Trauma 2009 Practice Questions: Set 3 (Solved)

Key Takeaway
Your ultimate guide to Trauma 2009 Practice Questions: Set 3 (Solved) starts here. Access high-yield Trauma questions for the 2009 board exam. This module (Set 3) covers critical topics including surgical techniques, pathology, and treatment protocols with verified answers.
Trauma 2009 Practice Questions: Set 3 (Solved)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 42-year-old college professor reports persistent pain at the hypothenar eminence 9 months after falling from his bicycle. Initial radiographs were reportedly normal. Use of a wrist splint for the last 2 months has failed to provide relief. A radiograph obtained by his primary care physician prior to referral is seen in Figure 31. What is the most appropriate treatment?

Explanation
Question 2
Figures 32a and 32b show the radiographs of a 13-year-old right hand-dominant boy who sustained a closed Salter-Harris type II fracture of the proximal humerus during a hockey game. The shoulder has significant swelling, but is neurovascularly intact. What treatment offers the best chance of reestablishing normal shoulder motion?

Explanation
Question 3
What letter in Figure 33 marks the correct starting point for a transiliac pelvic screw?

Explanation
Question 4
A 57-year-old man involved in a motor vehicle accident sustains an injury to his right shoulder. A spot AP radiograph is shown in Figure 34. What is the next most appropriate step in the orthopaedic management of this patient?

Explanation
Question 5
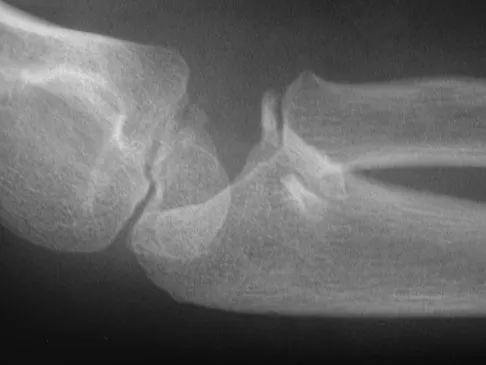
An 8-year-old girl injures her elbow playing soccer. After attempted reduction in the emergency department, radiographs of the elbow are shown in Figures 35a through 35c. What is the next most appropriate step in treatment?

Explanation
Question 6
A 30-year-old woman injured the ring finger of her nondominant hand while playing baseball 5 weeks ago. She now reports pain and limited motion of the proximal interphalangeal (PIP) joint. A lateral fluoroscopy image is shown in Figure 36. Treatment of the PIP joint should consist of

Explanation
Question 7
A 19-year-old woman fell onto her nondominant hand 6 weeks ago. Radiographs are shown in Figures 37a and 37b. A decision has been made to treat this fracture surgically. What is the best approach to treat this fracture?

Explanation
Question 8
Which of the following findings best describes the acetabular fracture shown in Figure 38?

Explanation
Question 9
In the setting of a proximal tibial plateau fracture and its repair, which of the following materials is an isotropic material?

Explanation
Question 10
A 28-year-old female firefighter fell from the top of a three-story building in the line of duty. She sustained a displaced pelvic fracture with more than 5 mm displacement. Compared to normal healthy controls, these patients have a higher incidence of

Explanation
Question 11
A 30-year-old man falls off a 7-foot ladder and sustains the injury seen in the radiograph and the CT scan shown in Figures 39a and 39b. Medical history is negative. Management of this injury should include which of the following?

Explanation
Question 12
A 24-year-old woman fell from a horse and landed on her outstretched right arm. Radiographs reveal an elbow dislocation with a type II coronoid fracture and a nonreconstructable comminuted radial head fracture. What is the most appropriate management?

Explanation
Question 13
A 30-year-old man is brought to the emergency department after a motor vehicle accident. He has a closed midshaft femoral fracture and an intra-abdominal injury. He is currently in the operating room and the exploration of his abdomen has been completed. His initial blood pressure was 70/30 mm Hg and is now 90/50 mm Hg after 4 liters of fluid and 2 units of blood. His initial serum lactate was 3.0 mmol/L (normal < 2.5), 1 hour postinjury it was 3.5 mmol/L, and it is now 5 mmol/L. His core temperature is 93 degrees F (34 degrees C). What is the most appropriate management for the femoral shaft fracture at this point?

Explanation
Question 14
A 45-year-old male karate instructor sustained the injury shown in Figures 40a through 40c while practicing karate. The decision to proceed with surgery depends on which of the following factors?

Explanation
Question 15
A 100-lb 9-year-old boy has a closed midshaft transverse femoral fracture. The oblique fracture is shortened by 3 cm with a 10-degree varus angulation. Surgical management consists of intramedullary, retrograde flexible titanium nailing. To optimize fracture stability, the surgeon should
Explanation
Question 16
A 16-year-old girl was involved in a motorcycle accident that resulted in a significant right tibial fracture with soft-tissue loss over the distal 4 cm of the anterior medial tibia. The patient has had two irrigations and debridements and recently had an intramedullary nail placed for the skeletal injury. Vacuum-assisted closure (VAC) has been used to cover the defect since the injury. The risk of infection developing in the tibia is
Explanation
Question 17
A 12-year-old boy falls from a bicycle. A radiograph of his injured shoulder is shown in Figure 41. What is the optimal method of treatment?

Explanation
Question 18
The major benefit of irrigation with a castile soap solution over irrigation with bacitracin solution for the treatment of the open fracture shown in Figure 42 can be seen in which of the following outcomes?

Explanation
Question 19
A 22-year-old cheerleader who fell from the top of a pyramid now reports anterior and posterior pelvic pain. A radiograph and CT scans are shown in Figures 43a through 43c. What is the best treatment for this injury?

Explanation
Question 20
What vessel is marked with an asterisk in Figure 44?

Explanation
Question 21
Figures 45a and 45b show the radiographs of a 14-year-old boy who sustained a distal radius fracture while playing hockey. After 1 year the patient is asymptomatic. Follow-up and comparison radiographs and an MRI scan are shown in Figures 45c and 45d. What is the next most appropriate step in management?

Explanation
Question 22
A 13-year-old girl sustained an isolated midshaft left femoral fracture in a motor vehicle accident. The fracture was treated with a rigid, antegrade intramedullary nail placed through the piriformis fossa. The fracture healed uneventfully, as shown in Figure 46a; however, at 12 months postoperatively she now reports left hip pain. A current AP radiograph and MRI scan are shown in Figures 46b and 46c. What complication occurred in this patient?
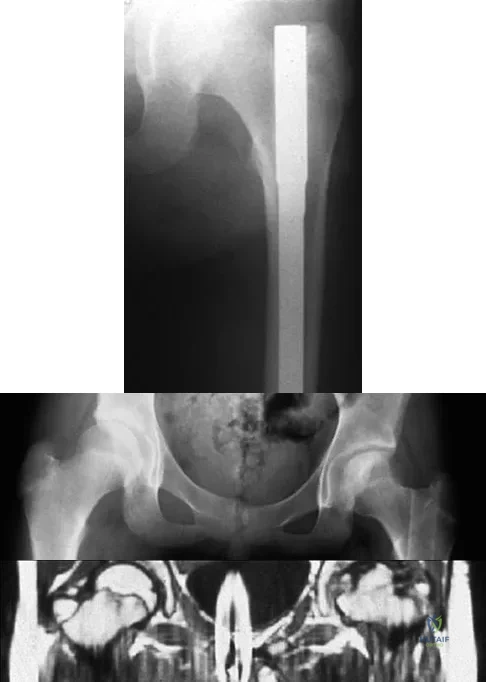
Explanation
Question 23
A 30-year-old man caught his dominant little finger on the straps of his windsurfing board 10 days ago. He reports swelling about the distal phalanx and has difficulty completely extending the distal interphalangeal joint. A radiograph is shown in Figure 47. What is the most appropriate treatment for this injury?
Explanation
Question 24
A 40-year-old man sustains a fracture-dislocation of C4-5. Examination reveals no motor or sensory function below the C5 level. All extremities are areflexic. The bulbocavernosus reflex is absent. The prognosis for this patient's neurologic recovery can be best determined by
Explanation
Question 25
Figures 48a and 48b show the radiographs of a 26-year-old woman who fell down two steps and twisted her foot and ankle. What is the most appropriate treatment for this injury?

Explanation
Question 26
A 35-year-old man is brought to the emergency department after a motorcycle collision. He is hemodynamically unstable, and a pelvic binder is ordered. Which of the following landmarks is the most appropriate location to center the pelvic binder?
Explanation
Question 27
A 28-year-old man sustains a closed spiral fracture of the tibial shaft. On examination, he is extremely anxious and requires increasing doses of opioid analgesia. Which of the following is the most sensitive early clinical finding of acute compartment syndrome?
Explanation
Question 28
A 65-year-old woman falls on her outstretched dominant hand and sustains a distal radius fracture. Closed reduction is performed in the emergency department. Which of the following post-reduction radiographic parameters falls outside the acceptable criteria for nonoperative management in an active adult?
Explanation
Question 29
A 6-year-old boy sustains a completely displaced extension-type supracondylar humerus fracture. On examination, the hand is pink and warm, with brisk capillary refill, but the radial pulse is not palpable. What is the most appropriate next step in management?
Explanation
Question 30
A 30-year-old man sustains a displaced, Pauwels type III (highly vertical) femoral neck fracture after a fall from a height. What is the most appropriate surgical strategy to optimize biomechanical stability for this specific fracture pattern?
Explanation
Question 31
A 45-year-old man sustains a Grade IIIB open tibia fracture from a farming accident involving heavy soil contamination. In addition to emergent surgical debridement, which of the following prophylactic antibiotic regimens is most appropriate?
Explanation
Question 32
A 22-year-old male athlete falls on his outstretched hand and sustains a scaphoid fracture. Which of the following fracture characteristics is associated with the highest risk of nonunion and avascular necrosis?
Explanation
Question 33
A 25-year-old unrestrained driver is involved in a head-on motor vehicle collision. He presents to the trauma bay with a shortened, internally rotated, and adducted left lower extremity. A radiograph confirms a posterior hip dislocation. Which of the following nerve injuries is most commonly associated with this injury?
Explanation
Question 34
A 32-year-old male sustains a twisting injury to his midfoot while playing soccer. He has swelling, plantar ecchymosis, and tenderness over the tarsometatarsal joints. Weight-bearing radiographs demonstrate a 3 mm diastasis between the base of the first and second metatarsals. What is the most appropriate definitive management?
Explanation
Question 35
A 28-year-old man falls from a height and sustains a Hawkins Type III fracture of the talar neck. Which of the following best describes the anatomical displacement associated with this injury?
Explanation
Question 36
A 42-year-old man sustains a severe closed tibial shaft fracture. He undergoes reamed intramedullary nailing. Which of the following intraoperative techniques is most effective in minimizing the elevation of intramedullary pressure and subsequent risk of fat embolism?
Explanation
Question 37
A 26-year-old male presents with an isolated, closed, displaced transverse fracture of the femoral shaft following a motorcycle collision. He is hemodynamically stable. Antegrade intramedullary nailing is planned. What is the most critical intraoperative factor in preventing a nonunion?
Explanation
Question 38
A 35-year-old man sustains a displaced Hawkins type III talar neck fracture. Which of the following surgical strategies provides the best biomechanical stability and allows for optimal visualization of the reduction?
Explanation
Question 39
A 68-year-old woman with a history of severe osteoporosis is treated with a locking plate for a 3-part proximal humerus fracture. Four weeks postoperatively, radiographs demonstrate varus collapse of the humeral head and screw cutout. Which of the following technical errors during the index procedure is most likely responsible for this complication?
Explanation
Question 40
A 25-year-old man arrives at the trauma center hemodynamically unstable with an anteroposterior compression type III (APC-III) pelvic ring injury. A pelvic binder is applied, and he receives massive transfusion protocol. His FAST exam is negative, but he remains hypotensive. What is the most likely anatomic source of his ongoing pelvic hemorrhage?
Explanation
Question 41
A 22-year-old male sustains a pelvic fracture in a motor vehicle accident. The AP pelvic radiograph demonstrates disruption of both the iliopectineal and ilioischial lines on the right side. The obturator ring is intact. Which of the following Judet-Letournel classifications best describes this fracture pattern?
Explanation
Question 42
The Sanders classification is utilized for preoperative planning in calcaneus fractures. Which of the following imaging modalities and views is essential for applying this classification system?
Explanation
Question 43
A 55-year-old woman sustains a highly comminuted intra-articular distal radius fracture. She undergoes open reduction and internal fixation with a volar locking plate. To minimize her risk of developing post-traumatic radiocarpal arthrosis, which of the following radiographic parameters is most critical to accurately restore?
Explanation
Question 44
A 38-year-old male falls from a ladder and sustains an isolated, closed, displaced midshaft clavicle fracture. Which of the following is considered an absolute indication for operative fixation?
Explanation
Question 45
A 40-year-old man sustains an extra-articular distal third tibia fracture. Intramedullary nailing is planned. To prevent the most common malalignment associated with this specific fracture pattern during nailing, which of the following techniques should be primarily employed?
Explanation
Question 46
A 25-year-old male sustains a purely ligamentous Lisfranc injury after a twisting mechanism while playing football. Which of the following fixation constructs has been shown to provide the best long-term clinical outcomes for this specific injury pattern?
Explanation
Question 47
A 45-year-old female presents with a closed, displaced intra-articular calcaneus fracture (Sanders Type III). The surgeon is considering an extensile lateral approach for open reduction and internal fixation. Which of the following is considered an absolute contraindication to utilizing this specific approach?
Explanation
Question 48
A 30-year-old construction worker sustains a severe pilon fracture and is initially treated with a spanning external fixator. At 14 days, the soft tissue envelope has improved and he undergoes definitive ORIF via an anterolateral approach to the distal tibia. During the superficial dissection, which of the following structures is most at risk of iatrogenic injury?
Explanation
Question 49
During the percutaneous placement of an S1 transiliac-transsacral screw for a posterior pelvic ring injury, the surgeon must be aware of sacral dysmorphism. Which of the following is a radiographic sign of sacral dysmorphism that indicates the S1 osseous corridor may be restricted or unsafe?
Explanation
Question 50
A 22-year-old male sustains a low-velocity handgun wound to the mid-thigh. Radiographs reveal a comminuted midshaft femur fracture. The patient has a normal neurovascular examination and the wounds are clean with 5 mm entry and exit holes. What is the most appropriate definitive management?
Explanation
Question 51
A 65-year-old female sustains a valgus-impacted proximal humerus fracture. The medial calcar hinge is completely disrupted. According to recent quantitative anatomical studies, which of the following blood vessels provides the primary vascular supply to the humeral head articular segment?
Explanation
Question 52
A 40-year-old male presents with a closed midshaft clavicle fracture with 100% displacement and 2.5 cm of shortening. Compared to nonoperative management with a sling, what is the most significant clinical advantage of open reduction and internal fixation for this patient?
Explanation
Question 53
A 55-year-old man sustains a perilunate dislocation and undergoes open reduction and ligament repair. To restore carpal stability, the surgeon identifies and repairs the primary ligamentous stabilizers. Which of the following intrinsic/extrinsic ligaments is considered the primary volar stabilizer of the lunate to the radius?
Explanation
Question 54
A 35-year-old woman sustains a closed, isolated transverse fracture of the middle third of the humeral shaft. She is initially treated with a coaptation splint and transitioned to a functional fracture brace. Which of the following represents an absolute contraindication to continued nonoperative treatment with functional bracing?
Explanation
Question 55
A 50-year-old male is involved in a high-speed collision and sustains an APC II (anteroposterior compression) pelvic ring injury with widening of the symphysis pubis. If isolated internal fixation is planned for the anterior ring, which of the following statements regarding the biomechanics of symphyseal plating is correct?
Explanation
Question 56
A 25-year-old man sustains a subtrochanteric femur fracture following a motor vehicle collision. During closed reduction and intramedullary nailing, the proximal fracture fragment is notoriously difficult to reduce due to the deforming forces of the attached musculature. Which of the following muscles is primarily responsible for the external rotation deformity of the proximal segment?
Explanation
Question 57
A 35-year-old male is brought to the trauma bay after a motorcycle collision.
He is hypotensive (BP 75/40 mmHg) and tachycardic (HR 130 bpm). A FAST exam is negative. A pelvic radiograph shows an anteroposterior compression type III (APC-III) pelvic ring injury. A pelvic binder is applied, and he receives 2 units of uncrossmatched blood, but his hemodynamics remain unstable. What is the most appropriate next step in management?

Explanation
Question 58
A 28-year-old woman sustains a displaced talar neck fracture following a fall from a height. The surgeon plans an open reduction and internal fixation to restore articular congruity and mitigate the risk of avascular necrosis (AVN). The primary blood supply to the body of the talus, which is at risk in this injury, is derived from the:
Explanation
Question 59
A 45-year-old male sustains a bicondylar tibial plateau fracture.
Preoperative computed tomography (CT) scan reveals a large, displaced posteromedial coronal shear fragment. What is the most appropriate surgical approach to anatomically reduce and buttress this specific fragment?
Explanation
Question 60
A 55-year-old woman presents with the inability to flex the interphalangeal joint of her thumb 6 months after undergoing open reduction and internal fixation of a distal radius fracture. Radiographs show a healed fracture, but the volar locking plate is positioned distal to the watershed line of the radius. Which of the following tendons is most likely injured?
Explanation
Question 61
A 30-year-old male sustains a severe open tibial shaft fracture (Gustilo-Anderson Type IIIB) following a high-speed motor vehicle collision. He is brought to the trauma center 45 minutes after the injury. According to current evidence, which of the following interventions has the greatest impact on reducing his risk of deep infection?
Explanation
Question 62
A 28-year-old male sustains a displaced, vertically oriented (Pauwels type III) femoral neck fracture.
Which of the following fixation constructs provides the most biomechanical stability for this specific fracture pattern?

Explanation
Question 63
A 22-year-old athlete sustains a hyperplantarflexion injury to his midfoot with severe pain and swelling. Radiographs demonstrate widening of the space between the first and second metatarsal bases and a small bony avulsion in this interval ('fleck sign'). The avulsed bone fragment originates from the attachment of the Lisfranc ligament. This ligament connects which of the following structures?
Explanation
Question 64
A 40-year-old construction worker undergoes open reduction and internal fixation of a displaced intra-articular calcaneus fracture via a standard extensile lateral approach. Postoperatively, he complains of numbness and tingling along the lateral aspect of his hindfoot. Which of the following nerves was most likely injured during the surgical approach?
Explanation
Question 65
A 24-year-old patient undergoes arthroscopic stabilization for recurrent anterior shoulder instability. Preoperative imaging reveals a large Hill-Sachs lesion that engages the anterior glenoid rim with the arm in abduction and external rotation. Glenoid bone loss is estimated at 10%. In addition to an arthroscopic Bankart repair, which of the following procedures is most appropriate to address the humeral head defect?
Explanation
Question 66
A 45-year-old farmer sustains a highly contaminated open fracture of the tibial shaft after his leg is caught in a tractor mechanism. The wound is 12 cm long with extensive soft tissue stripping, but adequate soft tissue coverage is achievable. According to the Gustilo-Anderson classification, what is the most appropriate initial intravenous antibiotic regimen?
Explanation
Question 67
A 35-year-old man involved in a high-speed motor vehicle collision sustains a closed subtrochanteric femur fracture. During closed reduction and intramedullary nailing, the proximal fragment is noted to be highly displaced. Which of the following muscles is primarily responsible for the flexion and external rotation of the proximal fracture fragment?
Explanation
Question 68
A 55-year-old woman is evaluated 4 months after undergoing open reduction and internal fixation of a distal radius fracture with a volar locking plate. She complains of new-onset inability to actively flex the interphalangeal (IP) joint of her thumb. Radiographs reveal the volar plate is positioned distal to the watershed line. What is the most likely cause of her symptom?
Explanation
Question 69
A 25-year-old man sustains a completely displaced Pauwels type III (vertical shear) fracture of the femoral neck. He is otherwise healthy. To minimize the risk of nonunion and avascular necrosis, what is the most biomechanically sound surgical construct for this patient?
Explanation
Question 70
A 40-year-old man is brought to the trauma bay after a motorcycle crash. His blood pressure is 80/40 mmHg and heart rate is 130 bpm. Pelvic radiographs demonstrate an anteroposterior compression type III (APC-III) pelvic ring injury with marked symphyseal diastasis. A FAST exam is negative. What is the most appropriate initial step to acutely reduce pelvic volume and aid hemodynamic stability?
Explanation
Question 71
A 30-year-old man sustains a closed midshaft humerus fracture after a fall. On examination in the emergency department, he exhibits a complete wrist drop and inability to actively extend his metacarpophalangeal joints, but has palpable distal pulses. What is the most appropriate initial management of his neurologic deficit?
Explanation
Question 72
A 28-year-old roofer falls 15 feet, landing on his feet, and sustains a Hawkins Type III fracture of the talar neck. According to the Hawkins classification, what anatomic disruptions define a Type III fracture, and what is the approximate risk of avascular necrosis (AVN) of the talar body?
Explanation
Question 73
A 22-year-old collegiate football player sustains an anterior knee dislocation which is immediately reduced on the field. In the emergency department, his knee is splinted. His dorsalis pedis and posterior tibial pulses are palpable but diminished compared to the contralateral side. The ankle-brachial index (ABI) is calculated to be 0.82. What is the most appropriate next step in management?
Explanation
Question 74
A 45-year-old man sustains a complex tibial plateau fracture. CT imaging demonstrates a large, displaced posteromedial shear fragment. To adequately visualize and anatomically reduce this fragment using a buttress plate, which surgical approach is most appropriate?
Explanation
Question 75
A 35-year-old driver is involved in a severe motor vehicle collision. Pelvic radiographs and computed tomography (CT) reveal an acetabular fracture. The fracture line disrupts the anterior column and extends inferiorly through the anterior wall. A separate transverse fracture line is noted traversing the posterior column, but the superior portion of the posterior column and the ilium remain solidly attached to the axial skeleton. According to the Judet-Letournel classification, what is the correct diagnosis?
Explanation
Question 76
A 35-year-old man is brought to the emergency department after a motorcycle collision. He is hypotensive with a blood pressure of 80/50 mm Hg. A pelvic radiograph shows a widened pubic symphysis consistent with an anteroposterior compression (APC) injury. You decide to apply a pelvic binder to provide temporary stability. To most effectively reduce the pelvic volume, at what anatomical level should the binder be centered?
Explanation
Question 77
A 28-year-old male sustains an isolated, closed, low-velocity gunshot wound to the midshaft femur. Radiographs reveal a comminuted midshaft femur fracture. He is neurovascularly intact, and there is no evidence of a compartment syndrome. Which of the following is the most appropriate management?
Explanation
Question 78
A 72-year-old female presents with severe groin pain and an inability to bear weight after a mechanical fall from standing. Radiographs reveal a displaced intracapsular femoral neck fracture. She has a history of mild hypertension, lives independently, and was an active community ambulator who played tennis twice a week prior to the injury. Which of the following treatments provides the lowest rate of reoperation and best functional outcome?
Explanation
Question 79
A 45-year-old male falls from a height of 15 feet and sustains a high-energy closed pilon fracture. Clinical examination reveals severe swelling, tense skin, and hemorrhagic fracture blisters over the medial and lateral aspects of the ankle. Which of the following represents the most appropriate initial management?
Explanation
Question 80
A 28-year-old male sustains a displaced talar neck fracture following a high-energy snowboard crash. You counsel him on the high risk of avascular necrosis (AVN) of the talar body due to the disruption of its precarious blood supply. Which of the following vessels provides the predominant blood supply to the body of the talus?
Explanation
Question 81
A 22-year-old male is struck by a motor vehicle and sustains a closed transverse midshaft tibia fracture, treated with reamed intramedullary nailing. Postoperatively, he requires rapidly increasing doses of opioids for leg pain. Examination reveals a tense leg, and passive extension of the great toe elicits excruciating pain. Which of the following compartments is most likely experiencing critically elevated pressures?
Explanation
Question 82
A 54-year-old male sustains a traumatic anterior shoulder dislocation. Post-reduction radiographs demonstrate a concentric reduction of the glenohumeral joint, but reveal an associated greater tuberosity fracture with 8 mm of superior displacement. What is the most appropriate management plan?
Explanation
Question 83
A 34-year-old man sustains a pelvic injury following a high-speed motor vehicle collision. An anteroposterior radiograph of the pelvis demonstrates a complex fracture involving the acetabulum. An obturator oblique radiograph clearly demonstrates a 'spur sign'. This radiographic finding is pathognomonic for which of the following acetabular fracture patterns?
Explanation
Question 84
A 30-year-old man sustains a severe open tibia fracture (Gustilo-Anderson IIIB) requiring a free tissue transfer for soft-tissue coverage. To minimize the risk of deep infection and maximize flap survival, the classic study by Godina demonstrated the best outcomes when coverage is performed within what timeframe?
Explanation
Question 85
A 22-year-old collegiate football player sustains a severe axial load to a plantarflexed foot. Radiographs reveal widening of the space between the medial and middle cuneiforms, with dorsal displacement of the second metatarsal base. The primary stabilizing structure of the Lisfranc joint complex connects which two bones?
Explanation
Question 86
A 35-year-old male is involved in a motor vehicle collision and sustains a posterior hip dislocation. Closed reduction is performed in the emergency department within 2 hours. A post-reduction CT scan demonstrates a posterior wall fracture involving 15% of the articular surface. There are no intra-articular fragments, and the joint is congruous. Dynamic fluoroscopic stress examination reveals a stable hip. What is the most appropriate definitive management?
Explanation
Question 87
A 45-year-old female sustains a closed, midshaft humerus fracture and is treated with a functional brace. At 12 weeks follow-up, she complains of persistent pain and mobility at the fracture site. Radiographs demonstrate no bridging callus formation. Which of the following factors is most strongly associated with nonunion in humeral shaft fractures treated with functional bracing?
Explanation
Question 88
A 22-year-old healthy male presents with a completely displaced midshaft clavicle fracture. Which of the following is considered a widely accepted relative indication for open reduction and internal fixation to improve functional outcomes and decrease nonunion risk?
Explanation
Question 89
A 68-year-old female undergoes open reduction and internal fixation of a distal femur fracture using a lateral locking plate. Six months postoperatively, she presents with implant failure and a nonunion. Radiographs reveal plate breakage at the level of the fracture. Which of the following surgical technique errors most likely contributed to this complication?
Explanation
Question 90
Which of the following physical examination findings is considered the most reliable and earliest clinical indicator of acute compartment syndrome in an alert patient with a closed tibial shaft fracture?
Explanation
Question 91
A 30-year-old male sustains a mechanically and hemodynamically unstable anteroposterior compression (APC-III) pelvic ring injury. A circumferential pelvic binder is applied in the trauma bay. To achieve optimal mechanical stability and maximal reduction in pelvic volume, over which anatomical landmark should the center of the binder be positioned?
Explanation
Question 92
In the surgical treatment of a young adult with a displaced, intracapsular femoral neck fracture, which of the following factors is most consistently associated with minimizing the risk of osteonecrosis (AVN) of the femoral head?
Explanation
Question 93
A 45-year-old male sustains a closed tongue-type calcaneus fracture. Physical examination reveals tense, blanched skin over the posterior heel. What is the most appropriate next step in management?
Explanation
Question 94
During open reduction and internal fixation of a completely displaced, transverse patella fracture, a tension band wiring technique is utilized. What is the primary biomechanical function of the anteriorly placed tension band wire during active knee flexion?
Explanation
Question 95
A 55-year-old male sustains a traumatic posterior hip dislocation. Following a successful closed reduction in the emergency department, what is the most appropriate imaging modality to evaluate for intra-articular loose bodies and ensure concentric reduction?
Explanation
Question 96
A 34-year-old female sustains a Denis Zone I sacral fracture with 1.5 cm of cephalad displacement following a fall from a height. She complains of weakness in foot dorsiflexion and big toe extension. Which nerve root is most likely injured in this specific fracture pattern?
Explanation
Question 97
A 32-year-old male sustains a displaced basicervical femoral neck fracture following a high-energy trauma. Which of the following internal fixation constructs provides the greatest biomechanical stability for this specific fracture pattern?
Explanation
Question 98
A 28-year-old man sustains a talar neck fracture following a high-energy motor vehicle collision. Radiographs demonstrate displacement of the talar neck with subluxation of the subtalar joint, but the tibiotalar and talonavicular joints remain congruent. According to the Hawkins classification, what is the approximate risk of developing avascular necrosis (AVN) of the talar body?
Explanation
Question 99
A 40-year-old farmer sustains an open midshaft tibia fracture after his leg is caught in a tractor mechanism. The wound is 8 cm long with moderate soft-tissue damage, but there is adequate periosteal coverage of the bone. He is taken to the operating room within 6 hours for surgical debridement. Which of the following intravenous antibiotic regimens is most appropriate for initial management?
Explanation
Question 100
A 22-year-old male presents with a closed proximal third tibia fracture. Eight hours post-injury, he complains of severe leg pain out of proportion to the injury that is refractory to intravenous opioids. His leg is swollen and tense, and passive stretch of the great toe severely exacerbates his pain. Pulses remain palpable. Intracompartmental pressure testing is performed. Which of the following pressure measurements establishes an absolute indication for emergent four-compartment fasciotomy?
Explanation
None
