Trauma Board Review 2009: High-Yield MCQs (Set 4)

Key Takeaway
Here are the crucial details you must know about Trauma Board Review 2009: High-Yield MCQs (Set 4). Access high-yield Trauma questions for the 2009 board exam. This module (Set 4) covers critical topics including surgical techniques, pathology, and treatment protocols with verified answers.
Trauma Board Review 2009: High-Yield MCQs (Set 4)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A still active 86-year-old pastry chef falls in her kitchen and notes pain and deformity of her little finger. There are no open wounds. Radiographs are shown in Figures 49a and 49b. What is the most appropriate management?

Explanation
Question 2
A 32-year-old man has a Glasgow Coma Scale score of 8 and an open pelvic fracture. The patient's family reports that he is a Jehovah's Witness. Initial hemodynamic instability has resolved. In the operating room during a washout, the patient's blood pressure becomes unstable. What is the most appropriate action?
Explanation
Question 3
Figure 50 shows the radiograph of a 26-year-old man who sustained an isolated open injury to his foot. Examination reveals no gross contamination in the wound. There is a palpable dorsalis pedis pulse and sensation is present on the dorsal and plantar aspects of the foot. Initial treatment should consist of wound debridement, antibiotics, and

Explanation
Question 4
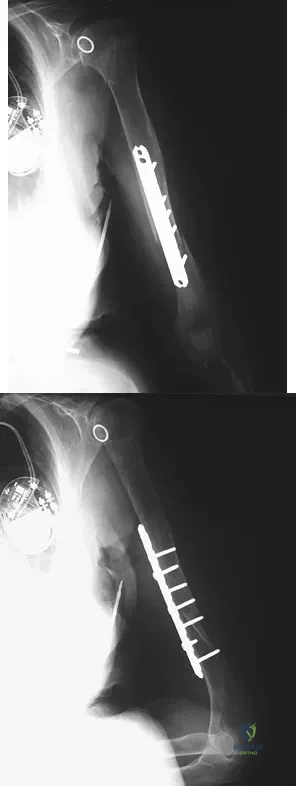
An 86-year-old woman sustained a fracture of the humerus and underwent surgical fixation 8 weeks ago. There was no radial nerve function below the elbow after surgery. Radiographs are shown in Figures 51a and 51b. What is the most appropriate management at this time?
Explanation
Question 5
Which of the following long bone fracture patterns occurs after a pure bending force is exerted to the bone?
Explanation
Question 6
A 20-year-old man sustained an isolated displaced type II odontoid fracture in a motor vehicle accident. He is neurologically intact. Treatment consists of placement in halo traction, and the fracture is reduced. What is the next most appropriate step in treatment?
Explanation
Question 7
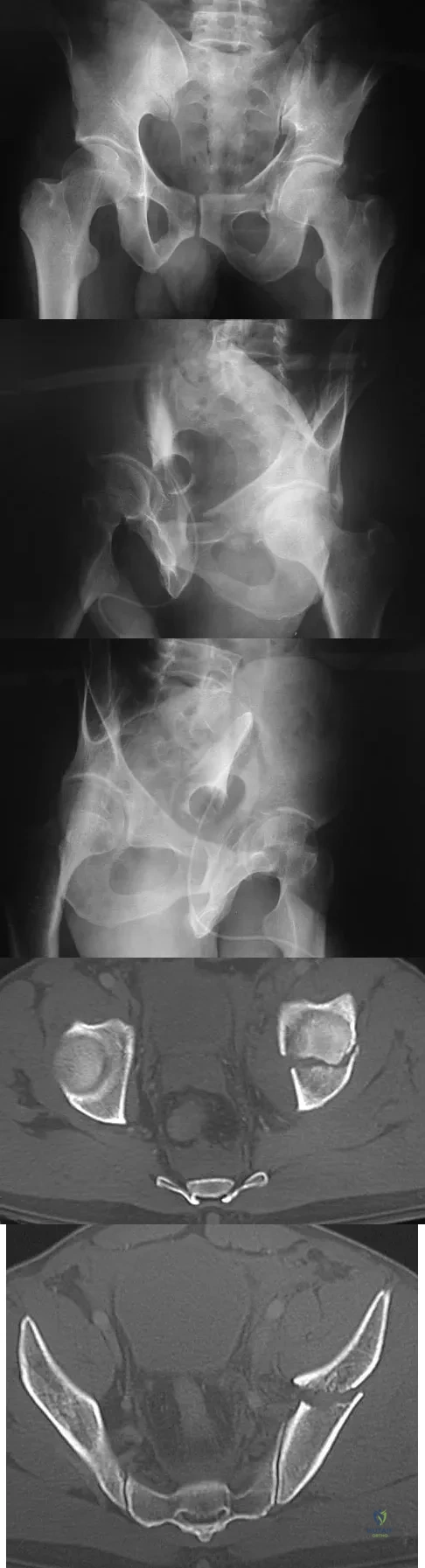
A 38-year-old woman fell from a ladder onto her right hip. The radiographs and CT scan are shown in Figures 52a through 52d. What is the best surgical approach for this fracture?

Explanation
Question 8
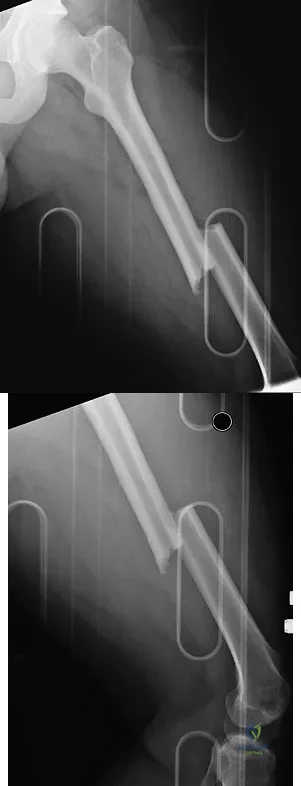
A 24-year-old man was thrown from a car and is seen in the emergency department with a Glasgow Coma Scale (GCS) score of 8. A CT scan of the head shows no significant bleeding. The patient is hemodynamically stable. The left femur has the closed injury shown on the radiographs in Figures 53a and 53b. What is the best treatment for this patient?
Explanation
Question 9
An otherwise healthy 26-year-old woman is involved in a high speed motor vehicle accident and sustains the injury shown in Figure 54 to her dominant right arm. Appropriate treatment of this injury complex includes

Explanation
Question 10
A 38-year-old man caught his index finger in a volleyball net. He noted an angular deformity of the finger that was reduced when a teammate pulled on his finger. Three weeks later, he now reports trouble extending his finger. A clinical photograph is shown in Figure 55. What anatomic structure is most likely injured?

Explanation
Question 11
A 40-year-old laborer sustains the injury shown in the radiograph and CT scan in Figures 56a and 56b. What is the most common complication associated with surgical intervention?

Explanation
Question 12
A 40-year-old woman sustains a flexion injury to her neck. Physical examination is normal. A lateral radiograph of the cervical spine is shown in Figure 57a. MRI scans of the cervical spine are shown in Figures 57b and 57c. Treatment should include

Explanation
Question 13
Patients in compensated shock (normal vital signs) are thought to be at risk for which of the following?
Explanation
Question 14
A 66-year-old woman was a restrained passenger in an automobile accident. She sustained a direct blow to her nondominant left hand as the airbag in her automobile deployed and she now reports pain, swelling, and difficulty moving her fingers. Radiographs are shown in Figures 58a and 58b. Appropriate definitive treatment should consist of

Explanation
Question 15
A 14-year-old boy sustains a right leg injury after being thrown from his motorcycle while racing. He reports diffuse right leg pain starting at his knee and proceeding distally to include his foot. After the injury the patient's mother reports the tibia moving posteriorly then anteriorly while she was supporting the leg. In the emergency department 4 hours after injury, examination reveals a large knee effusion, firm compartments of the leg, a palpable posterior tibialis pulse with a warm, pink foot, and capillary refill of 2 seconds at the toes. His blood pressure is 100/50 mm Hg. Motor examination is intact, but there is decreased sensation in the dorsal first interspace and plantar aspect of the foot. Compartment pressure measurement reveals all four compartments with pressures of 33, 36, 33, and 38 mm Hg respectively. Radiographs are shown in Figure 59a and 59b. The remainder of the skeletal examination is normal. What is the optimal management for this injury?

Explanation
Question 16
Resuscitation of a trauma patient who has been in hypovolemic shock is complete when which of the following has occurred?
Explanation
Question 17
A 12-year-old girl falls in gymnastics and sustains comminuted midshaft radius and ulna fractures. Closed reduction and cast immobilization are attempted but fracture redisplacement with 20 degrees of angulation occurs. Surgical treatment includes closed reduction and intramedullary fixation of both bones. What is the most common long-term complication for this fracture?
Explanation
Question 18
A 52-year-old woman who is right hand-dominant sustains an injury to her elbow in a fall. A radiograph is shown in Figure 60. The preferred treatment of this injury pattern should include

Explanation
Question 19
The teardrop shape marked with an asterisk in Figure 61 represents what anatomic structure?

Explanation
Question 20
A patient was treated with a revision reamed intramedullary nail for a nonunion 6 months ago. A current radiograph is shown in Figure 62. Based on these findings, what is the most appropriate treatment?

Explanation
Question 21
Figure 63 shows the radiographs of a 23-year-old man who sustained a twisting injury at work. Swelling, tenderness, and ecchymosis are noted about the entire midfoot. What associated injury is most likely to be problematic?

Explanation
Question 22
A 24-year-old man is ejected from his motorcycle and sustains a significant hip injury. The fracture shown in Figures 64a through 64e is best described as what type of fracture?
Explanation
Question 23
A 71-year-old woman who reports long-term use of oral steroids for asthma is referred for treatment of a distal humerus fracture. Radiographs reveal diffuse osteopenia and a severely comminuted intra-articular fracture. What is the most appropriate treatment?
Explanation
Question 24
A 14-year-old boy sustained a 100% displaced distal radius Salter-Harris type II fracture. Neurologic examination demonstrates normal motor examination and two-point discrimination. He undergoes fracture reduction to the anatomic position with the application of a long arm cast. Postreduction he reports increasing hand and wrist pain with diminution of two-point discrimination to 10 mm over the index and middle fingers over the next several hours after surgery. The cast is bivalved and the padding released relieving all external pressure over the arm. Reevaluation reveals increasing sensory deficit over the affected area. What is the next most appropriate management intervention?
Explanation
Question 25
A 25-year-old male polytrauma patient undergoes initial temporary external fixation for a femoral shaft fracture. He is converted to a femoral nail at 7 days. This management can be expected to result in
Explanation
Question 26
A 28-year-old man is involved in a high-speed motor vehicle collision. Radiographs and computed tomography (CT) scan reveal a displaced talar neck fracture with subluxation of the subtalar joint, but an intact tibiotalar joint. According to the Hawkins classification, what is the approximate expected rate of avascular necrosis (AVN) of the talar body for this injury?
Explanation
Question 27
A 45-year-old male presents in hemorrhagic shock following a crush injury. A pelvic binder is applied. Secondary survey reveals blood at the urethral meatus and a high-riding prostate on digital rectal examination. Pelvic radiographs show a displaced pubic symphysis diastasis. Which of the following is the most appropriate next step in the urologic management of this patient?
Explanation
Question 28
A 32-year-old male sustains a closed comminuted tibial shaft fracture. Twelve hours post-injury, he develops increasing pain out of proportion to his injury and severe pain with passive stretch of his toes. You suspect acute compartment syndrome and obtain compartment pressure measurements. Which of the following criteria is generally considered the most reliable threshold for performing a four-compartment fasciotomy?
Explanation
Question 29
A 75-year-old, independently living, highly active community-ambulating female sustains a displaced femoral neck fracture. Compared to treatment with unipolar or bipolar hemiarthroplasty, total hip arthroplasty (THA) for this patient is associated with:
Explanation
Question 30
A 25-year-old multiple trauma patient with a closed head injury (GCS 7), bilateral pulmonary contusions, and bilateral femoral shaft fractures presents to the trauma bay. Initial labs show a lactate of 4.5 mmol/L and a base deficit of -8. After initial fluid resuscitation, his vitals are HR 115 and BP 90/60. What is the most appropriate initial orthopedic management of his bilateral femur fractures?
Explanation
Question 31
Six weeks after undergoing closed reduction and cast application for a nondisplaced distal radius fracture, a 55-year-old woman suddenly loses the ability to actively extend her thumb at the interphalangeal joint. She denies any new trauma. What is the most appropriate definitive management?
Explanation
Question 32
A 40-year-old agricultural worker sustains a Grade IIIb open tibia fracture after his leg is caught in a tractor mechanism, resulting in heavy soil and manure contamination. In addition to a first-generation cephalosporin and an aminoglycoside, what additional intravenous antibiotic coverage is strictly indicated?
Explanation
Question 33
A 22-year-old collegiate football player sustains a violent axial load to a plantar-flexed foot during a tackle.
Weight-bearing radiographs of the foot demonstrate a 3.5 mm diastasis between the base of the first and second metatarsals. There are no associated fractures visible. What is the most appropriate definitive management?

Explanation
Question 34
A 35-year-old male sustains a closed, low-energy transverse fracture of the middle third of the humeral shaft. In the emergency department, he exhibits a complete wrist drop and absent sensation in the first dorsal web space of the hand. His skin is intact. What is the most appropriate initial management of the nerve injury?
Explanation
Question 35
A 28-year-old male sustains a low-velocity civilian gunshot wound to the right thigh, resulting in a comminuted femoral shaft fracture. The bullet passed cleanly through the thigh, leaving isolated 1 cm entry and exit wounds. Examination reveals a neurologically intact extremity with strong distal pulses. Which of the following is the most appropriate management strategy?
Explanation
Question 36
A 45-year-old man sustains an unstable anteroposterior compression (APC-II) pelvic ring injury requiring anterior symphyseal plating. During exposure via a Pfannenstiel approach, brisk arterial bleeding is encountered on the posterior aspect of the superior pubic ramus. Which of the following is the most likely source of this bleeding?
Explanation
Question 37
A 35-year-old man is involved in a high-speed motorcycle collision. Radiographs demonstrate a comminuted bicondylar tibial plateau fracture with metaphyseal-diaphyseal dissociation.
On examination, the leg is extremely tense, and he has agonizing pain with passive extension of the hallux. If a four-compartment fasciotomy of the leg is performed using a standard two-incision technique, which compartment is most at risk for inadequate decompression?

Explanation
Question 38
A 65-year-old woman sustained a supracondylar femur fracture treated with a lateral locked plate. Six months postoperatively, she presents with progressive thigh pain. Radiographs demonstrate a broken plate at the fracture site and a lack of bridging callus. Which technical error during the initial surgery is most strongly associated with this specific mode of implant failure?
Explanation
Question 39
A 28-year-old construction worker sustains a Gustilo-Anderson IIIB open fracture of the middle third of the tibia. After serial debridements, the wound bed is healthy, but there is a 6 cm x 4 cm area of exposed anterior tibia devoid of periosteum. Which of the following soft tissue coverage options is most appropriate for this specific defect?
Explanation
Question 40
A 22-year-old snowboarder sustained a Hawkins type II talar neck fracture treated with open reduction and internal fixation. At his 8-week postoperative visit, an anteroposterior radiograph of the ankle reveals a subchondral radiolucent band in the talar dome. What is the clinical significance of this radiographic finding?
Explanation
Question 41
A 24-year-old man has a displaced waist fracture of the scaphoid.
You plan for percutaneous fixation and request a CT scan to accurately evaluate the fracture morphology and degree of humpback deformity. To optimally visualize the true anatomy, the CT scan images should be reconstructed in which of the following planes?

Explanation
Question 42
A 6-year-old boy sustains a widely displaced, extension-type supracondylar humerus fracture. On presentation, his hand is pink and warm, with a capillary refill of 2 seconds, but the radial pulse is not palpable. Following closed reduction and percutaneous pinning in the operating room, the hand remains pink and well-perfused, but the radial pulse remains absent. What is the most appropriate next step in management?
Explanation
Question 43
A 55-year-old woman sustains a severely displaced 4-part proximal humerus fracture.
When considering the risk of avascular necrosis of the humeral head, which of the following arterial branches provides the predominant blood supply to the articular segment?

Explanation
Question 44
A 25-year-old man presents following a high-speed collision with a closed left femoral shaft fracture, multiple rib fractures, bilateral pulmonary contusions, and a grade III spleen laceration. Initial vitals: BP 85/50 mmHg, HR 120 bpm. Lactate is 4.5 mmol/L. After 2 liters of crystalloid and splenic embolization, his BP is 95/60 mmHg, and repeat lactate is 3.8 mmol/L. What is the most appropriate management of his femur fracture?
Explanation
Question 45
A 30-year-old athlete sustains a supination-external rotation (Weber B) ankle fracture. Intraoperatively, after anatomic fixation of the lateral malleolus, the surgeon utilizes a 'hook test' to assess the integrity of the syndesmosis under fluoroscopy. Which of the following radiographic parameters during the stress maneuver most reliably indicates syndesmotic instability necessitating fixation?
Explanation
Question 46
A 35-year-old male is brought into the trauma bay following a high-speed motor vehicle collision. He is hemodynamically unstable with a blood pressure of 80/50 mmHg. Pelvic compression reveals instability, and an anteroposterior pelvic radiograph demonstrates a wide symphyseal diastasis. An emergency responder placed a pelvic binder in the field.
What is the most common anatomical error in the placement of a circumferential pelvic binder?

Explanation
Question 47
A 30-year-old man is struck by a motor vehicle and sustains a closed Pauwels type III (high shear angle) femoral neck fracture.
To minimize the risk of mechanical failure and nonunion, what is the most biomechanically stable fixation construct for this specific fracture pattern?

Explanation
Question 48
A 25-year-old male is evaluated in the emergency department after sustaining an isolated low-velocity civilian gunshot wound to the right thigh. Radiographs demonstrate a midshaft femur fracture. He is hemodynamically stable, has palpable distal pulses, no sensory deficits, and the entrance and exit wounds are less than 1 cm with minimal contamination. What is the standard of care for definitive management?
Explanation
Question 49
A 28-year-old man sustains an anterior knee dislocation following a motorcycle crash. The knee is successfully reduced in the trauma bay. Distal pulses are palpable and symmetric to the uninjured side. However, an Ankle-Brachial Index (ABI) is measured at 0.8.
What is the most appropriate next step in management?

Explanation
Question 50
A 40-year-old man presents with a closed, highly comminuted midshaft tibia fracture. His blood pressure is 110/70 mmHg. He requires large amounts of analgesics for leg pain and has pain on passive stretch of his toes. His anterior compartment pressure is measured at 45 mmHg. Which of the following statements regarding his diagnosis and management is most accurate?
Explanation
Question 51
A 38-year-old woman falls from a ladder and sustains a complex intra-articular distal femur fracture. CT scanning identifies a Hoffa fracture fragment.
Which of the following statements accurately characterizes this specific injury component?

Explanation
Question 52
A 25-year-old snowboarder sustains a Hawkins Type III fracture of the talar neck after a high-energy landing. Which of the following accurately describes the anticipated rate of avascular necrosis (AVN) of the talar body for this specific injury pattern?
Explanation
Question 53
A 22-year-old collegiate athlete sustains a hyperplantarflexion injury to his midfoot. Weight-bearing radiographs demonstrate widening of the first and second intermetatarsal space with no evidence of fracture on CT.
Based on prospective randomized data, what is the recommended surgical management for this purely ligamentous injury?

Explanation
Question 54
A 19-year-old male is ejected during a motor vehicle rollover. On presentation, his right upper extremity is flail, massively swollen, and pulseless. Chest radiograph shows significant lateral displacement of the right scapula relative to the thoracic spine compared to the uninjured side. The mortality associated with this specific syndrome is most closely tied to which complication?
Explanation
Question 55
A 65-year-old woman underwent volar locking plate fixation for a displaced intra-articular distal radius fracture six months ago.
She presents to the clinic complaining of a sudden inability to actively lift her thumb off the table when the hand is resting flat. Which of the following technical errors during the index procedure is the most likely cause of this complication?
Explanation
Question 56
A 42-year-old man is brought to the emergency department after a high-speed motorcycle collision. His blood pressure is 80/50 mm Hg and heart rate is 120 bpm. Primary survey reveals an unstable pelvis. The trauma team decides to apply a pelvic binder. To be maximally effective in reducing pelvic volume, the binder should be centered over which of the following anatomic landmarks?
Explanation
Question 57
A 72-year-old woman presents with a 3-month history of vague, progressively worsening thigh pain. She denies any recent trauma but has been taking alendronate for the last 8 years. Radiographs reveal cortical thickening of the lateral femoral shaft with a transverse radiolucent line. What is the most appropriate next step in management?
Explanation
Question 58
A 24-year-old man sustains a closed midshaft tibia fracture following a soccer injury and undergoes antegrade intramedullary nailing. Postoperatively, he develops severe leg pain out of proportion to his injury. Passive extension of his great toe elicits excruciating pain. Which of the following compartments is most likely affected?
Explanation
Question 59
A 35-year-old construction worker sustains a severe open tibia fracture with extensive soft tissue stripping and a 12 cm laceration (Gustilo-Anderson Type IIIB). According to current evidence-based guidelines, which of the following is the most critical factor in preventing deep infection?
Explanation
Question 60
A 40-year-old man falls from a height of 15 feet and sustains a highly comminuted, intra-articular distal tibia (pilon) fracture. On presentation, there is severe swelling and hemorrhagic fracture blisters. What is the most appropriate initial management?
Explanation
Question 61
A 28-year-old motorcyclist is struck by a car and thrown 30 feet. He presents with a completely flail, pulseless left upper extremity. Radiographs demonstrate marked lateral displacement of the scapula relative to the thoracic spine and a displaced clavicle fracture. Which of the following associated injuries is responsible for the highest early mortality rate in this condition?
Explanation
Question 62
A 30-year-old man sustains a completely displaced, vertically oriented (Pauwels type III) femoral neck fracture in a motor vehicle accident. He undergoes closed reduction and internal fixation. Which of the following biomechanical constructs provides the most stable fixation for this specific high-shear fracture pattern?
Explanation
Question 63
A 25-year-old snowboarder sustains a displaced talar neck fracture with subluxation of the subtalar joint (Hawkins Type II). He undergoes prompt open reduction and internal fixation. Six weeks later, an AP radiograph of the ankle demonstrates a subchondral radiolucent band in the dome of the talus. What does this radiographic finding indicate?
Explanation
Question 64
A 22-year-old man sustains a low-velocity gunshot wound to the right thigh resulting in a comminuted midshaft femur fracture. The entrance and exit wounds are 1 cm in diameter with no active bleeding or expanding hematoma. His neurovascular examination is entirely intact. What is the most appropriate orthopedic management?
Explanation
Question 65
A 35-year-old man presents with a severe crush injury to his lower leg with a completely ischemic foot. The trauma team is deciding between limb salvage and primary amputation. Which of the following statements regarding the Mangled Extremity Severity Score (MESS) is most accurate according to the Lower Extremity Assessment Project (LEAP) study?
Explanation
Question 66
A 42-year-old man arrives in the emergency department hypotensive and tachycardic following a high-speed motor vehicle collision. A pelvic radiograph reveals an anteroposterior compression (APC) type III pelvic ring injury. A pelvic binder is applied, and a FAST scan is negative for intra-abdominal fluid. Despite fluid resuscitation, he remains hypotensive. What is the most common anatomic source of hemorrhage in this clinical scenario?
Explanation
Question 67
A 28-year-old man sustains a displaced, highly vertical femoral neck fracture (Pauwels III) following a fall from a roof.
Which of the following internal fixation constructs provides the greatest biomechanical stability to resist the high shear forces inherent in this specific fracture pattern?
Explanation
Question 68
A 35-year-old motorcyclist sustains a complex intra-articular fracture of the distal femur. Computed tomography (CT) reveals a coronal plane fracture of the lateral femoral condyle (Hoffa fracture).
What is the optimal method of internal fixation for this specific articular fragment?
Explanation
Question 69
A 40-year-old man falls from a height of 15 feet and presents with a severely swollen leg. Radiographs demonstrate a bicondylar tibial plateau fracture with diaphyseal-metaphyseal dissociation (Schatzker VI).
On physical examination, he has severe pain with passive stretch of his toes and decreased sensation in the first web space. His calf is extremely tense. What is the most appropriate next step in management?

Explanation
Question 70
A 30-year-old man undergoes open reduction and internal fixation for a displaced talar neck fracture (Hawkins type II).
Eight weeks postoperatively, an anteroposterior mortise radiograph of the ankle reveals a subchondral radiolucent band localized to the dome of the talus (Hawkins sign). What does this radiographic finding indicate?
Explanation
Question 71
A 25-year-old man with a closed tibial shaft fracture develops acute compartment syndrome. If left untreated, irreversible muscle necrosis will typically begin to occur after how many hours of continuous ischemia?
Explanation
Question 72
A 65-year-old right-hand-dominant woman is treated nonoperatively in a short arm cast for a nondisplaced distal radius fracture.
Six weeks post-injury, her cast is removed, and she immediately notes an inability to actively extend the interphalangeal joint of her right thumb, with her thumb adopting a dropped posture. What is the most appropriate surgical management?

Explanation
Question 73
A 45-year-old pedestrian is struck by a vehicle and sustains a Gustilo-Anderson Type IIIB open fracture of the distal third of the tibia. Following serial debridements, a clean 6 cm x 4 cm soft tissue defect remains with exposed bone completely devoid of periosteum.
What is the most appropriate method for providing definitive soft tissue coverage for this specific location?

Explanation
Question 74
A 6-year-old boy presents to the emergency department after falling from monkey bars, sustaining a severely displaced, extension-type supracondylar humerus fracture. On initial examination, the radial pulse is absent, but the hand is warm and pink with a capillary refill time of less than 2 seconds. The fracture is taken to the operating room for closed reduction and percutaneous pinning. Postoperatively, the hand remains warm and pink with brisk capillary refill, but the radial pulse remains unpalpable. What is the most appropriate next step in management?
Explanation
Question 75
A 24-year-old collegiate football player presents with severe midfoot pain and inability to bear weight after his foot was axially loaded in plantar flexion. Physical examination reveals midfoot swelling and pathognomonic plantar ecchymosis. Anteroposterior radiographs demonstrate a 'fleck sign' in the space between the medial and middle cuneiforms.
This avulsion fracture indicates disruption of a critical stabilizing ligament. From which anatomical structure does this specific bone fragment typically originate?

Explanation
Question 76
A 28-year-old polytrauma patient presents after a high-speed motor vehicle collision with bilateral femur fractures, a pelvic ring injury, and a grade IV splenic laceration. Following initial damage control surgery and splenectomy, the patient is in the ICU. Which of the following parameters is the most reliable indicator of adequate global tissue perfusion and resuscitation prior to proceeding with definitive orthopedic fixation?
Explanation
Question 77
A 45-year-old man is brought to the emergency department after falling from a 20-foot scaffold. He is hemodynamically unstable with a blood pressure of 80/40 mm Hg. Radiographs reveal an APC-III pelvic ring injury. A pelvic binder is to be applied. What is the most appropriate anatomical landmark for the optimal placement of the pelvic binder to effectively reduce pelvic volume?
Explanation
Question 78
A 22-year-old motorcycle rider is ejected and sustains a massive traction injury to his right upper extremity. Physical examination reveals a completely flail, anesthetic right arm, and severe swelling over the shoulder girdle. Radiographs show significant lateral displacement of the scapula relative to the spinous processes, an intact clavicle, and disruption of the acromioclavicular joint. What is the most likely associated limb-threatening vascular injury?
Explanation
Question 79
A 35-year-old man sustains a completely displaced, vertically oriented (Pauwels Type III) femoral neck fracture after a fall from a roof. Which of the following fixation constructs offers the greatest biomechanical stability and highest rate of union for this specific fracture pattern?
Explanation
Question 80
A 27-year-old man sustains a closed midshaft tibia fracture treated with intramedullary nailing. Postoperatively, he develops severe pain out of proportion to the injury, significantly worsened by passive stretch of the hallux. His blood pressure is 110/70 mm Hg. Intracompartmental pressure monitoring is performed. Which of the following pressure readings most strongly dictates the need for an emergent four-compartment fasciotomy?
Explanation
Question 81
A 30-year-old man presents with a gunshot wound to the distal thigh. He has an expanding hematoma, absent popliteal and pedal pulses, and a comminuted fracture of the distal femoral diaphysis. In the operating room, what is the most appropriate sequence of management?
Explanation
Question 82
A 40-year-old pedestrian is struck by a car and sustains a Gustilo-Anderson Type IIIB open fracture of the distal third of the tibia. Following serial thorough debridement and skeletal stabilization with an external fixator, the wound requires soft tissue coverage. Which of the following is the most appropriate flap option for a large defect over the distal third of the tibia?
Explanation
Question 83
A 25-year-old man falls from a height and sustains a displaced fracture of the talar neck. He undergoes open reduction and internal fixation. At the 8-week postoperative visit, an anteroposterior radiograph of the ankle reveals subchondral radiolucency in the dome of the talus. What does this radiographic finding indicate?
Explanation
Question 84
A 24-year-old professional football player sustains an axial load to a plantar-flexed foot. Radiographs and subsequent MRI confirm a purely ligamentous Lisfranc injury with 3 mm of diastasis between the base of the first and second metatarsals. What is the most appropriate definitive management for this patient?
Explanation
Question 85
An 82-year-old woman with severe osteoporosis falls and sustains a Type II odontoid fracture. She is neurologically intact. Which of the following treatment modalities is associated with the highest rate of morbidity and mortality in this specific patient population, and is therefore generally contraindicated?
Explanation
Question 86
A 35-year-old male sustains a high-energy motor vehicle collision. Radiographs demonstrate a displaced talar neck fracture with subluxation of the subtalar joint (Hawkins type II). Regarding the vascular supply to the talus and the risk of osteonecrosis, which of the following statements is true?
Explanation
Question 87
A 42-year-old construction worker is crushed by a heavy machine. On arrival, his blood pressure is 70/40 mmHg. A FAST examination is positive for intra-abdominal fluid, and a portable pelvic radiograph shows a widened pubic symphysis with disruption of the posterior sacroiliac complex (APC III injury). A commercial pelvic binder is ordered. To optimally reduce the pelvic volume and stabilize the fracture, the binder should be centered over which of the following anatomic landmarks?
Explanation
Question 88
A 45-year-old woman presents to the emergency department after falling on an outstretched hand. She is diagnosed with a 'terrible triad' injury of the elbow. Operative management is planned. According to standard biomechanical principles, which of the following represents the optimal surgical sequence of repair for this injury pattern?
Explanation
Question 89
A 28-year-old male is admitted to the intensive care unit with a closed midshaft tibia fracture and a severe closed head injury. He is intubated and obtunded. His current blood pressure is 110/70 mmHg. Due to a tense leg on examination, intracompartmental pressure monitoring is initiated. Which of the following thresholds is the most widely accepted absolute indication for a four-compartment fasciotomy in this patient?
Explanation
Question 90
A 22-year-old motorcyclist is thrown from his bike at highway speeds. A chest radiograph in the trauma bay reveals lateral displacement of the right scapula and a widely displaced midshaft clavicle fracture. Examination of the right upper extremity shows absent pulses, pallor, and a complete lack of motor and sensory function throughout the limb. Which of the following is the most likely neurologic injury associated with this clinical picture?
Explanation
Question 91
A 38-year-old man sustains a Gustilo-Anderson type IIIB open fracture of the proximal third of the tibia after a severe crush injury. Following aggressive surgical debridement, there is a 6 cm by 5 cm anterior soft-tissue defect exposing bare bone devoid of periosteum. Which of the following is the most appropriate soft-tissue coverage option for this specific anatomic location?
Explanation
Question 92
A 24-year-old man is evaluated in the emergency department for a gunshot wound to the right hip. Plain radiographs demonstrate a retained bullet resting entirely within the intra-articular space of the hip joint. CT imaging confirms the bullet is intracapsular, with no major osseous fracture. Which of the following represents the most appropriate initial management?
Explanation
Question 93
A 65-year-old woman is seen in the outpatient clinic 6 weeks after sustaining a non-displaced distal radius fracture treated with a short arm cast. She now complains of a sudden inability to actively extend the interphalangeal joint of her thumb. She denies any new trauma. What is the most appropriate definitive surgical management for her condition?
Explanation
Question 94
A 30-year-old male sustains a severe midfoot sprain while playing American football. Weight-bearing radiographs demonstrate a 3 mm diastasis between the base of the first and second metatarsals. The primary ligamentous structure injured in this pattern originates from which bone and inserts onto which bone?
Explanation
Question 95
A 42-year-old man sustains a high-energy distal femur fracture. A computed tomography (CT) scan is obtained, revealing a distinct coronal plane fracture of the lateral femoral condyle that was difficult to visualize on plain radiographs. What is the standard eponym for this specific fracture pattern, and how should interfragmentary lag screws generally be oriented for optimal fixation?
Explanation
Question 96
A 45-year-old man sustains a severe closed pilon fracture (OTA 43-C3) after a fall from a ladder. Examination in the emergency department reveals massive soft tissue swelling, fracture blisters, and a shortened extremity. What is the most appropriate initial surgical management?
Explanation
Question 97
A 35-year-old farmer is brought to the trauma bay after his leg was caught in a tractor power take-off. He sustains a grade IIIb open diaphyseal tibia fracture with gross soil and organic matter contamination. In addition to surgical debridement, which of the following is the most appropriate empiric intravenous antibiotic regimen?
Explanation
Question 98
A 28-year-old man sustains a vertically oriented, displaced femoral neck fracture (Pauwels type III) following a high-energy motor vehicle collision. Which of the following internal fixation constructs provides the greatest biomechanical stability for this specific fracture pattern?
Explanation
Question 99
A 30-year-old man who is intubated and sedated in the intensive care unit is noted to have a tense, significantly swollen left lower extremity 24 hours after sustaining a closed, comminuted tibial shaft fracture. Pedal pulses are palpable. What is the most appropriate next step in management?
Explanation
Question 100
A 40-year-old construction worker falls 20 feet from scaffolding, landing on his feet. He sustains bilateral displaced, intra-articular calcaneus fractures. Which of the following is the most common associated skeletal injury in this clinical scenario?
Explanation
None
