Surgical Dislocation of the Hip: A Masterclass in Femoroacetabular Impingement Correction

Key Takeaway
This masterclass provides an immersive, step-by-step guide to surgical hip dislocation, a powerful technique for treating complex hip pathologies like femoroacetabular impingement (FAI). We cover detailed anatomy, meticulous patient positioning, granular intraoperative execution, and crucial pearls to ensure successful outcomes while preserving the femoral head's vascularity. Fellows will gain insights into managing cam and pincer lesions.
Comprehensive Introduction and Patho-Epidemiology
Good morning, fellows, and welcome to today’s masterclass. The procedure we are embarking upon today—the surgical dislocation of the hip—is a cornerstone of modern joint-preserving orthopedic surgery. Pioneered and popularized by Reinhold Ganz and his colleagues in Bern, Switzerland, this remarkably versatile and powerful technique grants us unparalleled, direct, 360-degree visualization and access to the entire femoral head and acetabulum. This is not a procedure we undertake lightly; it demands a profound respect for regional vascular anatomy and meticulous surgical execution. However, for complex intra-articular pathology, particularly advanced femoroacetabular impingement (FAI), massive labral tears, extensive chondral injuries, complex reductions of femoral neck fractures, or severe slipped capital femoral epiphysis (SCFE), the open surgical dislocation remains the undisputed gold standard against which all other approaches are measured.
Femoroacetabular impingement, as you are well aware, is a primary biomechanical driver of early degenerative joint disease in active adolescents and young adults. FAI is fundamentally a dynamic conflict, characterized by abnormal, premature contact between the proximal femur and the acetabular rim at terminal ranges of motion—most notably in flexion and internal rotation. This repetitive microtrauma initiates a predictable cascade of labral delamination, chondral shear, and eventual global joint failure. Epidemiologically, we recognize two primary, albeit frequently overlapping, morphological variants: pincer and cam impingement. Pincer impingement occurs secondary to focal or global overcoverage of the acetabular rim (e.g., coxa profunda, acetabular retroversion), which acts as an anvil against the femoral neck during terminal flexion, crushing the intervening labrum. Cam impingement, conversely, is a femoral-sided pathology where an abnormal, aspherical osseous prominence at the femoral head-neck junction acts as a cam, aggressively plunging into the joint and shearing the acetabular cartilage from the subchondral bone. In the vast majority of our clinical presentations, these two forms coexist in a mixed impingement pattern.
While the advent and refinement of hip arthroscopy have revolutionized our field, offering a less invasive avenue for many patients, it is not a panacea. Arthroscopy can sometimes limit our ability to dynamically assess complex hip mechanics in real-time and can be technically prohibitive when addressing massive, multi-planar osseous deformities or addressing severe extra-articular impingement. Anterior approaches without dislocation, similarly, offer limited visualization of the posterior and inferior articular cartilage. Surgical dislocation, however, circumvents these limitations entirely. It allows for a thorough, unrestricted dynamic assessment of motion intraoperatively, ensuring we definitively re-establish proper sphericity of the femoral head and adequate head-neck offset.
Furthermore, despite historical trepidation regarding open hip surgery, the morbidity associated with the Ganz surgical dislocation is surprisingly low when executed correctly. The historical fear of iatrogenic avascular necrosis (AVN) of the femoral head—once the bane of open hip procedures—has been virtually eliminated. With rigorous adherence to the anatomical principles we will discuss today, the blood supply to the femoral head is meticulously protected, making AVN an exceptionally rare complication in the modern era of joint preservation.
Detailed Surgical Anatomy and Biomechanics
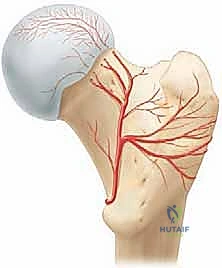
Before a scalpel even touches the skin, a profound, three-dimensional understanding of the regional anatomy is absolutely paramount. The entire conceptual framework of the surgical dislocation hinges upon one critical objective: the absolute preservation of the vascular supply to the femoral head. The dominant arterial contribution to the adult femoral head is derived from the medial femoral circumflex artery (MFCA).
The MFCA typically originates from the deep femoral artery (profunda femoris) and courses posteriorly, navigating between the iliopsoas and pectineus. Its deep branch is the vessel of paramount importance to us today. This deep branch travels posteriorly along the inferior border of the obturator externus tendon, passing anterior to the quadratus femoris. It then crosses the posterior aspect of the femoral neck, deep to the conjoint tendon of the short external rotators, before piercing the joint capsule near the superior gemellus and obturator internus to become the retinacular vessels. These terminal retinacular branches traverse the superior and posterosuperior femoral neck within the synovial folds to supply the weight-bearing dome of the femoral head. These branches are exquisitely vulnerable during the posterior limb of any capsulotomy and during the dislocation maneuver itself.
The genius of the Ganz trochanteric flip osteotomy lies in its elegant exploitation of this anatomy to protect the blood supply. By performing a digastric osteotomy of the greater trochanter—leaving the gluteus medius and minimus attached proximally, and the vastus lateralis attached distally—we maintain a continuous muscular sleeve. Crucially, the intact short external rotator muscles, most notably the obturator externus muscle and the quadratus femoris, act as a dynamic, protective soft-tissue hinge. They form a protective sheath over the MFCA as it wraps around the posterior aspect of the femoral neck, shielding the vessel from tension and direct trauma during anterior dislocation of the femoral head.
Navigating the muscular intervals requires precision. We typically utilize the Gibson approach, exploiting the interval between the gluteus maximus and the gluteus medius.
* Gluteus Maximus: The largest and most superficial gluteal muscle. The Gibson approach preserves the integrity of the gluteus maximus, generally resulting in less postoperative hip extensor dysfunction compared to the muscle-splitting Kocher-Langenbeck approach, though it demands meticulous retraction to achieve adequate anterior exposure.
* Gluteus Medius and Minimus: These primary abductors are critical for pelvic stability. The gluteus medius inserts onto the lateral and superoposterior facets of the greater trochanter, while the minimus inserts more anteriorly. We will elevate a specific osseous wafer containing these insertions during our osteotomy.
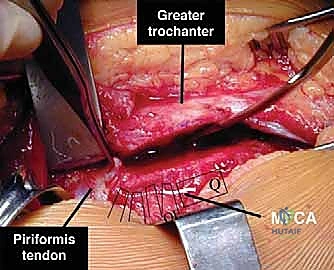
* Piriformis: Originating from the anterior sacrum, this tendon inserts onto the superior aspect of the greater trochanter. It is a crucial anatomical landmark. In the classic Ganz osteotomy, the piriformis tendon remains attached to the stable, intact trochanteric bed, ensuring the posterosuperior capsular vascular network remains undisturbed.
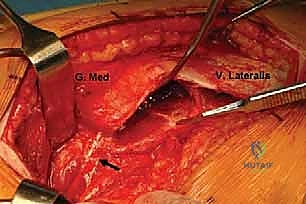
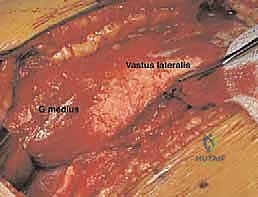
* Vastus Lateralis: Originating from the greater trochanter and linea aspera, its proximal fascia and fibers are reflected anteriorly, maintaining continuity with the gluteus medius via the osteotomized trochanteric fragment.
Biomechanically, we must understand the osteology we are altering. The greater trochanter osteotomy creates a precise wafer (typically 1.5 cm thick), mobilizing the abductor mechanism. The femoral head-neck junction, the frequent site of cam impingement, will be exposed, allowing us to re-establish the normal concavity and offset. The acetabular rim, the site of pincer impingement, will be fully visualized, allowing for precise rim trimming and labral refixation.
Exhaustive Indications and Contraindications
The decision to proceed with a surgical dislocation must be predicated on strict clinical and radiographic criteria. While highly effective, it is an extensive open procedure that should be reserved for pathology that cannot be adequately or safely addressed via arthroscopy or an anterior mini-open approach.
Indications
Surgical dislocation is primarily indicated for complex, multi-planar deformities of the proximal femur and acetabulum. Severe cam lesions that extend far posteriorly or laterally, beyond the safe reach of an arthroscope, are prime indications. Global pincer impingement, such as severe coxa profunda or protrusio acetabuli requiring extensive rim reduction (often exceeding 5-7 mm) and complex labral reconstruction, benefits immensely from the 360-degree visualization afforded by this approach. Furthermore, pediatric and adolescent deformities, including severe slipped capital femoral epiphysis (SCFE) requiring an Imhäuser osteotomy or direct subcapital realignment, and complex Legg-Calvé-Perthes disease sequelae (e.g., coxa magna, hinge abduction), are classic indications. In orthopedic trauma, Pipkin fractures (femoral head fractures associated with posterior hip dislocations) and highly comminuted femoral neck fractures frequently necessitate surgical dislocation for anatomical reduction and stable fixation. Finally, the approach is invaluable in orthopedic oncology for the en bloc excision of benign or low-grade malignant intra-articular tumors (e.g., synovial chondromatosis, pigmented villonodular synovitis).
Contraindications
Contraindications are equally critical to recognize to prevent catastrophic failures. Advanced osteoarthritis is an absolute contraindication; patients with Tönnis grade 3 changes, or those with less than 2 mm of remaining joint space on weight-bearing radiographs, will inevitably fail joint preservation and should be directed toward total hip arthroplasty (THA). Severe osteopenia or osteoporosis precludes the safe execution and subsequent fixation of the trochanteric flip osteotomy. Active local or systemic infection is an absolute contraindication to any elective joint preservation surgery. High-riding developmental dysplasia of the hip (DDH) is a relative contraindication for isolated surgical dislocation; addressing the impingement without correcting the underlying severe dysplasia via a periacetabular osteotomy (PAO) will rapidly accelerate joint degeneration.
| Category | Specific Conditions |
|---|---|
| Primary Indications | Severe/Posterior Cam FAI, Protrusio Acetabuli, Complex SCFE (Subcapital Realignment), Perthes Deformities (Coxa Magna), Pipkin Fractures, Synovial Chondromatosis. |
| Relative Indications | Moderate FAI with massive labral tears requiring complex reconstruction, isolated anterior femoral neck cysts, hardware removal from previous pediatric hip surgeries. |
| Absolute Contraindications | Advanced Osteoarthritis (Tönnis Grade 3), Joint space < 2mm, Active Infection, Severe Osteoporosis, Charcot Arthropathy. |
| Relative Contraindications | Severe DDH without planned PAO, Morbid Obesity (BMI > 40), Heavy smoking (high risk of trochanteric non-union), Uncontrolled Diabetes Mellitus. |
Pre-Operative Planning, Templating, and Patient Positioning
Preoperative planning is not merely a formality; it is a meticulous, highly structured roadmap for the surgery. A successful surgical dislocation begins weeks before the patient enters the operating theater. We must thoroughly review all imaging studies to decode the specific pathoanatomy and template our osseous resections.
Imaging Review: Decoding the Deformity
Our radiographic workup is exhaustive. We always begin with high-quality plain radiographs. An AP view of the pelvis provides a global assessment of acetabular coverage (lateral center-edge angle, Tönnis angle), version (crossover sign, ischial spine sign), and joint space narrowing.

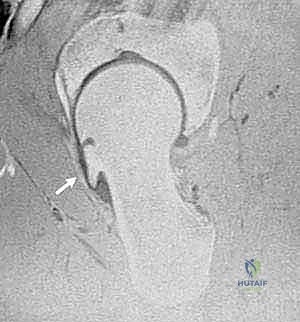
Equally critical is the true lateral view of the hip (or a Dunn 45-degree flexion view), taken in 15 to 20 degrees of internal rotation. This specific projection is crucial for appreciating the lack of anterior femoral head-neck offset, the hallmark of cam impingement. Notice the diminished offset and the osseous prominence encroaching on the normal concavity.

Advanced cross-sectional imaging is mandatory. Computed Tomography (CT) Scans, particularly with two- and three-dimensional reconstructions, are invaluable. CT allows us to precisely quantify femoral version (which dictates how much internal rotation is required to clear an anterior cam lesion) and meticulously map the extent of the osseous prominence.


These 3D reconstructions serve as our intraoperative blueprint, clearly delineating the "bumps" obscuring the anterior femoral head-neck junction and correlating perfectly with the lack of offset seen on plain films.
Finally, Magnetic Resonance Imaging (MRI), ideally a high-resolution MR arthrogram utilizing gadolinium with radial sequences centered on the femoral neck axis, is essential. This modality delineates labral tears, paralabral cysts, and the precise depth and area of chondral delamination, allowing us to anticipate the extent of intra-articular soft-tissue work required.
Patient Positioning: Precision is Key
Once general anesthesia and profound muscle relaxation are achieved, patient positioning must be executed flawlessly. We perform a final, dynamic examination under anesthesia to confirm our preoperative range of motion deficits, noting the exact degree of flexion and internal rotation where impingement occurs.
The patient is then carefully transitioned into the full lateral decubitus position on a specialized radiolucent pegboard.


The pelvis must be strictly perpendicular to the floor. We secure the patient firmly using anterior and posterior pegs to prevent any pelvic roll during the forceful dislocation maneuver. A flat-top cushion with a half-moon-shaped cutout is placed beneath the operative leg, providing crucial stability during the initial approach.

Before final prepping and draping, it is absolutely critical to verify that the operative leg can be fully flexed, adducted, and externally rotated without being obstructed by the anterior inferior peg or the table attachments. This unrestricted freedom of movement is the mechanical prerequisite for a safe dislocation.

A specialized hip drape featuring a sterile, waterproof side bag (or "pouch") is utilized. This bag captures the leg, maintaining strict sterility while allowing the assistant to freely manipulate the limb through extreme ranges of motion during the dislocation and subsequent reduction.
Step-by-Step Surgical Approach and Fixation Technique
Alright, fellows, the patient is prepped, draped, and optimally positioned. Let us walk through the surgical masterclass step-by-step.
Incision and Superficial Dissection
We begin with a straight, longitudinal lateral incision, approximately 15 to 20 centimeters in length. The incision is meticulously centered over the greater trochanter, specifically aligned with the junction between its anterior and middle thirds.

We carry the dissection sharply through the subcutaneous fat down to the fascia lata. Hemostasis is maintained meticulously to preserve visualization.
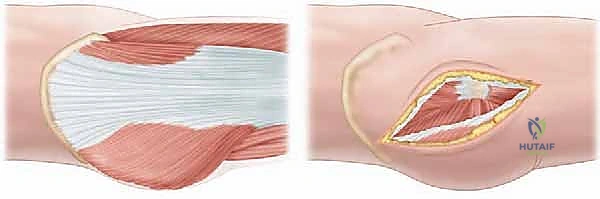
The fascia lata is then incised in line with the skin incision. Proximally, we carefully split the fascia in the direction of its fibers, aiming slightly posterior to access the Gibson interval—the avascular plane between the anterior border of the gluteus maximus and the posterior border of the gluteus medius.
Using blunt dissection and Charnley retractors, we mobilize the gluteus maximus posteriorly. This exposes the underlying abductor mechanism (gluteus medius) and the vastus lateralis distally.
The Trochanteric Flip Osteotomy
We now identify the precise boundaries for our trochanteric osteotomy. We must identify the posterior border of the gluteus medius and the anterior border of the piriformis tendon.
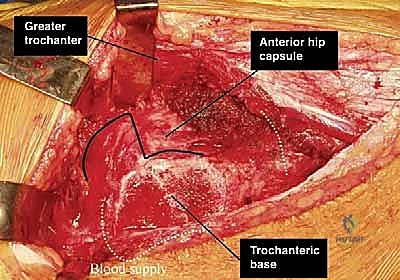
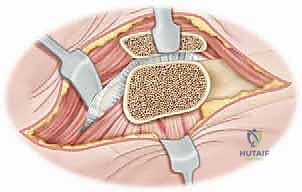
The osteotomy line is marked. It begins posterosuperiorly, just anterior to the insertion of the piriformis tendon, and extends distally to the vastus lateralis ridge. The goal is to create a trochanteric wafer approximately 1.5 cm thick at its maximum depth.
Using an oscillating saw, the osteotomy is performed from posterior to anterior. It is critical to angle the blade slightly laterally to avoid violating the trochanteric fossa, as plunging medially here risks catastrophic injury to the deep branch of the MFCA.
Once the osteotomy is complete, the trochanteric fragment, with the gluteus medius and vastus lateralis firmly attached, is mobilized and flipped anteriorly. We release the underlying gluteus minimus from the capsule to allow full anterior translation of the digastric muscle flap.
Capsulotomy and Dislocation
With the abductors reflected, the superior and anterior hip capsule is broadly exposed. We identify the interval between the piriformis and the gluteus minimus.
We perform a Z-shaped capsulotomy (for a right hip, or an inverse Z for a left hip). The longitudinal limb runs along the anterosuperior axis of the femoral neck. The crucial step is the posterior limb of the capsulotomy. It must remain anterior to the lesser trochanter and the trochanteric crest to definitively avoid the retinacular vessels traversing posterosuperiorly.

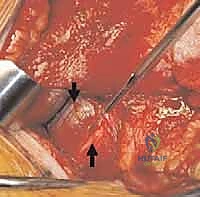
Once the capsule is opened and tagged, we proceed with the dislocation maneuver. This is a coordinated effort. The assistant places the leg into a position of flexion, adduction, and progressive external rotation. Concurrently, a bone hook is placed around the inferior femoral neck to gently lever the head out of the acetabulum. The ligamentum teres is sharply transected as it comes into view.

Intra-Articular Pathology Correction
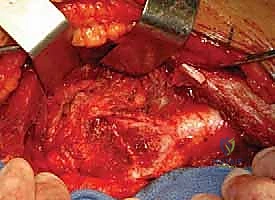
The hip is now fully dislocated anteriorly, providing spectacular, 360-degree access. We inspect the femoral head for chondral damage and meticulously map the cam lesion.

Using a high-speed burr and curved osteotomes, we perform the femoral osteochondroplasty. We resect the aspherical prominence, restoring the normal concavity of the anterior and anterolateral head-neck junction. We utilize spherical templates to guarantee a perfect contour and avoid over-resection, which could compromise the mechanical integrity of the femoral neck.

Attention is then turned to the acetabulum. We address any pincer impingement by carefully trimming the osseous rim using a burr, taking care to preserve the labrum whenever possible. If the labrum is detached or torn, we perform a robust repair or reconstruction using suture anchors placed along the newly contoured acetabular rim.
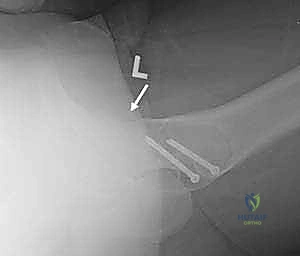
Reduction and Fixation
Following thorough irrigation to remove all osseous debris, the hip is gently reduced by reversing the dislocation maneuver (internal rotation, abduction, and extension).

We perform a dynamic examination, moving the hip through a full range of motion to confirm that the impingement has been completely eradicated and that the labral seal is re-established. The capsule is then meticulously closed, taking care not to plicate it too tightly, which could restrict motion. Finally, the trochanteric flip osteotomy is anatomically reduced and rigidly fixed. We typically utilize two or three 4.5 mm fully threaded cortical screws, directed medially and slightly proximally to engage the dense bone of the lesser trochanteric region.
