AAOS Orthopedic MCQs (Set 3): Long Bone Fractures & Joint Dislocations | 2026 Board Review
Key Takeaway
This high-yield question set (Set 3) for AAOS/ABOS exams focuses on critical orthopedic trauma topics. It covers diagnosis, classification, and management of long bone fractures, common joint dislocations, and essential principles of polytrauma patient care. Prepare effectively for board certification or OITE with these solved MCQs.
AAOS Orthopedic MCQs (Set 3): Long Bone Fractures & Joint Dislocations | 2026 Board Review
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A left-handed 23-year-old man who fell 5 feet from a ladder onto his left elbow sustained the closed injury shown in Figure 26. Management should consist of
Explanation
Question 2
Which of the following is a long-term complication of ankle arthrodesis for posttraumatic arthritis?
Explanation
Question 3
A 19-year-old female long-distance runner has an incomplete tension-side femoral neck stress fracture. Management should consist of
Explanation
Question 4
A 7-year-old girl who sustained a type III posteromedial extension supracondylar fracture underwent a closed reduction at the time of injury. Figure 27a shows the position of the fracture fragments prior to percutaneous medial and lateral pin fixation. Following surgery, healing was uneventful and the patient regained a full painless range of motion. Fifteen months after the injury, she now reports loss of elbow motion and moderate pain with activity. A current AP radiograph is shown in Figure 27b. What is the most likely cause of her symptoms?
Explanation
Question 5
A 55-year-old man sustained an isolated closed fracture of the humerus. Initial neurologic examination reveals no active wrist or finger extension. Radiographs are shown in Figures 28a and 28b. Management should consist of
Explanation
Question 6
Examination of a 41-year-old man who was thrown from a motorcycle reveals that both legs appear externally rotated and there is bruising in the perineal area. He has a blood pressure of 80/40 mm Hg, a pulse rate of 140/min, a respiratory rate of 25/min, and he appears confused. Following administration of 4 L of saline solution and 2 units of packed red blood cells, he has a blood pressure of 80/40 mm Hg, a pulse rate of 160/min, and a respiratory rate of 25/min. The abdominal assessment for intraperitoneal blood is negative. An AP radiograph shows an anteroposterior compression injury with 7 cm of symphysis diastasis but no posterior displacement in the sacroiliac joints. What is the next most appropriate step in management?
Explanation
Question 7
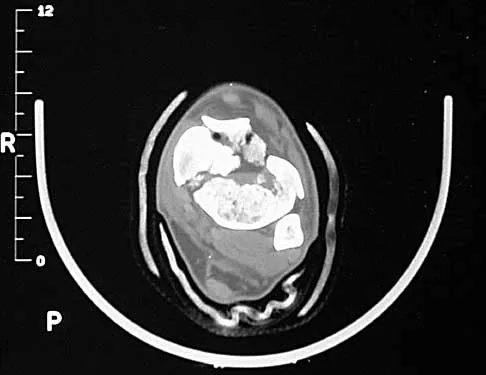
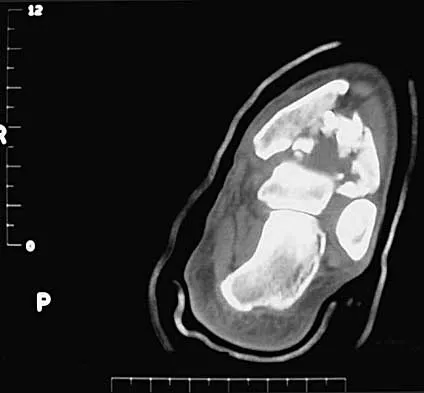
A 32-year-old man sustained a closed injury after falling 25 feet from a roof. His ankle and foot are severely swollen. Radiographs and CT scans are shown in Figures 29a through 29d. Initial management should consist of
Explanation
Question 8
Which of the following parameters is considered most important when assessing an acetabular fracture for surgical indications?
Explanation
Question 9
A 57-year-old man has had right ankle pain for the past 10 months following an injury that went untreated. Radiographs are shown in Figures 30a through 30c. Management should consist of
Explanation
Question 10
A 32-year-old man sustains a forceful inversion injury while playing soccer. Examination reveals tenderness in the lateral hindfoot and midfoot region with associated ecchymosis and swelling. Radiographs show proximal migration of the os peroneum. Active eversion is still present. These findings indicate disruption of the
Explanation
Question 11
A 24-year-old man sustained a grade IIIb open tibial fracture and an ipsilateral grade IIIa femoral fracture in a motorcycle accident. He is unresponsive, intubated, and has a Glasgow Coma Scale score of 8. He is resuscitated and taken to the operating room for definitive orthopaedic care. Which of the following intraoperative problems will most likely adversely affect his long-term outcome?
Explanation
Question 12
Figure 31 shows the radiograph of an 8-year-old boy who has a swollen forearm after falling out of a tree. Examination reveals that all three nerves are functionally intact, and there is no evidence of circulatory embarrassment. Management should consist of
Explanation
Question 13
Figure 32 shows the radiograph of a laborer who jammed his thumb in a fall. Examination reveals pain at the base of the thumb and proximal thenar eminence region. Management should consist of
Explanation
Question 14
In displaced calcaneal fractures, what fragment is the only one that remains in its anatomic position?
Explanation
Question 15
A 46-year-old man sustains a calcaneal fracture in a fall off a scaffold. During surgical reconstruction using an extended lateral incision, the fracture is reduced and fixed with a plate and screws. One of the posterior facet screws is found to be 5 mm out of the bone on the Harris view. What structure is most likely at risk because of this finding?
Explanation
Question 16
A 23-year-old man sustained an injury to his left foot when a forklift rolled over it at work. Examination reveals marked swelling of the midfoot and forefoot, with tenderness to palpation over the medial hindfoot and dorsomedial forefoot. The distal dorsalis pedis pulse is audible on Doppler examination, and his sensation is intact to touch. Radiographs are shown in Figures 33a and 33b. Management should consist of
Explanation
Question 17
A 24-year-old woman who has hypotension, a head injury, and who experienced a poor response to resuscitation has been taken to the operating room for a splenectomy. Following abdominal surgery she remains unstable with increasing pulmonary respiratory pressures and decreasing oxygen saturation. She has a transverse mid-diaphyseal fracture of the tibia with a 4-cm laceration and soil-contaminated muscle in the wound. Based on these findings, management should consist of
Explanation
Question 18
A 53-year-old woman has severe neck and left shoulder pain after a rollover motor vehicle accident. Radiographs and a CT scan of the cervical spine are shown in Figures 34a through 34c. Management should consist of
Explanation
Question 19
What is the most common clinically significant preventable complication secondary to the treatment of a displaced talar neck fracture?
Explanation
Question 20
Examination of a carpenter who hit his thumb with a hammer reveals that the nail plate is broken but in place, and there is a 100% subungual hematoma that covers 100% of the area under the nail plate. Radiographs reveal a comminuted distal phalangeal tuft fracture. Management should consist of
Explanation
Question 21
An olecranon fracture-dislocation of the elbow in which the fracture line exits distal to the coronoid process is best managed by open reduction and
Explanation
Question 22
A 15-year-old baseball pitcher who reports increasing pain in his right shoulder over the past 3 weeks states that the pain increases the more he pitches. Radiographs of both shoulders are shown in Figures 35a and 35b. What is the next most appropriate step in management?
Explanation
Question 23
A 36-year-old man sustains a traumatic spondylolisthesis of L5 on S1. Surgical stabilization requires pedicular fixation into the sacrum. If the screw is placed in a medial to lateral direction and penetrates the sacral ala, what nerve root is at risk?
Explanation
Question 24
A 25-year-old woman who fell on her outstretched hand reports chronic pain over the hypothenar eminence region and some dorsal ulnar wrist pain. She also notes difficulty playing golf and tennis. Plain radiographs of the hand and wrist are unremarkable. A CT scan is shown in Figure 36. What is the next most appropriate step in management?
Explanation
Question 25
An active 72-year-old woman sustained a mid-diaphyseal right humerus fracture 16 months ago. History reveals that she was first treated with a brace for 7 months. Additional treatment consisted of intramedullary nailing 9 months ago. Recently the rod was removed, and the patient now reports pain and gross motion at the fracture site. Current radiographs are shown in Figures 37a and 37b. What is the next most appropriate step in management?
Explanation
Question 26
A 24-year-old man presents with a closed femoral shaft fracture, multiple rib fractures, pulmonary contusions, and an initial Glasgow Coma Scale (GCS) of 6 following a high-speed motor vehicle collision. He is hypotensive in the emergency department and requires vasopressor support. What is the most appropriate management of his femur fracture?
Explanation
Question 27
A 28-year-old man sustains a closed spiral fracture of the distal third of the humerus (Holstein-Lewis fracture). Physical examination reveals an inability to actively extend the wrist or fingers. What is the most appropriate initial management?
Explanation
Question 28
A 32-year-old man sustains a posterior hip dislocation. Following emergent closed reduction, a CT scan reveals a concentric joint space, no intra-articular loose bodies, and a posterior wall fracture involving 15% of the acetabular articular surface. What is the most appropriate definitive management?
Explanation
Question 29
A 28-year-old man sustains a closed midshaft humeral fracture. He presents with a wrist drop and inability to extend his fingers. Radiographs show a transverse midshaft fracture. What is the most appropriate initial management of the nerve injury?
Explanation
Question 30
A 45-year-old polytrauma patient presents with a closed left femoral shaft fracture, multiple rib fractures, and bilateral pulmonary contusions. His serum lactate is 4.5 mmol/L and pH is 7.15. Which of the following is the most appropriate management of his femur fracture?
Explanation
Question 31
A 24-year-old unrestrained driver is involved in a motor vehicle collision. He presents with his right lower extremity positioned in flexion, adduction, and internal rotation.
Which of the following structures is at greatest risk of injury?

Explanation
Question 32
A 65-year-old woman presents with an anterior shoulder dislocation and an associated greater tuberosity fracture. Following closed reduction, radiographs reveal that the greater tuberosity fragment is displaced superiorly by 8 mm. What is the most appropriate next step in management?
Explanation
Question 33
A 32-year-old man undergoes reamed intramedullary nailing for a closed tibial shaft fracture. Postoperatively, he complains of severe leg pain out of proportion to the injury, exacerbated by passive toe stretch. His blood pressure is 130/80 mmHg. What intracompartmental pressure finding definitively confirms acute compartment syndrome?
Explanation
Question 34
A 70-year-old woman on long-term alendronate therapy presents with vague thigh pain. Radiographs demonstrate an incomplete transverse fracture of the lateral cortex of the subtrochanteric femur with localized periosteal thickening.
What is the recommended prophylactic surgical treatment?
Explanation
Question 35
A 25-year-old cyclist falls directly onto his shoulder. Radiographs reveal a midshaft clavicle fracture with 2.5 cm of shortening and complete displacement. Which of the following is an expected outcome if this is treated nonoperatively rather than surgically?
Explanation
Question 36
A 19-year-old athlete sustains a high-energy traumatic knee dislocation that is spontaneously reduced in the emergency department. His ankle-brachial index (ABI) is measured at 0.8. What is the most appropriate next step in management?
Explanation
Question 37
A 7-year-old boy falls on an outstretched hand and sustains a plastic deformation fracture of the proximal ulna with an associated radial head dislocation. Which nerve is most commonly injured in this specific fracture-dislocation pattern?
Explanation
Question 38
A 34-year-old man sustains an isolated, closed, diaphyseal fracture of both the radius and ulna.
What is the preferred definitive management to maximize the restoration of forearm pronation and supination?

Explanation
Question 39
A 40-year-old man presents after a high-energy motor vehicle crash with a distal femur fracture. CT scan reveals a coronal plane fracture of the lateral femoral condyle. What is the optimal fixation strategy for this specific fracture fragment?
Explanation
Question 40
In a subtrochanteric femur fracture, the proximal fragment is typically deformed by specific muscle forces. Which of the following describes the typical position of the proximal fragment and the primary muscle responsible for its flexion?
Explanation
Question 41
A 10-year-old boy presents with knee pain and inability to actively extend his knee after a jumping injury. Radiographs reveal a high-riding patella and a small bony avulsion from the inferior pole of the patella. What is the most appropriate management?
Explanation
Question 42
An 80-year-old woman with a cemented total hip arthroplasty sustains a fall. Radiographs show a periprosthetic fracture around the stem tip. The stem appears loose within the cement mantle, but there is adequate distal bone stock. According to the Vancouver classification, what is the appropriate treatment?
Explanation
Question 43
A 28-year-old polytrauma patient sustains a highly comminuted, closed femoral shaft fracture in a motor vehicle collision. On arrival, he is tachycardic, has an SpO2 of 88% on room air, and exhibits petechiae across his axillae and chest. Which of the following is the most appropriate initial management for his femur fracture?
Explanation
Question 44
A 34-year-old man sustains a transverse midshaft humerus fracture during an arm wrestling match. In the emergency department, he demonstrates an inability to actively extend his wrist or digits. What is the most appropriate initial management?
Explanation
Question 45
A 45-year-old male presents to the emergency department after a seizure with his left arm locked in internal rotation. Radiographs reveal a posterior shoulder dislocation. A subsequent CT scan demonstrates an anteromedial humeral head impression defect involving 45% of the articular surface. What is the most appropriate definitive management?
Explanation
Question 46
The deforming muscular forces acting on a subtrochanteric femur fracture characteristically result in what position of the proximal fragment?
Explanation
Question 47
A 25-year-old man sustains a posterior hip dislocation following a dashboard injury. A closed reduction is performed within 4 hours. Post-reduction CT imaging shows a concentric joint reduction, no intra-articular fragments, and a non-displaced posterior wall fracture involving 10% of the articular surface. What is the most appropriate next step in management?
Explanation
Question 48
A 30-year-old man is brought to the trauma bay after a high-velocity knee injury. Examination reveals a severe posterolateral dislocation with a prominent transverse groove or 'dimple sign' at the medial joint line. Attempted closed reduction is unsuccessful. What is the most likely anatomic reason for the irreducibility?
Explanation
Question 49
A 55-year-old woman presents with severe thigh pain and a low-energy, transverse diaphyseal femur fracture with focal lateral cortical thickening. She has been taking alendronate for 8 years. Which of the following statements regarding her management is most accurate?
Explanation
Question 50
A 22-year-old male sustains a high-energy closed tibial diaphysis fracture. Four hours later, his leg is tense, and he complains of pain out of proportion to the injury. Passive stretch of his hallux elicits excruciating pain. His diastolic blood pressure is 65 mmHg, and his anterior compartment pressure measures 45 mmHg. What is the most appropriate management?
Explanation
Question 51
In a Galeazzi fracture-dislocation, which of the following stabilizing structures is most commonly disrupted, leading to instability of the distal radioulnar joint (DRUJ)?
Explanation
Question 52
A 60-year-old patient sustains a Vancouver type B2 periprosthetic femur fracture around a cemented, polished taper-slip stem. Radiographs demonstrate a loose femoral component but adequate proximal bone stock. What is the gold standard surgical treatment?
Explanation
Question 53
A 66-year-old woman presents with atraumatic thigh pain. She has been taking oral alendronate for 9 years. Radiographs reveal a transverse fracture of the femoral shaft with lateral cortical thickening and a medial cortical spike. What is the most appropriate management of this condition?
Explanation
Question 54
A 24-year-old man sustains a closed spiral fracture of the distal third of the humerus (Holstein-Lewis fracture). Initial examination in the emergency department documents normal wrist and finger extension. Following closed reduction and application of a coaptation splint, the patient immediately develops an inability to extend his wrist and digits. What is the most appropriate next step in management?
Explanation
Question 55
A 30-year-old male sustains an anterior knee dislocation during a sporting event. The joint is reduced in the emergency department. Palpation reveals symmetric pedal pulses, but the measured Ankle-Brachial Index (ABI) is 0.85. What is the most appropriate next step in the management of this patient?
Explanation
Question 56
A 45-year-old woman falls on an outstretched hand and sustains an elbow injury. Imaging confirms a posterior elbow dislocation, a type II coronoid fracture, and a comminuted radial head fracture (the "terrible triad"). During surgical reconstruction, what is the standard recommended sequence of repair?
Explanation
Question 57
A 25-year-old man sustains a subtrochanteric femur fracture. To achieve an anatomic reduction, the surgeon must overcome the deforming forces acting on the proximal fragment. The proximal fragment is typically pulled into which of the following positions, and by which corresponding muscles?
Explanation
Question 58
A 32-year-old man undergoes reamed intramedullary nailing for a closed tibial shaft fracture. Twelve hours postoperatively, he complains of severe leg pain requiring rapidly escalating doses of narcotics. Which of the following is the most objective and definitive threshold indicating the need for emergent fasciotomy?
Explanation
Question 59
A 22-year-old athlete sustains a midfoot injury with severe midfoot pain and plantar ecchymosis. Radiographs reveal widening of the interval between the first and second metatarsal bases. The primary stabilizing ligament disrupted in this classic Lisfranc injury connects which two osseous structures?
Explanation
Question 60
A 28-year-old driver is involved in a motor vehicle collision and sustains a posterior hip dislocation. He presents with a foot drop and decreased sensation over the dorsum of the foot. Following emergent, uneventful closed reduction within 2 hours of injury, the neurologic deficit persists. What is the most appropriate management of this persistent deficit?
Explanation
Question 61
While most middle-third clavicle fractures can be managed nonoperatively, certain clinical and radiographic criteria strictly dictate surgical intervention. Which of the following is an absolute indication for operative fixation of an acute clavicle fracture?
Explanation
Question 62
A 22-year-old man presents with a closed right femoral shaft fracture and a severe closed head injury with a Glasgow Coma Scale (GCS) score of 6. He is hemodynamically labile. According to the principles of Damage Control Orthopedics (DCO), what is the most appropriate initial management of the femur fracture?
Explanation
Question 63
A 35-year-old man undergoes open reduction and internal fixation of a Hawkins Type II talar neck fracture. At 8 weeks postoperatively, an anteroposterior mortise radiograph reveals a subchondral radiolucent band in the dome of the talus (Hawkins sign). What does this radiographic finding indicate?
Explanation
Question 64
A 55-year-old woman sustained a nondisplaced distal radius fracture treated in a short arm cast. Two weeks after the cast was removed (6 weeks post-injury), she notes a sudden inability to actively extend the interphalangeal joint of her thumb. Radiographs confirm the distal radius fracture is healing well in anatomic alignment. What is the most appropriate surgical treatment?
Explanation
Question 65
A 40-year-old man sustains a high-energy trauma resulting in a distal femur fracture. CT imaging reveals a coronal plane fracture of the lateral femoral condyle (Hoffa fracture). What is the optimal surgical approach and fixation strategy for this specific fragment?
Explanation
Question 66
A 21-year-old collegiate rugby player with a history of recurrent anterior shoulder instability undergoes preoperative imaging, which reveals 25% anterior glenoid bone loss and a large, engaging Hill-Sachs lesion. Which of the following procedures is most appropriate to restore stability and prevent recurrence?
Explanation
Question 67
A 29-year-old motorcyclist sustains a completely displaced, closed midshaft femur fracture and a closed midshaft tibia fracture on the same limb (ipsilateral floating knee). Both fractures are amenable to antegrade intramedullary nailing. Which of the following describes the most universally accepted sequence of definitive stabilization?
Explanation
Question 68
A 25-year-old man with a severe closed head injury (GCS 7) and a closed femoral shaft fracture is admitted to the trauma bay. Initial head CT shows cerebral edema with mass effect. Which of the following is the most appropriate initial management of his femur fracture?
Explanation
Question 69
A 34-year-old man sustains an open humeral shaft fracture (Gustilo-Anderson Type II) after a motorcycle collision. Examination reveals a complete inability to extend the wrist and fingers, which was noted immediately after the injury. What is the most appropriate management of the nerve injury?
Explanation
Question 70
During surgical reconstruction for a 'terrible triad' injury of the elbow, what is the recommended sequence of repair to best restore elbow stability?
Explanation
Question 71
A 68-year-old woman on long-term alendronate therapy presents with a low-energy, transverse subtrochanteric femur fracture. Radiographs show lateral cortical thickening and a medial spike. What is the most crucial next step in the workup prior to surgical intervention?
Explanation
Question 72
A 22-year-old football player sustains a high-energy knee injury resulting in a multi-ligamentous knee dislocation. Upon reduction in the emergency department, his pedal pulses are palpable, but his ankle-brachial index (ABI) is 0.8. What is the most appropriate next step in management?
Explanation
Question 73
A 24-year-old male presents with recurrent anterior shoulder instability. Advanced imaging reveals a 30 percent anterior glenoid bone loss and an engaging Hill-Sachs lesion. Which of the following surgical procedures provides the lowest rate of recurrent instability for this patient?
Explanation
Question 74
A 28-year-old man sustains a completely displaced, high-shear vertical femoral neck fracture (Pauwels Type III). Which of the following internal fixation constructs provides the highest biomechanical stability for this fracture pattern?
Explanation
Question 75
A 40-year-old man sustains a Gustilo-Anderson Type IIIB open tibial shaft fracture. Following initial aggressive debridement and stabilization, within what timeframe should definitive soft-tissue coverage ideally be performed to minimize the risk of deep infection?
Explanation
Question 76
A 35-year-old male sustained a closed tibial shaft fracture treated with a reamed intramedullary nail 9 months ago. He presents with persistent weight-bearing pain. Radiographs demonstrate an oligotrophic nonunion at the fracture site without hardware failure. Which of the following is the most appropriate definitive management?
Explanation
Question 77
A 25-year-old male is brought to the emergency department after a high-speed motorcycle collision. He is hemodynamically unstable, intubated for severe bilateral pulmonary contusions, and has bilateral closed femoral shaft fractures. What is the most appropriate initial orthopedic management?
Explanation
Question 78
A 22-year-old professional rugby player presents with recurrent anterior shoulder instability. A 3D CT scan reveals 28% anteroinferior glenoid bone loss. Which of the following is the most appropriate surgical intervention to restore stability?
Explanation
Question 79
A 40-year-old female sustains a high-energy knee dislocation. Following closed reduction, her foot is warm, but the Ankle-Brachial Index (ABI) is calculated to be 0.8. What is the most appropriate next step in management?
Explanation
Question 80
A 30-year-old male sustains a closed midshaft humerus fracture and presents with an immediate, complete radial nerve palsy. The fracture is acceptably reduced and placed in a coaptation splint. If there is no clinical sign of nerve recovery, at what post-injury timeframe is an EMG/NCS most indicated to evaluate for subclinical reinnervation?
Explanation
Question 81
A 35-year-old restrained driver in a motor vehicle collision sustains a traumatic posterior hip dislocation. Following successful closed reduction, the patient exhibits weak ankle dorsiflexion and decreased sensation over the dorsum of the foot. Which nerve division is most commonly injured in this injury pattern?
Explanation
Question 82
A 28-year-old male falls on his outstretched hand and presents with a displaced distal third radial shaft fracture.
After anatomic rigid plate fixation of the radius, how should the distal radioulnar joint (DRUJ) be managed?

Explanation
Question 83
A 72-year-old female on alendronate for 8 years presents with a transverse, minimally displaced subtrochanteric femur fracture after a ground-level fall. Radiographs of the contralateral asymptomatic femur show lateral cortical thickening and a 'beaked' appearance. What is the most appropriate management?
Explanation
Question 84
A 31-year-old pedestrian struck by a vehicle sustains ipsilateral fractures of the femoral and tibial shafts (floating knee). What systemic complication is statistically most associated with this specific injury pattern compared to isolated long bone fractures?
Explanation
Question 85
An 18-year-old male undergoes closed reduction of a both-bone forearm fracture. He develops severe pain out of proportion to the injury and tense compartments, prompting a volar fasciotomy. To adequately decompress the deep volar compartment, which specific fascial structure MUST be released?
Explanation
Question 86
A 65-year-old female sustains a severely displaced 4-part proximal humerus fracture. According to recent quantitative anatomical studies, preservation of which artery is most critical for the primary blood supply to the humeral head?
Explanation
Question 87
A 19-year-old football player complains of dyspnea, dysphagia, and right-sided neck pain after being tackled. Examination reveals a palpable depression at the right medial clavicle.
What is the most appropriate management plan?

Explanation
Question 88
A 24-year-old warehouse worker drops a heavy crate on his midfoot. AP and oblique radiographs are obtained to evaluate for a Lisfranc injury. On a normal anteroposterior (AP) radiograph of the foot, what is the key radiographic parameter that confirms structural integrity of the Lisfranc complex?
Explanation
None
