Trauma Board Review 2009: High-Yield MCQs (Set 2)

Key Takeaway
This article provides essential research regarding Trauma Board Review 2009: High-Yield MCQs (Set 2). Access high-yield Trauma questions for the 2009 board exam. This module (Set 2) covers critical topics including surgical techniques, pathology, and treatment protocols with verified answers.
Trauma Board Review 2009: High-Yield MCQs (Set 2)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 20-year-old man is brought to the emergency department after a high-speed motor vehicle accident. His initial blood pressure is 70/40 mm Hg. He is currently receiving intravenous fluids as well as blood. His Focused Assessment with Sonography for Trauma examination did not show any free fluid in his abdomen and his chest radiograph is unremarkable. An AP pelvis radiograph is shown in Figure 15. What is the next most appropriate step in the management of his pelvic injury?

Explanation
Question 2
A 7-year-old girl is hit by a motor vehicle and sustains the isolated ipsilateral injuries shown in Figures 16a and 16b. What is the optimal definitive method of treatment?

Explanation
Question 3
What is the most common cause of errors that harm patients?

Explanation
Question 4
A 220-lb 20-year-old man was involved in a motor vehicle accident. His work-up reveals that he has multiple long bone fractures as well as a splenic injury that is currently being managed nonsurgically. His initial blood pressure in the trauma bay was 70/30 mm Hg. After receiving 4 liters of fluid and 3 units of packed red blood cells, his blood pressure is currently 110/70, his heart rate is 100, his urine output is 90 mL/h (normal 0.5 to 1 mL/kg/h), and his core temperature is 97.9 degrees F (36.5 degrees C). At this point, the patient's resuscitation can be described as which of the following?

Explanation
Question 5
A 30-year-old man who sustained a work-related injury 6 weeks ago reports persistent back and left-sided buttock pain that has been attributed to lumbar transverse process fractures. A pelvic radiograph and CT scans obtained 2 days ago are seen in Figures 17a through 17c. What is the best treatment for his injury?
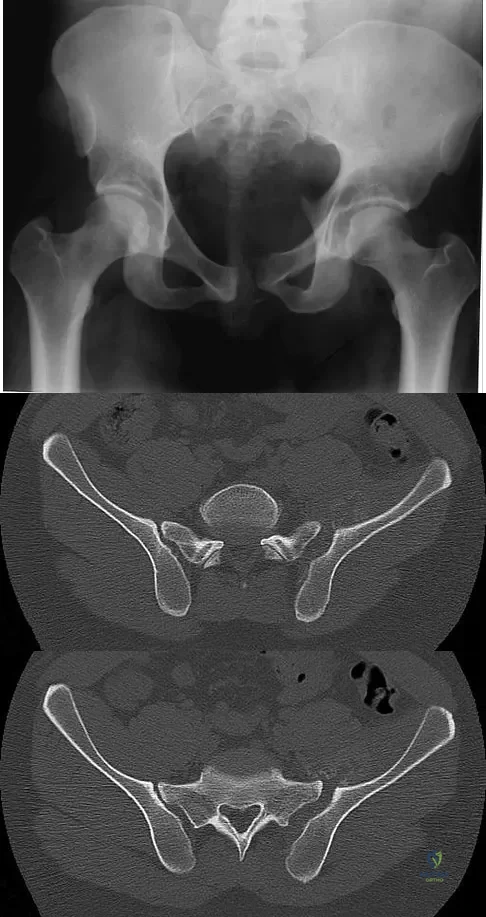
Explanation
Question 6
A 36-year-old woman was injured in a train derailment. She has a significant open depressed skull fracture with active bleeding, a hemopneumothorax, and blood in the left upper quadrant and colic gutter by Focused Assessment with Sonography for Trauma (FAST) examination. Additionally, she has the pelvic injury seen on the CT scans in Figures 18a and 18b. The mortality rate for this patient approaches
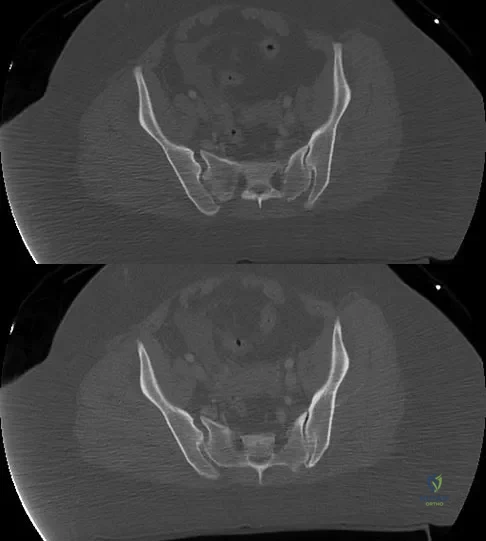
Explanation
Question 7
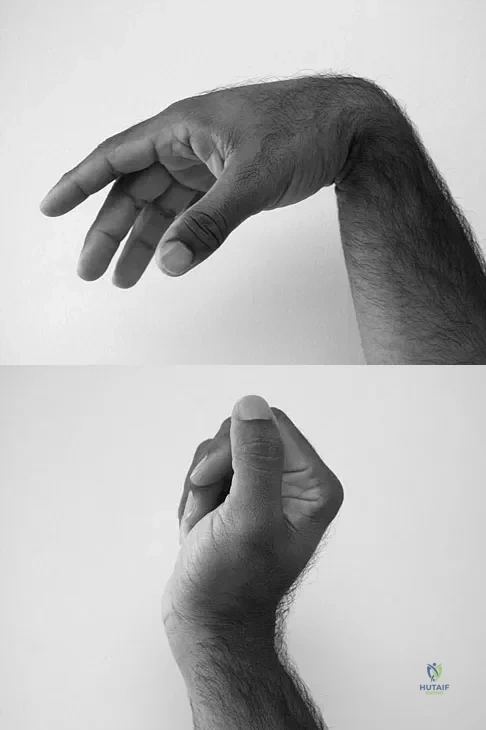
A 19-year-old collegiate baseball player injures the ring finger on his dominant hand while sliding headfirst into second base. He reports that he is unable to actively flex or extend the distal interphalangeal joint of the finger. Radiographs are shown in Figures 19a and 19b. What is the anatomic lesion leading to this injury?

Explanation
Question 8
A 72-year-old man was involved in an automobile accident 4 weeks ago. Initially he noted pain about his nondominant left shoulder, which resolved within a few weeks after the accident. He now describes trouble with gripping and carrying items in his left hand. Radiographs are shown in Figures 20a through 20c. His signs and symptoms are the result of injury to which of the following ligaments?

Explanation
Question 9
To avoid an injury to the L5 nerve root when placing an S1 sacroiliac screw, what area of the sacrum should be avoided on the lateral C arm image shown in Figure 21?

Explanation
Question 10
An otherwise healthy 37-year-old man fell off the flatbed of a delivery truck and landed directly on his dominant left hand. Surgical stabilization of a distal radius fracture is performed. An intraoperative radiograph is shown in Figure 22. What is the next most appropriate step in management?

Explanation
Question 11
A 36-year-old woman is placed in a short arm cast for a nondisplaced extra-articular distal radius fracture. Seven weeks later she notes the sudden inability to extend her thumb. What is the most likely cause of her condition?

Explanation
Question 12
In Gustilo type III open tibial diaphyseal fractures, which of the following factors is associated with an increased risk of a poor functional outcome?

Explanation
Question 13
Figures 23a and 23b show the radiographs of a 75-year-old woman who sustained an injury to her nondominant hand. Initial treatment should consist of

Explanation
Question 14
A 43-year-old man sustained a closed, intra-articular pilon fracture. It has now been 1 year since he underwent open reduction and internal fixation. Which of the following statements most accurately describes his perceived outcome?

Explanation
Question 15
The injury shown in Figure 24 was most likely caused by what mechanism of injury?

Explanation
Question 16
A 21-year-old college student fell from a balcony and landed on his outstretched right hand. He is seen in the emergency department 4 hours later and reports wrist pain and diffuse hand numbness. The volar forearm compartment is soft and there is no pain with passive finger extension. Radiographs are shown in Figures 25a and 25b. Definitive treatment should consist of

Explanation
Question 17
A 9-year-old boy falls from a scooter and sustains the injury shown in the radiographs in Figure 26. After closed reduction and cast immobilization, what is the most likely complication that can result?

Explanation
Question 18
A 69-year-old man sustains a traumatic amputation to the distal phalanx of his little finger while working with power tools. Radiographs are shown in Figures 27a and 27b. The patient was instructed how to perform wet-to-dry dressing changes in the emergency department. Clinical pictures taken in the office are shown in Figures 27c through 27e. What is the most appropriate management of this soft-tissue wound?

Explanation
Question 19
A 32-year-old man has an open comminuted humeral shaft fracture. Examination reveals absence of sensation in the first web space and he is unable to fully extend the thumb, fingers, and wrist. What is the recommended treatment following irrigation and debridement of the fracture?

Explanation
Question 20
Which of the following complications is associated with the use of a short cephalomedullary nail for fixation of intertrochanteric hip fractures?

Explanation
Question 21
A 19-year-old man sustained the isolated injury seen in Figure 28a. He is adequately resuscitated. A closed reduction was performed in the emergency department, and postreduction radiographs are shown in Figures 28b and 28c. What is the next most appropriate step in management?

Explanation
Question 22
The iliopectineal fascia runs between which of the following structures?

Explanation
Question 23
Which of the following is most predictive of a medial side ankle injury in the presence of a fibula fracture above the level of the joint?

Explanation
Question 24
Figure 29 shows the radiograph of a 10-year-old boy who injured his knee playing football. What is the most appropriate initial treatment?

Explanation
Question 25
A 35-year-old man sustained a 1-inch stab incision in his proximal forearm while trying to use a screwdriver 2 weeks ago. The laceration was routinely closed, and no problems about the incision site were noted. He now reports that he has been unable to straighten his fingers or thumb completely since the injury. Clinical photographs shown in Figures 30a and 30b show the man passively flexing the wrist. What is the most appropriate management?
Explanation
Question 26
A 25-year-old male presents after a high-speed motorcycle collision with a closed right femur fracture, left tibial shaft fracture, and bilateral pulmonary contusions. The surgical team is debating between early total care (ETC) and damage control orthopedics (DCO). Which of the following serum markers provides the most reliable indicator of adequate resuscitation to safely proceed with definitive intramedullary nailing of both long bones?
Explanation
Question 27
A 30-year-old man sustains a closed, isolated, displaced femoral neck fracture. Radiographs demonstrate a vertically oriented fracture line with an angle greater than 50 degrees from the horizontal (Pauwels Type III). What biomechanical construct provides the most stable fixation against the dominant deforming forces for this specific fracture pattern?
Explanation
Question 28
A 42-year-old farmer sustains a severe open tibia fracture after his leg is caught in a piece of agricultural machinery. The wound is 14 cm long with extensive soft tissue stripping, bone loss, and gross contamination with soil and manure. According to current guidelines, which of the following is the most appropriate initial intravenous antibiotic regimen?
Explanation
Question 29
A 28-year-old motorcyclist presents to the trauma bay with an avulsed, flail, and pulseless upper extremity. Radiographs show a massively laterally displaced scapula, an intact clavicle, and complete acromioclavicular separation. What is the most common vascular injury associated with this diagnosis?
Explanation
Question 30
A 35-year-old man falls from a 15-foot ladder and sustains a displaced fracture of the talar neck. Imaging reveals subluxation of both the subtalar and tibiotalar joints, but the talonavicular joint remains reduced. What is the approximate reported risk of developing avascular necrosis (AVN) of the talar body in this injury pattern?
Explanation
Question 31
During the ilioinguinal approach for open reduction and internal fixation of an anterior column acetabular fracture, vigorous arterial bleeding is encountered on the posterior aspect of the superior pubic ramus, approximately 5 cm from the pubic symphysis. Which of the following anatomic structures is the most likely source of this bleeding?
Explanation
Question 32
A 45-year-old roofer undergoes open reduction and internal fixation of a displaced intra-articular calcaneus fracture via an extensile lateral approach. Postoperatively, he complains of significant numbness and burning pain along the lateral aspect of his foot. Which of the following nerves was most likely injured during the surgical approach?
Explanation
Question 33
A 38-year-old unrestrained driver presents with a severely swollen knee after a motor vehicle collision. CT scan reveals a supracondylar distal femur fracture with an associated intra-articular coronal plane fracture of the lateral femoral condyle. Which of the following accurately describes the biomechanically optimal fixation for this coronal plane component?
Explanation
Question 34
A 24-year-old man sustains a closed comminuted tibial shaft fracture. Two hours after presentation, he complains of severe pain out of proportion to the injury that is not relieved by intravenous narcotics. His leg is swollen and tense. Compartment pressures are measured. What pressure differential (Delta P) is considered the absolute threshold for performing an emergency four-compartment fasciotomy?
Explanation
Question 35
A 28-year-old man sustains a closed spiral fracture of the middle third of the humerus after an arm-wrestling match. On examination in the emergency department, he is unable to extend his wrist or fingers, and he has decreased sensation over the dorsal first web space. What is the most appropriate initial management?
Explanation
Question 36
A 45-year-old polytrauma patient is brought to the trauma bay after a high-speed motor vehicle collision. He presents with a severe head injury (Glasgow Coma Scale score of 7) and a closed midshaft femur fracture. According to current guidelines for Damage Control Orthopedics (DCO), what is the most appropriate initial management of the femur fracture?
Explanation
Question 37
A 28-year-old man sustains a Pauwels type III (vertical) femoral neck fracture after falling from a ladder. Which of the following fixation constructs provides the most biomechanically stable fixation against shear forces for this specific fracture pattern?
Explanation
Question 38
A 35-year-old woman sustains a highly comminuted distal femur fracture following a high-energy trauma. Computed tomography (CT) imaging reveals an isolated coronal plane fracture of the lateral femoral condyle. What is the eponym for this specific fracture fragment?
Explanation
Question 39
A 30-year-old man sustains an open tibia fracture with massive soft tissue stripping and exposed bone (Gustilo-Anderson IIIB) after a motorcycle collision. After initial thorough surgical debridement and bony stabilization, what is the optimal timeframe for definitive soft tissue coverage to minimize the risk of deep infection and flap failure?
Explanation
Question 40
A 65-year-old woman presents with an isolated closed, highly displaced distal radius fracture. She undergoes closed reduction and splinting in the emergency department. Which of the following nerves is at greatest risk of developing an acute compression neuropathy following this specific injury and manipulation?
Explanation
Question 41
A 25-year-old man falls from a height of 20 feet, sustaining a displaced, intra-articular calcaneus fracture. The Sanders classification system is utilized to guide surgical management based on CT imaging. What is the primary anatomical landmark assessed on coronal CT to determine the Sanders classification?
Explanation
Question 42
A 40-year-old man sustains a Hawkins type III fracture of the talar neck after a severe motor vehicle collision. What is the approximate reported risk of developing avascular necrosis (AVN) of the talar body with this specific injury pattern?
Explanation
Question 43
Which of the following statements is most accurate regarding the initial management of a traumatic, hemodynamically unstable pelvic ring disruption?
Explanation
Question 44
A 55-year-old man presents with a closed, highly comminuted tibial shaft fracture. His diastolic blood pressure is 60 mm Hg. What absolute intra-compartmental pressure would meet the widely accepted delta pressure threshold for performing an immediate four-compartment fasciotomy?
Explanation
Question 45
A 22-year-old male sustains a severe pelvic trauma. Radiographs and CT imaging reveal a transverse fracture of the acetabulum combined with a posterior wall fracture. According to the Letournel and Judet classification of acetabular fractures, which of the following categories best describes this injury?
Explanation
Question 46
A 35-year-old man sustains a severe open tibia fracture (Gustilo-Anderson IIIB) in a motorcycle crash. He is hemodynamically stable. Which of the following factors has been shown in the literature to be the most critical independent predictor for reducing the risk of deep infection in this patient?
Explanation
Question 47
A 28-year-old male is admitted with a closed midshaft tibia fracture. Overnight, he develops increasing pain out of proportion to his injury that is poorly responsive to IV opioids. Pain is elicited with passive stretch of his hallux. You measure his compartment pressures. Which of the following parameters represents an absolute indication for emergency fasciotomy?
Explanation
Question 48
A 25-year-old female presents with a high-energy Pauwels type III (vertical shear) femoral neck fracture. Which of the following internal fixation constructs provides the most biomechanical stability for this specific fracture pattern?
Explanation
Question 49
A 40-year-old male motorcyclist experiences a severe lateral traction injury to his right shoulder. He presents with massive shoulder swelling, an absent right radial pulse, and a completely flail right upper extremity. Radiographs reveal a widened scapulothoracic articulation and lateral displacement of the scapula. What is the most likely associated neurologic injury?
Explanation
Question 50
In a polytrauma patient with bilateral femur fractures and a pulmonary contusion, 'Damage Control Orthopedics' (DCO) with temporary external fixation is being considered over Early Total Care (ETC) with intramedullary nailing. Which of the following physiological parameters classifies the patient as 'borderline' and supports the use of DCO?
Explanation
Question 51
A 22-year-old male football player sustains a spontaneous reduction of a knee dislocation prior to arrival at the emergency department. He has a grossly unstable knee but normal, palpable dorsalis pedis and posterior tibial pulses. What is the most appropriate next step in his management to evaluate for vascular injury?
Explanation
Question 52
A 45-year-old roofer falls 15 feet, sustaining a displaced, intra-articular calcaneus fracture. You review his imaging to determine the Sanders classification. Which specific imaging modality and view dictates the Sanders classification for calcaneus fractures?
Explanation
Question 53
A 35-year-old male is undergoing open reduction and internal fixation of a transverse posterior wall acetabular fracture via a Kocher-Langenbeck approach. To minimize iatrogenic traction injury to the sciatic nerve during retraction, what is the optimal position of the operative lower extremity?
Explanation
Question 54
Six months after open reduction and internal fixation of a volar Barton's distal radius fracture using a volar locked plate, a 65-year-old female presents with sudden inability to actively flex the interphalangeal (IP) joint of her thumb. What is the most likely etiology of this complication?
Explanation
Question 55
A 32-year-old male is brought to the trauma bay after a motorcycle crash. He has an 'open book' pelvic ring injury (APC III) and is hemodynamically unstable. In severe pelvic fractures with massive volume expansion, what is the primary anatomical source of the life-threatening hemorrhage?
Explanation
Question 56
An 82-year-old man presents with a hip injury after a mechanical fall. Radiographs and CT scan show an anterior column and posterior hemitransverse acetabular fracture with severe superomedial dome impaction (the "gull sign"). Which of the following factors most strongly predicts early failure if open reduction and internal fixation alone is chosen?
Explanation
Question 57
A 30-year-old man with a closed midshaft tibia fracture complains of severe leg pain out of proportion to his injury, worsening with passive toe stretch. His blood pressure is 110/60 mm Hg. Intracompartmental pressure monitoring reveals an anterior compartment pressure of 40 mm Hg. What is the most appropriate next step in management?
Explanation
Question 58
A 25-year-old man sustains a displaced, vertically oriented (Pauwels type III) femoral neck fracture. He undergoes open reduction and internal fixation. What biomechanical advantage does a sliding hip screw with a derotation screw provide over three parallel cancellous screws for this specific fracture pattern?
Explanation
Question 59
What is the most critical factor in reducing the risk of infection in a patient who sustains a severe, open tibia fracture in a high-speed motor vehicle collision?
Explanation
Question 60
A 22-year-old man sustains a low-velocity gunshot wound to the right distal thigh. Radiographs demonstrate a comminuted fracture of the distal femoral diaphysis with the bullet lodged in the adjacent soft tissues. Distal pulses are palpable, and the ABI is 1.0. Which of the following is the most appropriate initial soft tissue management?
Explanation
Question 61
A 35-year-old woman sustains a 'floating shoulder' injury, defined by ipsilateral displaced fractures of the clavicle and the scapular neck. Which of the following represents the primary biomechanical rationale for open reduction and internal fixation of the clavicle in this injury pattern?
Explanation
Question 62
A 68-year-old woman treated with alendronate for 8 years presents with a 3-month history of an unprovoked dull ache in her right thigh. A radiograph of the femur reveals localized lateral cortical thickening and a transverse radiolucent line in the subtrochanteric region. What is the most appropriate next step in orthopaedic management?
Explanation
Question 63
A 42-year-old man sustains an anteroposterior compression type II (APC II) pelvic ring injury. He is hemodynamically stable. Imaging shows a 3.5 cm symphyseal diastasis and bilateral anterior sacroiliac joint widening. The posterior sacroiliac ligaments are intact. What is the optimal surgical treatment to restore pelvic ring stability?
Explanation
Question 64
A 55-year-old woman undergoes volar locked plating for a displaced intra-articular distal radius fracture. Six weeks postoperatively, she suddenly loses the ability to actively extend her thumb interphalangeal joint. What is the most likely etiology of this complication?
Explanation
Question 65
A 45-year-old man sustains a closed, highly comminuted tibial pilon fracture with severe soft tissue swelling and multiple clear and blood-filled fracture blisters over the ankle. What is the preferred initial management strategy?
Explanation
Question 66
A 25-year-old man sustains a low-velocity gunshot wound to the right thigh, resulting in a comminuted midshaft femur fracture. The bullet is retained in the soft tissues adjacent to the fracture. Distal pulses are palpable and symmetrical to the contralateral limb, and there are no expanding hematomas. What is the most appropriate initial management of the wound and fracture?
Explanation
Question 67
A 32-year-old man is brought to the trauma bay after a fall from a height of 15 feet. Radiographs reveal a displaced basicervical femoral neck fracture. Which of the following internal fixation constructs is considered biomechanically superior for this specific fracture pattern?
Explanation
Question 68
A 30-year-old farmer with no known allergies sustains a severe open tibia fracture (Gustilo-Anderson Type IIIA) heavily contaminated with manure and soil. In addition to a first-generation cephalosporin and an aminoglycoside, which of the following antibiotics is most critical to include in his initial prophylactic regimen?
Explanation
Question 69
A 28-year-old construction worker sustains a Hawkins type III talar neck fracture following a fall. At his 8-week postoperative follow-up, an AP radiograph of the ankle demonstrates 'Hawkins sign'. What does this radiographic finding represent?
Explanation
Question 70
A 40-year-old woman with a highly comminuted Schatzker VI tibial plateau fracture undergoes application of a spanning external fixator. Twelve hours postoperatively, she reports excruciating, unremitting leg pain that is out of proportion to her injury. Passive stretch of her toes elicits severe pain. Intracompartmental pressure testing reveals an anterior compartment pressure of 45 mm Hg. Her current blood pressure is 100/60 mm Hg. What is the most appropriate next step in management?
Explanation
Question 71
A 76-year-old female with advanced osteoporosis and severe preexisting osteoarthritis of the elbow sustains a comminuted, intra-articular distal humerus fracture (AO/OTA 13-C3) after a mechanical fall. Which of the following is the most appropriate definitive surgical intervention?
Explanation
Question 72
A 22-year-old motorcyclist is involved in a high-speed collision and presents with massive soft tissue swelling over the left shoulder and a flail, insensate left upper extremity. Radiographs reveal lateral displacement of the scapula with widening of the acromioclavicular joint. Which of the following nerve injuries is most strongly associated with this specific injury pattern?
Explanation
Question 73
A 35-year-old man falls from a height of 30 feet, sustaining a spinopelvic dissociation characterized by a U-shaped sacral fracture on imaging. Upon physical examination, he has decreased perianal sensation, loss of voluntary anal sphincter tone, and urinary retention. This clinical presentation is primarily due to injury at which of the following neurologic levels?
Explanation
Question 74
A 29-year-old active male falls directly onto his left shoulder, sustaining a completely displaced, shortened midshaft clavicle fracture. Which of the following radiographic or demographic characteristics is recognized as the most significant predictor for nonunion if this injury is treated nonoperatively?
Explanation
Question 75
A 21-year-old collegiate football player suffers a high-energy knee dislocation during a tackle. Upon arrival at the emergency department, his knee has spontaneously reduced. Pedal pulses are palpable, but his Ankle-Brachial Index (ABI) is measured at 0.8. What is the most appropriate next step in his management?
Explanation
Question 76
In the context of damage control orthopaedics for a polytrauma patient, when is it most appropriate to convert an external fixator of a femoral shaft fracture to a reamed intramedullary nail?
Explanation
Question 77
A 35-year-old man sustains an isolated closed tibial shaft fracture treated with a reamed intramedullary nail. Postoperatively, he develops severe pain out of proportion to the injury, which is markedly exacerbated by passive stretch of the hallux. His leg is tense and swollen. What is the most appropriate next step in management?
Explanation
Question 78
A 45-year-old man presents to the emergency department with a midshaft clavicle fracture after falling off his bicycle. Which of the following is considered an absolute indication for operative fixation of this injury?
Explanation
Question 79
A 25-year-old male sustains a low-velocity gunshot wound to the thigh, resulting in a minimally displaced midshaft femur fracture. The bullet completely traversed the thigh. Examination reveals normal distal pulses and no signs of compartment syndrome. What is the most appropriate management?
Explanation
Question 80
Which of the following injury patterns represents the classic 'terrible triad' of the elbow?
Explanation
Question 81
In the initial management of a severe Type II open tibia fracture, what is the single most important factor in decreasing the risk of deep infection?
Explanation
Question 82
A 30-year-old male sustains a talar neck fracture with subluxation of the subtalar joint (Hawkins Type II) after a fall from a height. Which of the following vascular structures provides the primary blood supply to the talar body and is most at risk of injury in this specific fracture pattern?
Explanation
Question 83
A 65-year-old female sustains a completely displaced, off-ended subtrochanteric femur fracture. She is scheduled for cephalomedullary nailing. To prevent the most common malreduction during this procedure, what intraoperative consideration is most critical?
Explanation
Question 84
A 40-year-old man presents with a pelvic ring injury after a high-speed motorcycle crash. An AP pelvis radiograph demonstrates widening of the pubic symphysis of 3.5 cm and widening of the left sacroiliac joint. He remains hemodynamically unstable (BP 70/40) despite receiving 2 liters of crystalloid and 2 units of PRBCs. What is the most appropriate next step in orthopedic management?
Explanation
Question 85
A 50-year-old woman is evaluated for a nonunion of a midshaft humerus fracture 6 months after injury. She was originally treated with a Sarmiento cast brace. Radiographs show atrophic bone ends with no callus formation. Laboratory markers for infection are negative. What is the most reliable surgical treatment?
Explanation
Question 86
Which of the following inflammatory markers is considered the most reliable early predictor for the development of acute respiratory distress syndrome (ARDS) and multiple organ dysfunction syndrome (MODS) in a polytrauma patient, guiding the decision between early total care and damage control orthopedics?
Explanation
Question 87
A 32-year-old man sustains a subtrochanteric femur fracture. During attempts at closed reduction, the proximal fracture fragment is noted to be severely flexed, abducted, and externally rotated. The abduction deformity of the proximal fragment is primarily caused by the pull of which of the following muscles?
Explanation
Question 88
A 45-year-old farmer is brought to the emergency department after his leg was caught in a tractor mechanism. He has sustained a Gustilo-Anderson Type III open tibia fracture that is heavily contaminated with soil and organic material. In addition to prompt surgical debridement, what is the most appropriate initial intravenous antibiotic regimen according to classic trauma guidelines?
Explanation
Question 89
A 40-year-old man sustains an anteroposterior compression type III (APC III) pelvic ring injury in a high-speed motorcycle collision. In the trauma bay, a pelvic binder is applied, and he receives massive transfusion protocol. His systolic blood pressure remains 70 mm Hg. The Focused Assessment with Sonography for Trauma (FAST) examination is negative, and a chest radiograph shows no abnormalities. What is the most appropriate next step in the management of this patient?
Explanation
Question 90
A 30-year-old woman undergoes closed reduction and percutaneous pinning of a Hawkins type II talar neck fracture. At her 8-week follow-up appointment, an anteroposterior radiograph of the ankle reveals a subchondral radiolucent band extending across the dome of the talus. What is the clinical significance of this radiographic finding?
Explanation
Question 91
A 28-year-old man is brought to the trauma center following a severe motor vehicle accident. On physical examination, his left upper extremity is flail, pale, and completely pulseless. Radiographs reveal massive lateral displacement of the left scapula, an intact clavicle, and complete disruption of the acromioclavicular joint. Which of the following associated injuries carries the highest risk of acute mortality in this patient?
Explanation
Question 92
A 6-year-old boy sustains a completely displaced, extension-type Gartland type III supracondylar humerus fracture. Prior to operative intervention, a thorough neurologic examination reveals that he is unable to actively flex the interphalangeal joint of his thumb and the distal interphalangeal joint of his index finger. Which of the following nerves has most likely been injured?
Explanation
Question 93
A 68-year-old woman with a history of osteoporosis treated with alendronate for the past 10 years presents with 3 months of progressive, severe right thigh pain worsened by weight-bearing. Plain radiographs show cortical thickening of the lateral cortex of the right subtrochanteric femur with a visible transverse radiolucent line. What is the most appropriate management of this patient's condition?
Explanation
Question 94
A 35-year-old man undergoes reamed intramedullary nailing for a closed diaphyseal tibia fracture. Twelve hours postoperatively, he complains of severe leg pain that is completely out of proportion to his injury and is unresponsive to escalating doses of intravenous opioids. On examination, he experiences severe pain upon passive flexion of his great toe. This finding specifically suggests compartment syndrome involving which of the following compartments of the leg?
Explanation
Question 95
A 42-year-old construction worker falls from a scaffolding, sustaining a severely displaced, closed, intra-articular calcaneus fracture. While evaluating the patient to determine whether operative or nonoperative management is indicated, which of the following patient-specific factors is considered a strong relative or absolute contraindication to open reduction and internal fixation through an extensile lateral approach?
Explanation
Question 96
A 28-year-old polytrauma patient presents to the emergency department after a high-speed motorcycle collision. He has bilateral closed femoral shaft fractures, severe pulmonary contusions, and a traumatic brain injury. His initial vital signs include a blood pressure of 85/50 mm Hg and a heart rate of 125 bpm. Laboratory studies reveal a lactate of 5.5 mmol/L, pH 7.20, and base excess of -8 mmol/L. According to the principles of damage control orthopedics (DCO), what is the most appropriate initial management of his bilateral femur fractures?
Explanation
Question 97
A 24-year-old man sustains a closed fracture of the middle third of the humeral shaft during an arm-wrestling match. On physical examination, he is unable to actively extend his wrist or fingers, and has decreased sensation over the dorsal first web space of the ipsilateral hand. Radiographs confirm a transverse midshaft humerus fracture. What is the most appropriate initial management?
Explanation
Question 98
A 30-year-old man sustains a low-velocity gunshot wound to the right leg. Radiographs reveal a comminuted midshaft tibia fracture. There is a 1-cm entrance wound on the anteromedial aspect of the leg and no exit wound. The bullet is lodged in the deep posterior compartment soft tissues. Distal pulses are strong, and compartment compartments are soft and compressible. What is the most appropriate initial management of the wound and fracture?
Explanation
Question 99
A 45-year-old male is brought to the trauma bay after being crushed by heavy machinery. His pelvis is unstable to manual compression, and radiographs confirm an anteroposterior compression (APC-III) pelvic ring injury. During the secondary survey, he complains of a severe inability to void, and the examining physician notes blood at the urethral meatus. What is the next most appropriate step in the evaluation of his urologic injury?
Explanation
Question 100
A 52-year-old farmer sustains an open tibial shaft fracture after his leg becomes entangled in an agricultural tiller. In the emergency department, the wound measures 12 cm in length with significant muscle crush injury, periosteal stripping, and visible heavy soil and manure contamination. According to classic evidence-based guidelines for open fractures, what is the most appropriate initial intravenous antibiotic regimen for this patient?
Explanation
None
