massive tear of the supraspinatus tendon with medial retraction to the level of the glenoid. This is most likely an attritional tear with a high risk of failure of the repair. The preferred treatment is nonsurgical management for pain and stiffness. Acromioplasty and coracoacromial ligament release in this setting are controversial, as they can result in the devastating complication of anterosuperior subluxation of the humerus. Rockwood CA Jr, Williams GR Jr, Burkhead WZ Jr: Debridement of degenerative, irreparable lesions of the rotator cuff. J Bone Joint Surg Am 1995;77:857-866.
Question 64High Yield
Based on the radiographic findings shown in Figure 41, which of the following wrist ligaments is most likely disrupted?

Explanation
The radiograph shows a diastasis of the scapholunate interval, caused by certain failure of the scapholunate interosseous ligament. The lunotriquetral interosseous ligament stabilizes the lunotriquetral joint. The long radiolunate ligament originates in the volar radius and inserts in the lunate. The short radiolunate ligament originates on the ulnar margin of the radius and inserts on the ulnar margin of the lunate. The ulnolunate ligament originates at the ulnar styloid base and inserts on the volar aspect of the lunate. Linscheid RL, Dobyns JH, Beabout JW, et al: Traumatic instability of the wrist: Diagnosis, classification, and pathomechanics. J Bone Joint Surg Am 1972;54:1612-1632. Mayfield JK, Johnson RP, Kilcoyne RK: Carpal dislocations: Pathomechanics and progressive perilunar instability. J Hand Surg Am 1980;5:226-241.
Question 65High Yield
Figures 54a and 54b show the radiograph and MRI scan of a 7-year-old boy who has a painful right thoracic scoliosis that measures 35 degrees. Neurologic examination is normal. Management should consist of

Explanation
Because hydrosyringomyelia, with or without an Arnold-Chiari malformation, is now being recognized as the etiology of many infantile and juvenile idiopathic scolioses, management should consist of a neurosurgical consultation. Observation with follow-up radiographs is not an option in curves of this magnitude. A technitium Tc 99m bone scan is unnecessary because the etiology of the curve has been identified. Although spinal fusion may be needed in the future, it should not be undertaken before the neurosurgical problem has been addressed. Zadeh HG, Sakka SA, Powell MP, Mehta MH: Absent superficial abdominal reflexes in children with scoliosis: An early indicator of syringomyelia. J Bone Joint Surg Br 1995;77:762-767. Schwend RM, Hennrikus W, Hall JE, Emans JB: Childhood scoliosis: Clinical indications for magnetic resonance imaging. J Bone Joint Surg Am 1995;77:46-53.
Question 66High Yield
What is the most common complication of using structural bulk allograft to reconstruct segmental defects of the acetabulum?
Explanation
Both autograft and allograft have been used for complex acetabular reconstructions. They have been shown to be successful in the short term. However, graft resorption with collapse and subsequent cup loosening have occurred at high rates for both types of grafts, especially if reinforcement rings or cages are not used. Jasty M, Harris WH: Salvage total hip reconstruction in patients with major acetabular bone deficiency using structural femoral head allografts. J Bone Joint Surg Br 1990;72:63-67. Paprosky WG, Magnus RE: Principles of bone grafting in revision total hip arthroplasty: Acetabular technique. Clin Orthop 1994;298:147-155.
Question 67High Yield
During the evaluation of a patient suspected of having a lumbar disk herniation, T1- and T2-weighted MRI scans reveal a hyperintence lobular, well-defined lesion in the L2 vertebral body. What is the most likely diagnosis?

Explanation
The findings are characteristic of hemangioma. When the hemangioma is large enough, vertical striations may be visible on plain radiographs. Axial CT scans commonly reveal a speckled appearance. Metastatic lesions are typically hypointense on T1-weighted images because they replace the fatty marrow. Bony islands, like cortical bone, are dark on T1- and T2-weighted images. Intravertebral disk herniation would have characteristics similar to the disk and be in continuity with the disk. Osteoporosis is more diffuse. Ross JS, Masaryk TJ, Modic MT, Carter JR, Mapstone T, Dengel FH: Vertebral hemangiomas: MR imaging. Radiology 1987;165:165-169.
Question 68High Yield
What is the most commonly reported complication following elbow arthroscopy?
Explanation
Explanation
The complication rate following elbow arthroscopy is reported at 5%. The most commonly reported complication is transient neurapraxia, with nerve transection remaining an unfortunate and rare event. While infection remains the most common serious complication, it is uncommon (0.8%). Synovial cutaneous fistula and compartment syndrome, while reported, are the least frequent complications of elbow arthroscopy. Kelly EW, Morrey BF, O'Driscoll SW: Complications of elbow arthroscopy. J Bone Joint Surg Am 2001;83:25-34.
References:
- Morrey BF: Elbow complication, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 519-522.
Question 69High Yield
A 15-year-old boy falls from his bicycle and sustains an injury to his elbow. Prereduction radiographs are shown in Figure 12a. Closed reduction is performed without difficulty and postreduction radiographs are shown in Figure 12b. What is the next most appropriate step in treatment?

Explanation
Elbow dislocations in children are rare injuries and usually result from a fall on an outstretched arm. The incidence of these injuries increases as patients age and concurrently the incidence of supracondylar humerus fractures decreases. In adolescent patients, simple elbow dislocations are treated with splint immobilization and the initiation of physical therapy once comfortable. The practitioner must be aware of structures that may get caught in the joint on reduction. These include the median nerve as well as the medial epicondyle. In this patient, the radiographs reveal a medial epicondyle fracture. Postreduction radiographs show the joint to be incongruous secondary to intra-articular displacement. At this point, the most appropriate treatment is to perform an open reduction and repair of the medial epicondyle fragment. Rasool MN: Dislocations of the elbow in children. J Bone Joint Surg Br 2004;86:1050-1058.
Question 70High Yield
A 28-year-old female firefighter fell from the top of a three-story building in the line of duty. She sustained a displaced pelvic fracture with more than 5 mm displacement. Compared to normal healthy controls, these patients have a higher incidence of
Explanation
Explanation
Pelvic trauma in women has been shown to increase the risk of sexual dysfunction and dyspareunia. Additionally, caesarean section childbirth is almost universal following pelvic trauma regardless of whether anterior pelvic hardware is present or not. Copeland CE, Bosse MJ, McCarthy ML et al: Effect of trauma and pelvic fracture on female genitourinary, sexual, and reproductive function. J Orthop Trauma 1997;11:73-81.
Question 71High Yield
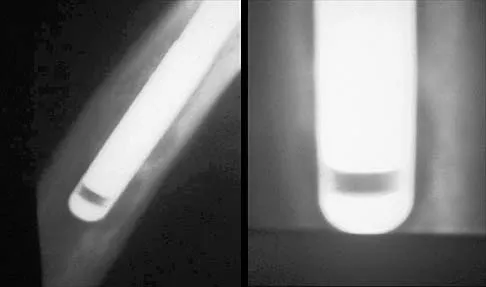
A 13-year-old girl sustained an isolated midshaft left femoral fracture in a motor vehicle accident. The fracture was treated with a rigid, antegrade intramedullary nail placed through the piriformis fossa. The fracture healed uneventfully, as shown in Figure 46a; however, at 12 months postoperatively she now reports left hip pain. A current AP radiograph and MRI scan are shown in Figures 46b and 46c. What complication occurred in this patient?
Explanation
Explanation
46b 46c The development of femoral head ischemic necrosis is the iatrogenically created complication in this skeletally immature patient. Placement of a rigid, antegrade intramedullary nail through the piriformis fossa is likely to damage the vascular supply to the femoral head as the vessels ascend the femoral neck on the way to the femoral head. The MRI scan reveals ischemic necrosis with early collapse of the femoral head. The joint space is preserved on the MRI scan, ruling out chondrolysis. Letts M, Jarvis J, Lawton L, et al: Complications of rigid intramedullary rodding of femoral shaft fractures in children. J Trauma 2002;52:504-516. Buckley SL: Current trends in the treatment of femoral shaft fractures in children and adolescents. Clin Orthop Relat Res 1997;338:60-73.
Question 72High Yield
A 21-year-old college student fell from a balcony and landed on his outstretched right hand. He is seen in the emergency department 4 hours later and reports wrist pain and diffuse hand numbness. The volar forearm compartment is soft and there is no pain with passive finger extension. Radiographs are shown in Figures 25a and 25b. Definitive treatment should consist of
Explanation
Explanation
25b A spectrum of perilunate injury patterns exists, with the dorsal trans-scaphoid perilunate fracture-dislocation being the most common. Perilunate injuries are highly unstable complex carpal disruptions that are not amenable to closed treatment. Open reduction and internal fixation is necessary to accurately restore carpal alignment via fracture reduction and fixation and intercarpal ligament repair. Controversy exists regarding the need for dorsal or combined dorsal and volar approaches. Based on the radiographic findings of a volar dislocation of the lunate and the associated median nerve injury, the patient requires open reduction and internal fixation via combined dorsal and volar approaches with a concomitant carpal tunnel release. Herzberg G, Forissier D: Acute dorsal trans-scaphoid perilunate fracture-dislocations: Medium-term results. J Hand Surg Br 2002;27:498-502. Melone CP Jr, Murphy MS, Raskin KB: Perilunate injuries: Repair by dual dorsal and volar approaches. Hand Clin 2000;16:439-448.
Question 73High Yield
A 25-year-old man sustained an L1 compression fracture in a fall from his roof. He is neurologically intact and has no other injuries. Radiographs reveal a 25% loss of height anteriorly and 5 degrees of kyphosis at the fracture site. A CT scan reveals no compromise of the posterior column. Management should consist of
Explanation
The patient has a stable fracture that can be initially treated with bed rest, followed by bracing and quick mobilization. The outcome is good and surgery is not required. These fractures can be treated nonsurgically if there is less than 50% compression, 15 degrees of angulation, and intact posterior structures. Cantor JB, Lebwohl NH, Garvey T, Eismont FJ: Nonoperative management of stable thoracolumbar burst fractures with early ambulation and bracing. Spine 1993;18:971-976.
Question 74High Yield
A 15-year-old girl reports a 6-month history of activity-related knee pain and swelling. A radiograph, MRI scan, and biopsy specimen are shown in Figures 21a through 21c. What is the most likely diagnosis?
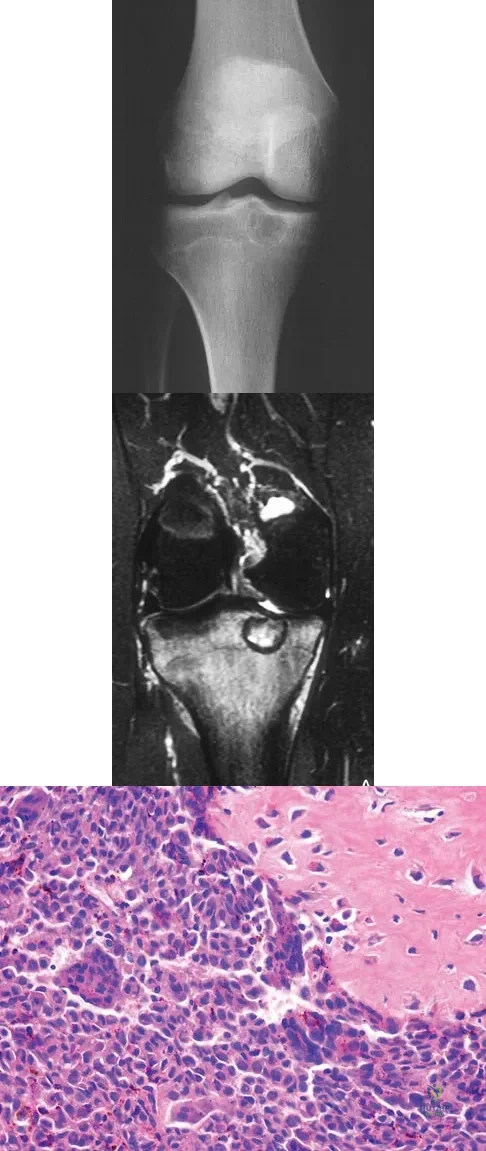
Explanation
The epiphyseal location on the radiograph and MRI scan and the histologic findings of polyhedral cells separated by a chondroid matrix with pericellular, lattice-like "chicken wire" calcification all suggest chondroblastoma. Although giant cell tumors of bone typically occupy an epiphyseal location, they are rare in children and when present are often metaphyseal in skeletally immature patients. Enchondromas and osteoblastomas are generally metaphyseal and, along with giant cell tumors, have very different histology than seen here. Chondromyxoid fibromas are typically metaphyseal in location. Huvos AG: Bone Tumors: Diagnosis, Treatment, and Prognosis. Philadelphia, PA, WB Saunders, 1991, pp 295-313.
Question 75High Yield
A 35-year-old woman has had significant pain and swelling in the left medial ankle inferior to the medial malleolus for the past 8 months. Physical therapy, brace and orthotic management, and immobilization have failed to provide relief. She is now requesting a more aggressive option to assist in pain relief. Clinical photographs and radiographs are seen in Figures 42a through 42f. Following exposure, a complete rupture of the posterior tibial tendon is visible. What is the most appropriate surgical reconstruction?
Explanation
Explanation
42b 42c 42d 42e 42f The patient has a complete rupture of the posterior tibial tendon with minimal hindfoot valgus deformity. The deformity is supple, and there is no arthritis in the subtalar, talonavicular, or calcaneocuboid joints; therefore, joint-sparing procedures are appropriate in this patient (avoidance of arthrodeses). The treatment of choice is flexor digitorum longus tendon transfer, medial slide calcaneal osteotomy, and spring ligament repair. Primary repair of an incompetent posterior tibial tendon can lead to failure and recurrence of pain and deformity. Talonavicular arthrodesis corrects the forefoot abduction and elevates a plantar flexed talus; however, the patient does not have this deformity; therefore, the procedure is not indicated. Myerson MS, Corrigan J, Thompson F, et al: Tendon transfer combined with calcaneal osteotomy for treatment of posterior tibial tendon insufficiency: A radiological investigation. Foot Ankle Int 1995;16:712-718. Trnka HJ, Easley ME, Myerson MS: The role of calcaneal osteotomies for correction of adult flat foot. Clin Orthop 1999;365:50-64. Jahss MH: Spontaneous rupture of the tibialis posterior tendon: Clinical findings, tenographic studies, and a new technique for repair. Foot Ankle 1982;3:158-166.
References:
- Toolan BC, Sangeorzan BJ, Hansen ST Jr: Complex reconstruction for the treatment of dorsolateral peritalar subluxation of the foot. J Bone Joint Surg Am 1999;81:1545-1560.
Question 76High Yield
An 8-year-old boy sustains injuries to his head, abdomen, and left lower extremity after being struck by a truck. In the emergency department, his mental status deteriorates and he is intubated after assessment reveals a Glasgow Coma Scale score of 3; the score subsequently improves to 10. A CT scan reveals a right parietal intracranial hemorrhage, and an abdominal ultrasound reveals free fluid. Prior to an emergency laparotomy, the swollen left thigh is evaluated. Radiographs reveal a transverse fracture of the mid-diaphysis. Management of the fracture should consist of

Explanation
The prognosis for a young patient with a head injury is more favorable compared to that for adults. Full neurologic recovery generally occurs. Spasticity may occur within a few days after injury, which can lead to fracture displacement if immediate spica casting or traction is used. Early surgical stabilization will reduce problems with shortening and malunion and will facilitate transportation of the child for diagnostic tests. Surgery may be performed when it is best for the patient, either on the day of injury or later if time is needed for stabilization. In this patient, the fracture is ideally suited to stabilization using flexible intramedullary nails. Heinrich and associates' report of 78 diaphyseal femur fractures stabilized with flexible intramedullary nails included 14 patients with an associated closed head injury. All fractures healed, and there were no major complications. Tolo VT: Management of the multiply injured child, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 83-95.
Question 77High Yield
A 40-year-old right hand-dominant construction worker has had a 6-month history of aching left shoulder pain that is worse after working a long day. Examination reveals limited range of motion and good strength when compared to his asymptomatic right arm. He has not had any orthopaedic intervention to date. Radiographs are shown in Figures 43a and 43b. What is the most appropriate treatment?

Explanation
The patient is a young laborer with osteoarthritis. Initial treatment should begin with nonsurgical management that may include anti-inflammatory drugs, cortisone injections, and physical therapy to diminish pain and improve motion. The other choices may eventually be necessary but should only follow a course of nonsurgical management. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 257-266.
Question 78High Yield
A 52-year-old woman who is right hand-dominant sustains an injury to her elbow in a fall. A radiograph is shown in Figure 60. The preferred treatment of this injury pattern should include

Explanation
The patient has a Bado type 2 variant Monteggia fracture with a radial head fracture. The type 2 variant is associated with a higher nonunion rate and poorer outcomes compared to other Bado-type Monteggia fractures. While it is potentially acceptable to repair the radial head, factors such as higher degrees of comminution and older age lead toward replacement as the treatment of choice. Plate and screw fixation is favored over Kirschner wire/tension band fixation because this is not a simple olecranon fracture. Plate placement in a type 2 fracture is dorsal to counteract very high tensile forces associated with fixation failure. Egol KA, Tejwani NC, Bazzi J, et al: Does a Monteggia variant lesion result in a poor functional outcome? A retrospective study. Clin Orthop Relat Res 2005;438:233-238. Jupiter JB, Leibovic SJ, Ribbans W, et al: The posterior Monteggia lesion. J Orthop Trauma 1991;5:395-402.
Question 79High Yield
A 28-year-old man has had a 2-year history of progressive lateral ankle pain. History reveals that he underwent a triple arthrodesis at age 13 for a tarsal coalition. The pain has been refractory to braces, custom inserts, and nonsteroidal anti-inflammatory drugs. Weight-bearing radiographs of the ankle and foot are shown in Figures 3a through 3d. Surgical management should include which of the following?

Explanation
The patient has a valgus-supination triple arthrodesis malunion. Weight-bearing radiographs show excessive residual valgus through the subtalar joint, producing lateral subfibular impingement, and residual forefoot abduction and midfoot supination through the talonavicular joint, lateralizing the weight-bearing forces through the foot. The deformity is best managed with a medial displacement calcaneal osteotomy and transverse tarsal derotational osteotomy. Ankle arthroscopy and lateral ligament reconstruction are indicated in the event of ligament instability. Tendon transfer, lateral column lengthening, and heel cord lengthening are used for treatment of adult flatfoot from posterior tibial tendon insufficiency. Ankle arthrodesis and ankle arthroplasty are not indicated in this patient because the lateral ankle symptoms are the result of the underlying deformity in the hindfoot, the patient is young, and the ankle joint is relatively normal. Haddad SL, Myerson MS, Pell RF IV: Clinical and radiographic outcome of revision surgery for failed triple arthrodesis. Foot Ankle Int 1997;18:489-499.
Question 80High Yield
A 39-year-old man reports low back pain, lower extremity numbness, and urinary retention after being injured in a motor vehicle accident 1 day ago. He is able to walk but is in pain. A straight leg raise results in increased back pain, and examination reveals that perianal sensation is decreased. Placement of a urinary catheter results in 500 mL of urine. What is the next most appropriate step in management?
Explanation
Explanation
Acute cauda equina syndrome, including saddle hypesthesia and bowel/bladder incontinence, is a red flag that demands emergent evaluation with MRI and urgent surgery if compression is confirmed. Results appear to be improved if surgery is performed within 48 hours. The other treatment approaches listed are not indicated if a cauda equina syndrome is present. Ahn UM, Ahn NU, Buchowski JM, et al: Cauda equina syndrome secondary to lumbar disc herniation: A meta-analysis of surgical outcomes. Spine 2000;25:1515-1522. Shapiro S: Medical realities of cauda equina syndrome secondary to lumbar disc herniation. Spine 2000;25:348-351.
References:
- Kostuik JP, Harrington I, Alexander D, et al: Cauda equina syndrome and lumbar disc herniation. J Bone Joint Surg Am 1986;68:386-391.
Question 81High Yield
A 22-month-old girl has cerebral palsy. Which of the following findings is a good prognostic indicator of the child's ability to walk in the future?
Explanation
For the parachute test, the examiner holds the child prone and then lowers the child rapidly toward the floor. The parachute reaction is normal or positive if the child reaches toward the floor. The Moro or startle reflex should not be present beyond age 6 months. Asymmetric tonic neck reflex, extensor thrust, and absent foot placement are abnormal findings at any age. Bleck EE: Orthopaedic Management in Cerebral Palsy. Lavenham, Suffolk, The Lavenham Press, 1987, pp 121-139.
Question 82High Yield
A 42-year-old man has had left lower extremity pain in an L5 radicular pattern for the past 6 weeks. He denies significant axial low back pain. History reveals that he underwent an L4-5 diskectomy with successful relief of similar pain 5 years ago. Which of the following imaging studies would offer the greatest amount of information?
Explanation
MRI with gadolinium will best identify recurrent herniated nucleus pulposus or other root compression and distinguish scar from recurrent disk. CT is unable to distinguish scar from recurrent disk density, and the addition of myelogram dye can reveal compromise of the thecal sac but cannot distinguish the scar from recurrent disk as the source of compression. Although lateral flexion-extension radiographs may be important to rule out any instability, much of that information can be inferred from the associated disk and adjacent bony changes on MRI. Bone scan techniques may identify subtle stress fractures resulting from previous aggressive facet resection, but low back pain also would be expected. Mirowitz SA, Shady KL: Gadopentetate dimeglumine-enhanced MR imaging of the postoperative lumbar spine: Comparison of fat-suppressed and conventional T1-weighted images. Am J Roentgenol 1992;159:385-389.
Question 83High Yield
The Coleman block test is used to evaluate the cavovarus foot. What is the most important information obtained from this test?
Explanation
Coleman block testing, performed by placing an elevation under the lateral border of the foot, is used to determine if the forefoot and/or plantar flexed first ray is causing a compensatory varus in the hindfoot. The block is placed under the lateral border of the foot, and therefore does not have any relation to the Achilles tendon and suppleness of the hindfoot. Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Question 84High Yield
Figures 35a through 35c show the clinical photograph and radiographs of a 15-year-old boy who stubbed his toe 1 day ago while walking barefoot in the yard. Management should consist of
Explanation
Explanation
35b 35c The patient has an open fracture of the physis of the distal phalanx with a portion of the nail bed interposed in the physis. Seymour initially described this injury in the distal phalanges of fingers. Optimal treatment consists of removing the interposed tissue, irrigating the fracture, and a short course of antibiotics. The nail should be preserved to provide stability. Kensinger DR, Guille JT, Horn BD, et al: The stubbed great toe: Importance of early recognition and treatment of open fractures of the distal phalanx. J Pediatr Orthop 2001;21:31-34. Pinckney LE, Currarino G, Kennedy LA: The stubbed great toe: A cause of occult compound fracture and infection. Radiology 1981;138:375-377.
References:
- Seymour N: Juxta-epiphysial fracture of the terminal phalanx of the finger. J Bone Joint Surg Br 1966;48:347-349.
Question 85High Yield
Compared to postoperative radiation therapy, preoperative radiation therapy has a higher rate of what complication?
Explanation
Explanation
Radiation therapy is commonly used as an adjuvant in the treatment of soft-tissue sarcomas, but a controversy exists whether it should be preoperative or postoperative. Radiation therapy can be given prior to or following resection of the tumor. Postoperative radiation is usually given in a higher dose to a larger treatment field. This commonly results in a higher incidence of fibrosis and lymphedema. There is no statistical difference in local recurrence rate between the two radiation treatment plans. Neuropathy is more commonly a complication of chemotherapy. Preoperative radiation therapy has been shown to have a higher wound complication rate than postoperative radiation. Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 197-215.
References:
- Davis AM, O'Sullivan B, Turcotte R, et al: Late radiation morbidity following randomization to preoperative versus postoperative radiotherapy in extremity soft tissue sarcoma. Radiother Oncol 2005;75:48-53.
Question 86High Yield
Figures 5a and 5b show the radiographs of an active 52-year-old man who has increasing knee pain and progressive varus deformity after undergoing total knee arthroplasty 7 years ago. Examination reveals a small effusion, but he has good motion and stability. What is the most likely diagnosis?

Explanation
The radiographs show narrowing of the medial joint space, which indicates polyethylene wear and progressive varus alignment. Wear particles incite osteolytic lesions like the one seen on the lateral radiograph. O'Rourke MR, Callaghan JJ, Goetz DG, et al: Osteolysis associated with a cemented modular posterior-cruciate-substituting total knee design. J Bone Joint Surg Am 2002;84:1362-1371.
Question 87High Yield
A 23-year-old man reports pain on the superior aspect of his right shoulder with repetitive overhead activities and when lying on his right side. Figure 29 shows an axial MRI scan. What is the most likely diagnosis based on the MRI findings?
Explanation
Explanation
Os acromiale represents a failure of fusion of the anterior acromial apophysis and has been reported in approximately 8% of the population. Patients with a symptomatic os acromiale often report impingement-type symptoms with pain over the superior acromion, especially with overhead activities or sleeping. When nonsurgical management is unsuccessful, surgical options include excision, open reduction and internal fixation, and arthroscopic decompression. Kurtz CA, Humble BJ, Rodosky MW, et al: Symptomatic os acromiale. J Am Acad Orthop Surg 2006;14:12-19.
References:
- Ortiguera CJ, Buss DD: Surgical management of the symptomatic os acromiale. J Shoulder Elbow Surg 2002;11:521-528.
Question 88High Yield
An axillary nerve lesion may cause weakness in the deltoid and the
Explanation
While the most prominent functional deficit from axillary nerve lesions occurs from denervation of the deltoid, denervation of the teres minor also occurs.
Question 89High Yield
A 28-year-old anesthesia resident has aching pain in his dominant right forearm after injuring it while playing basketball 1 week ago. He reports that he is unable to perform regional anesthesia that requires manipulation of a needle. Examination reveals that he is unable to flex the interphalangeal joint of the thumb, and flexion of the distal interphalangeal joint of the index finger is weak. Management should consist of
Explanation
Explanation
The patient has anterior interosseous nerve palsy. Initial management should consist of splinting followed by observation; surgical decompression may be required if there is no improvement in the functional deficit in 6 months. Anterior interosseous nerve palsy is classically described as an inability to flex the interphalangeal joint of the thumb because of flexor pollicis longus paralysis and a weakness or inability to flex the distal interphalangeal joint of the index finger because of weakness and/or paralysis of the flexor digitorum profundus to the index finger. There has been some controversy in the literature as to whether this represents a true peripheral compression neuropathy or neuritis. Recent recommendations have been to extend the period of observation from 3 to 6 months before surgical decompression, as most cases will resolve within 6 months. Miller-Breslow A, Terrono A, Millender LH: Nonoperative treatment of anterior interosseous nerve paralysis. J Hand Surg Am 1990;15:493-496.
References:
- Stern PJ, Fassler PR: Anterior interosseous nerve compression syndrome, in Gelberman RH (ed): Operative Nerve Repair and Reconstruction. Philadelphia, PA, 1991, vol 2, pp 983-1002.
Question 90High Yield
Lumbar instability may be surgically induced by
Explanation
In cadaveric studies, unilateral facetectomy, or excision of 50% or more of both facets, significantly decreases the biomechanic integrity of the motion segment and may increase the risk of iatrogenic instability. Sacrifice of the spinous process, interspinous ligaments, and ligamentum flavum weakens the motion segment but does not increase the risk for instability. Facetectomy, even unilateral, predisposes the patient toward lumbar instability.
Question 91High Yield
A 13-year-old boy hyperextends his knee while playing basketball and reports a pop that is followed by a rapid effusion. A lateral radiograph is shown in Figure 4. Initial management consists of attempted reduction with extension, with no change in position of the fragment. What is the next most appropriate step in management?
Explanation
Explanation
Avulsion fractures of the tibial spine are rare injuries that result from rapid deceleration or hyperextension of the knee in skeletally immature individuals. This injury is the equivalent of ruptures of the anterior cruciate ligament in adults. These fractures are classified as types 1 through 3. Type 1 is a minimally displaced fracture, type 2 fractures have an intact posterior hinge, and type 3 fractures have complete separation. The radiograph demonstrates a completely displaced, or type III, tibial spine avulsion. Surgical reduction is indicated in type 2 fractures that fail to reduce with knee extension and in all type 3 fractures. Reduction may be arthroscopic or open, with fixation of the bony fragment using a method that maintains physeal integrity and prevents later growth arrest. Preferred techniques would be with suture or an intra-epiphyseal screw Wiley JJ, Baxter MP: Tibial spine fractures in children. Clin Orthop 1990;255:54-60. Mulhall KJ, Dowdall J, Grannell M, et al: Tibial spine fractures: An analysis of outcome in surgically treated type III injuries. Injury 1999;30:289-292. Owens BD, Crane GK, Plante T, et al: Treatment of type III tibial intercondylar eminence fractures in skeletally immature athletes. Am J Orthop 2003;32:103-105.
References:
- Vocke AK, Vocke AR: Cartilaginous avulsion fracture of the tibial spine. Orthopedics 2002;25:1293-1294.
Question 92High Yield
Which of the following assessment tools most accurately reflects outcomes of well-being, daily function, and general health in a patient treated for cervical myelopathy?
Explanation
Explanation
The short-form 36 is an excellent tool for measuring the patient's perception of treatment outcome because it is a patient-generated, validated assessment of physical, social, and role function, emotional and mental health, energy/fatigue, pain, health perception, and health change. The Nurick criteria is an evaluation of physical function with gradations of ambulation and daily function. The Japanese Orthopaedic Association score gives points for function in activities of daily living but does not assess perception of general health. The neck disability index assesses the impact of neck pain on daily life, and the Odom criteria are the surgeon's evaluations of degree of radicular pain and deficit. Albert TJ, Mesa JJ, Eng K, McIntosh TC, Balderston RA: Health outcome assessment before and after lumbar laminectomy for radiculopathy. Spine 1996;21:960-963. Swiontkowski MF, Buckwalter JA, Keller RB, Haralson R: The outcomes movement in orthopaedic surgery: Where we are and where we should go. J Bone Joint Surgery Am 1999;81:732-740.
References:
- Ludwig SC, Albert TJ: Measuring outcomes in cervical myelopathy and radiculopathy. Instr Course Lect 1999;48:417-421.
Question 93High Yield
A 35-year-old man has numbness and tingling in the index, middle, and ring fingers. History reveals that he also has had vague wrist pain and stiffness since being injured in a motorcycle accident 1 year ago. Radiographs are shown in Figures 47a through 47c. Management should consist of

Explanation
The patient has a chronic unrecognized volar lunate dislocation. Median nerve compression is the result of the lunate displaced into the carpal tunnel. The diagnosis can be made by radiographs; MRI is not necessary. A volar approach allows median nerve decompression with excision of the lunate, whereas a dorsal approach facilitates excision of the scaphoid and triquetrum. Rettig ME, Raskin KB: Long-term assessment of proximal row carpectomy for chronic perilunate dislocations. J Hand Surg Am 1999;24:1231-1236.
Question 94High Yield
In a patient who has undergone fusion with instrumentation from T4 to the sacrum for adult scoliosis, at which site is a pseudarthrosis most likely to be discovered?
Explanation
Although pseudarthrosis can be found anywhere within the spine that has been fused using long multisegmental fixation to the sacrum, it most commonly occurs at the lumbosacral junction. The thoracolumbar junction is another common site of potential pseudarthrosis. In this location, the anatomy changes from lumbar transverse processes to thoracic through the transition zone, and overlying instrumentation often makes it difficult to obtain enough sound bone on decorticated bone to achieve a successful fusion. Saer EH III, Winter RB, Lonstein JE: Long scoliosis fusion to the sacrum in adults with nonparalytic scoliosis: An improved method. Spine 1990;15;650-653. Kostuik JP, Hall BB: Spinal fusions to the sacrum in adults with scoliosis. Spine 1983;8:489-500.
Question 95High Yield
A 25-year-old man underwent a Putti-Platt repair for recurrent anterior dislocation of his right shoulder 9 months ago. He reports no further episodes of instability but continues to have severely restricted motion, with external rotation limited to less than 0 degrees with the arm at the side. He has pain at the ends of range of motion and restricted activities of daily living despite undergoing nearly 9 months of physical therapy. Radiographs of the shoulder show no arthritic changes. Management should now consist of
Explanation
Open release allows lengthening of the shortened subscapularis and is preferred when there are extra-articular contractures. Arthroscopic release, combined with the use of an interscalene catheter postoperatively, is an excellent treatment for capsular contractures but is contraindicated after procedures that result in extracapsular shortening (ie, Magnuson-Stack, Putti-Platt). Additional physical therapy or manipulation under anesthesia is not likely to be helpful. Shoulder hemiarthroplasty is contraindicated with normal articular surfaces, but prosthetic arthroplasty is sometimes necessary for arthritis associated with instability or overly tight instability repairs. Harryman DT II, Matsen FA III, Sidles JA: Arthroscopic management of refractory shoulder stiffness. Arthroscopy 1997;13:133-147. Warner JJ: Frozen shoulder: Diagnosis and management. J Am Acad Orthop Surg 1997;5:130-140. Warner JJ, Allen AA, Marks PH, Wong P: Arthroscopic release of postoperative capsular contracture of the shoulder. J Bone Joint Surg Am 1997;79:1151-1158.
Question 96High Yield
What is the treatment of choice for the injury shown in Figures 20a through 20c?
Explanation
Explanation
20b 20c The radiographs show multiple carpometacarpal dislocations. Reduction is often obtainable but difficult to maintain. Internal fixation is required to maintain the reduction, preferably with Kirschner wires. Closed reduction and percutaneous pinning is preferred by some surgeons. Others recommend open reduction to remove irreconstructable osteochondral fragments from the individual joints and to ensure correct reduction of the carpometacarpal joints. Kirschner wires are removed at 6 to 8 weeks. Prokuski LJ, Eglseder WA Jr: Concurrent dorsal dislocations and fracture-dislocations of the index, long, ring, and small (second to fifth) carpometacarpal joints. J Orthop Trauma 2001;15:549-554.
References:
- Lawlis JF III, Gunther SF: Carpometacarpal dislocations: Long-term follow-up. J Bone Joint Surg Am 1991;73:52-59.
Question 97High Yield
An otherwise healthy 45-year-old man has a 3-cm subcutaneous mass on his anterior thigh that is presumed to be a lipoma. Removal of the mass is performed in the office of his primary care physician. Pathologic evaluation shows a high-grade malignant fibrous histiocytoma. Staging reveals no evidence of metastatic disease. Management at this time should consist of
Explanation
Explanation
Resection of a previously excised soft-tissue sarcoma is recommended. Reoperation is recommended after removal of malignant tumors previously believed to be benign, as approximately one half of the patients will have residual tumor in the re-excised specimen. Observation is not indicated in most patients because local recurrence is likely. Radiation therapy alone may result in long-term local control but is felt to be less effective than reoperation. Chemotherapy and radiation therapy alone are not recommended. Wide excision is the most important factor for local disease control. Radiation therapy after surgical re-excision may also decrease the risk of local recurrence. Peabody TD, Monson D, Montag A, Schell MJ, Finn H, Simon MA: A comparison of the prognoses for deep and subcutaneous sarcomas of the extremities. J Bone Joint Surg Am 1994;76:1167-1173. Giuliano AE, Eilber FR: The rationale for planned reoperation after unplanned total excision of soft-tissue sarcomas. J Clin Oncol 1985;3:1344-1348. Lewis JJ, Leung D, Espat J, Woodruff JM, Brennan MF: Effect of resection in extremity soft tissue sarcoma. Ann Surg 2000;231:655-663.
References:
- Noria S, Davis A, Kardel R, et al: Residual disease following unplanned excision of soft-tissue sarcoma of an extremity. J Bone Joint Surg Am 1996;78:650-655.
Question 98High Yield
A 40 year-old-man was involved in a motor vehicle accident and sustained the pelvic injury seen in Figures 24a and 24b. Definitive management of the injury should consist of reduction by
Explanation
Explanation
24b The radiograph reveals disruption of the symphysis pubis and a displaced left sacral fracture. A posterior injury with displacement of greater than 1 cm is unstable, and a sacral fracture is particularly unstable. Surgical stabilization is required for these unstable anterior and posterior injuries. External fixation provides little stability to an unstable posterior pelvic injury. Reduction and internal fixation of the symphysis pubis and sacral fracture will provide the most stable pelvis with the least resultant deformity and allow patient mobilization. Tile M: Management of pelvic ring injuries, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 168-202.
References:
- Kabak S, Halici M, Tuncel M, et al: Functional outcome of open reduction and internal fixation for completely unstable pelvic ring fractures (type C): A report of 40 cases. J Orthop Trauma 2003;17:555-562.
Question 99High Yield
Figure 10 shows the AP radiograph of an ambulatory 76-year-old patient. What is the most appropriate surgical treatment option for this patient?

Explanation
The patient has a periprosthetic fracture around a loose cemented femoral component. The proximal bone stock is poor; therefore, this fracture may be categorized as Vancouver 3-B. Hip arthrodesis and resection arthroplasty provide suboptimal results, particularly for ambulatory patients. Although impaction allografting may be an option to restore the bone stock in a younger patient, the latter procedure will be very difficult to perform when the proximal bone is poor in quality and fractured. Cementing another component into this wide femur is not an option. The best option for revision of the femoral component in this elderly patient is proximal femoral replacement arthroplasty. Malkani AL, Settecerri JJ, Sim FH, et al: Long-term results of proximal femoral replacement for non-neoplastic disorders. J Bone Joint Surg Br 1995;77:351-356.
Question 100High Yield
A 25-year-old man reports wrist pain following a motorcycle accident. Examination reveals minimal swelling, slightly limited active range of motion, and point tenderness in the snuff box region. AP and oblique radiographs are shown in Figures 40a and 40b. Management should consist of
Explanation
Explanation
40b The radiographs reveal a scaphoid fracture with displacement and comminution and an unstable fracture pattern. Treatment should consist of open reduction and internal fixation. In displaced scaphoid fractures and fractures with unstable fracture patterns, closed reduction is ineffective and is likely to lead to nonunion. Limited intercarpal fusion and proximal row carpectomy are used to correct a variety of traumatic and posttraumatic problems of the wrist. Amadio PC, Taleisnik J: Fractures of the carpal bone, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 809-823. Rettig ME, Kozin SH, Cooney WP: Open reduction and internal fixation of acute displaced scaphoid waist fractures. J Hand Surg Am 2001;26:271-276. Cooney WP, Dobyns JH, Linscheid RL: Fractures of the scaphoid: A rational approach to management. Clin Orthop 1980;149:90-97.
References:
- Szabo RM, Manske D: Displaced fractures of the scaphoid. Clin Orthop 1988;230:30-38.
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding closed-reduction-casting-and-traction-are-three-common-treatment-methods-for-fractures